Second-Line Treatment Strategies for Right-Sided, RAS/RAF Wild-Type Colorectal Cancer
Nishwant Swami, Wei-Ting Hwang, Ronac Mamtani, Mark H. O’Hara, William J. Chapin

TL;DR
The study compares two treatment options for a specific type of colorectal cancer based on tumor location and genetic status.
Contribution
The paper introduces a comparative analysis of second-line therapies for RAS/RAF wild-type, right-sided colorectal cancer.
Findings
Anti-vascular endothelial growth factor therapy is evaluated against anti-epidermal growth factor receptor therapy.
The study focuses on effectiveness in second-line treatment for a specific subset of colorectal cancer patients.
Abstract
This comparative effectiveness study investigates anti–vascular endothelial growth factor vs anti–epidermal growth factor receptor therapy in second-line treatment among patients with RAS/RAF wild-type, right-sided cancer.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Patients, No. (%) | ||
|---|---|---|---|
| Total cohort (N = 444) | Anti-VEGF therapy (n = 269) | Anti-EGFR therapy (n = 175) | |
| Age, median (IQR), y | 65 (56-72) | 65 (56-72) | 65 (56-71) |
| Gender | |||
| Women | 175 (39.4) | 105 (39.0) | 70 (40.0) |
| Men | 269 (60.6) | 164 (61.0) | 105 (60.0) |
| ECOG performance status category | |||
| 0-1 | 390 (87.8) | 243 (90.5) | 147 (84.1) |
| ≥2 | 54 (12.2) | 26 (9.5) | 28 (15.9) |
| MMR or MSI status | |||
| MMR proficient, MSS, or both | 422 (95.1) | 256 (95.4) | 166 (94.6) |
| MMR deficient, MSI high, or both | 22 (4.9) | 12 (4.6) | 10 (5.4) |
| CEA within 30 d of index date, median (IQR) | 23 (6.3-89.1) | 21.8 (6.1-80.4) | 25.4 (6.5-111.9) |
| Duration of first-line treatment, median (IQR), d | 309 (181-510) | 309 (182-510) | 308 (176-517) |
| Timing of metastasis | |||
| Synchronous | 330 (74.3) | 206 (76.8) | 124 (70.5) |
| Metachronous | 114 (25.7) | 62 (23.2) | 52 (29.5) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Colorectal Cancer Treatments and Studies · Colorectal and Anal Carcinomas
Introduction
For patients with metastatic colorectal cancer (mCRC) that is wild type for KRAS, NRAS, and BRAF (RAS/RAF), treatment includes fluoropyrimidine-based chemotherapy with anti–vascular endothelial growth factor (VEGF) or anti–epidermal growth factor receptor (EGFR) targeted therapy. The PARADIGM trial confirmed that primary tumor sidedness was a predictive biomarker for patients with RAS/RAF wild-type disease and showed no overall survival (OS) benefit from first-line chemotherapy plus anti-EGFR therapy compared with chemotherapy plus anti-VEGF therapy for patients with right-sided tumors.^1,2^ However, to our knowledge, there are no prospective data to guide second-line treatment in this population.^3^ Despite limited evidence, national guidelines recommend anti-EGFR therapy for patients with RAS/RAF wild-type, right-sided cancer who did not receive it previously.^4^ To better inform practice, we compared the effectiveness of second-line chemotherapy plus anti-EGFR vs chemotherapy plus anti-VEGF therapy for patients with RAS/RAF wild-type, right-sided mCRC who received first-line chemotherapy plus anti-VEGF.
Methods
This comparative effectiveness study was exempted from review by the institutional review board at the University of Pennsylvania by meeting 45 CFR §46.104, category 4. It is reported following the ISPOR reporting guideline. We used the nationwide, longitudinal Flatiron Health electronic health record–derived database, comprising deidentified, patient-level structured and unstructured data curated via technology-enabled abstraction from approximately 280 cancer clinics (approximately 800 care sites), most being community oncology settings.^5,6^ Data are deidentified and subject to obligations to prevent reidentification and protect patient confidentiality. Patients 18 years or older with RAS/RAF wild-type, right-sided mCRC who received first-line therapy of chemotherapy plus anti-VEGF and second-line therapy with anti-VEGF therapy (bevacizumab or its biosimilars, ziv-aflibercept, or ramucirumab) or anti-EGFR therapy (cetuximab or panitumumab) between January 2013 and May 2024 were eligible (eMethods in Supplement 1). Multiple imputation with chained equations (MICE) imputed missing values for tumor sidedness, RAS/RAF status, and propensity score model covariates (age, gender, year of diagnosis, synchronous or metachronous metastases, mismatch repair and microsatellite instability status, performance status, carcinoembryonic antigen level, and duration of first-line therapy) (eMethods and eTable in Supplement 1). After MICE, we used Cox proportional hazards modeling with stabilized inverse probability of treatment weighting (IPTW) to assess the adjusted association of anti-EGFR vs anti-VEGF–containing treatment with OS using Stata/SE statistical software version 18.5 (StataCorp) (eMethods, eFigure 1, and eFigure 2 in Supplement 1). A 2-sided P < .05 was considered statistically significant.
Results
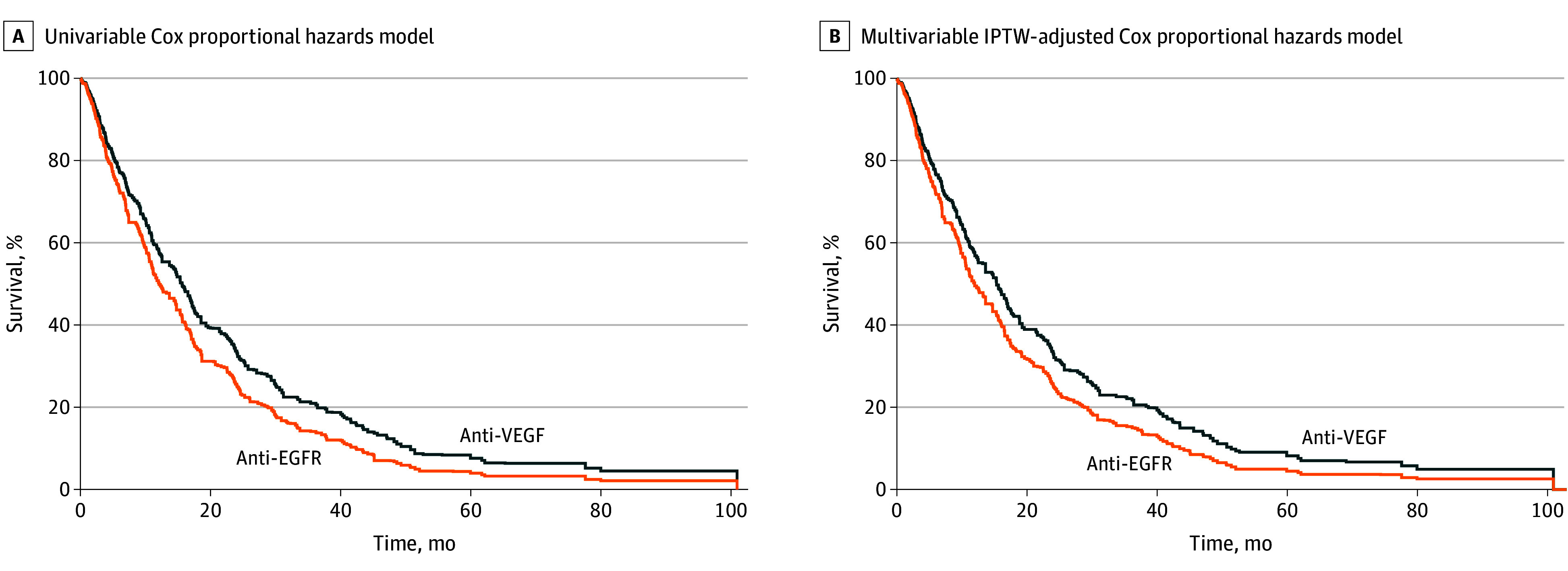
A total of 4444 patients received first-line therapy plus anti-VEGF therapy and second-line anti-VEGF or anti-EGFR therapy with chemotherapy; data were missing for 709 patients (16.0%) on tumor sidedness and 993 patients (22.3%) on RAS/RAF status. Across 25 imputations, a mean of 444 patients (median [IQR] age, 65 [56-72] years; 175 women [39.4%]) met inclusion criteria; 269 patients received anti-VEGF therapy, and 175 patients received anti-EGFR therapy (Table). After IPTW, baseline characteristics were well balanced between treatment groups. Patients who received chemotherapy plus anti-EGFR therapy did not have a significantly increased hazard of death compared with patients who received chemotherapy plus anti-VEGF therapy (hazard ratio, 1.24; 95% CI, 0.96-1.61; P = .10) (Figure). The estimated median survival from the IPTW-adjusted Cox proportional hazards model was 15.3 months (95% CI, 12.5-17.1 months) among patients with chemotherapy plus anti-VEGF therapy and 12.0 months (95% CI, 9.8-15.3 months) among those receiving chemotherapy plus anti-EGFR therapy.
Estimated Survival FunctionsEstimated survival functions were generated independently for each of 25 imputations, with the mean subsequently calculated at each time interval to generate the estimated survival function after multiple imputation. Because the plot represents means of estimated survival functions and not directly observed data, the number at risk at each time are not provided. Estimated median survival was 15.6 months (95% CI, 12.5-17.1 months) in unadjusted and 15.3 months (95% CI, 12.5-17.1 months) in adjusted analysis for patients treated with anti–vascular endothelial growth factor (VEGF) therapy and 12.0 months (95% CI, 9.8-15.3 months) in unadjusted and 12.1 months (95% CI, 10.5-15.3 months) in adjusted analysis for patients treated with anti–epidermal growth factor receptor (EGFR) therapy. IPTW indicates stabilized inverse probability of treatment weights.
Discussion
Among patients with RAS/RAF wild-type, right-sided mCRC who received first-line chemotherapy plus anti-VEGF therapy, this comparative effectiveness research’s findings provide some evidence for continuing anti-VEGF therapy in the second line, although the result was not statistically significant. Our findings corroborate outcomes in first-line therapy from the PARADIGM trial, where nonsignificantly worse OS was observed in patients with right-sided disease receiving anti-EGFR compared with anti-VEGF therapy (hazard ratio, 1.09; 95% CI, 0.79-1.51).^1^ Limitations include possible unmeasured confounding and limited power given the relatively small proportion of mCRC that is right sided and RAS/RAF wild type. Future studies should explore better predictive biomarkers for anti-EGFR vs anti-VEGF treatment in this population to identify patients most likely to benefit from anti-EGFR therapy at any time during their disease course.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Watanabe J, Muro K, Shitara K, . Panitumumab vs bevacizumab added to standard first-line chemotherapy and overall survival among patients with RAS wild-type, left-sided metastatic colorectal cancer: a randomized clinical trial. JAMA. 2023;329(15):1271-1282. doi:10.1001/jama.2023.4428 37071094 PMC 10114040 · doi ↗ · pubmed ↗
- 2Tejpar S, Stintzing S, Ciardiello F, . Prognostic and predictive relevance of primary tumor location in patients with RAS wild-type metastatic colorectal cancer: retrospective analyses of the CRYSTAL and FIRE-3 trials. JAMA Oncol. 2017;3(2):194-201. doi:10.1001/jamaoncol.2016.3797 27722750 PMC 7505121 · doi ↗ · pubmed ↗
- 3Bennouna J, Sastre J, Arnold D, ; ML 18147 Study Investigators. Continuation of bevacizumab after first progression in metastatic colorectal cancer (ML 18147): a randomised phase 3 trial. Lancet Oncol. 2013;14(1):29-37. doi:10.1016/S 1470-2045(12)70477-1 23168366 · doi ↗ · pubmed ↗
- 4Benson AB, Venook AP, Adam M, . Colon cancer, version 3.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2024;22(2 D):e 240029. doi:10.6004/jnccn.2024.002938862008 · doi ↗ · pubmed ↗
- 5Ma X, Long L, Moon S, Adamson BJS, Baxi SS. Comparison of population characteristics in real-world clinical oncology databases in the US: Flatiron Health, SEER, and NPCR. med Rxiv. Preprint posted online June 7, 2023. doi:10.1101/2020.03.16.20037143 · doi ↗
- 6Birnbaum B, Nussbaum N, Seidl-Rathkopf K, Model-assisted cohort selection with bias analysis for generating large-scale cohorts from the EHR for oncology research. ar Xiv. Preprint posted online January 13, 2020. doi:10.48550/ar Xiv.2001.09765 · doi ↗