Real‐World Impact of Steerable Sheaths for Paroxysmal Atrial Fibrillation Catheter Ablation: The INSIGHT Study
Yasuo Okumura, Tsunesuke Kono, Akira Mizukami, Osamu Inaba, Yuji Wakamatsu, Daisuke Yamagishi, Satoshi Nakamura, Takumi Arashiro, Akira Sato, Yi Wang, Atsushi Kobori

TL;DR
The VIZIGO sheath reduces fluoroscopy time and dose during heart procedures for atrial fibrillation without affecting safety or effectiveness.
Contribution
Real-world evidence showing the VIZIGO sheath improves procedural efficiency in paroxysmal atrial fibrillation ablation.
Findings
VIZIGO sheath significantly reduced fluoroscopy time and dose compared to non-steerable sheaths.
Procedural times for PVI isolation were shorter with the VIZIGO sheath.
Acute and long-term effectiveness and safety were comparable between the two sheath types.
Abstract
In atrial fibrillation (AF) ablation procedures, the CARTO VIZIGO Bidirectional Guiding Sheath has previously shown promising results in reducing fluoroscopy times without compromising clinical effectiveness or safety compared with non‐steerable sheaths. This non‐randomized, multicenter, retrospective cohort study (INSIGHT) aimed to determine the real‐world impact of the VIZIGO sheath on procedural efficiency, clinical effectiveness, and safety in paroxysmal AF (PAF) catheter ablation. Consecutive adults who underwent de novo radiofrequency (RF) ablation for PAF with a non‐VIZIGO sheath (January 2019–July 2021) or VIZIGO sheath (January 2020–July 2021) were included. Procedural characteristics, primary adverse events (PAEs), and 12‐month effectiveness (freedom from repeat ablation or recurrent atrial arrhythmia) were evaluated. Of 199 patients included (mean age, 69.7 years; 59.3%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
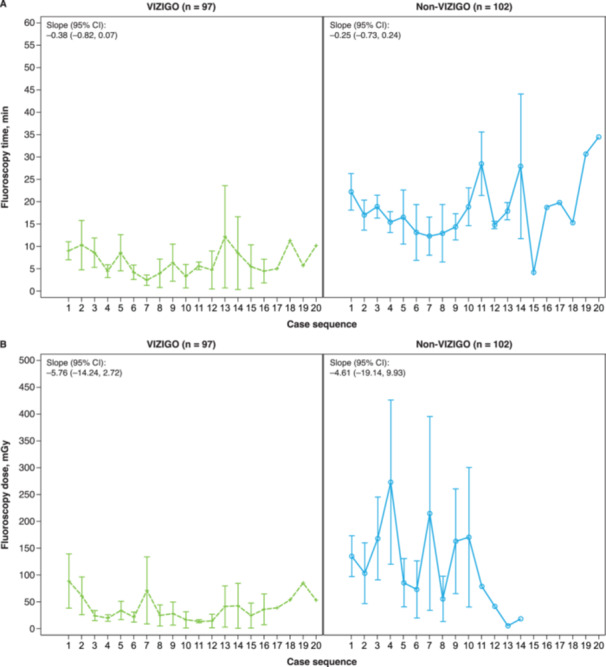 Figure 1
Figure 1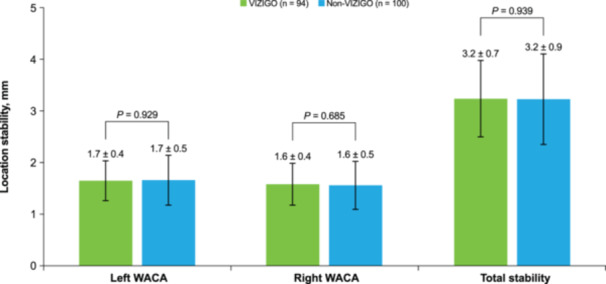 Figure 2
Figure 2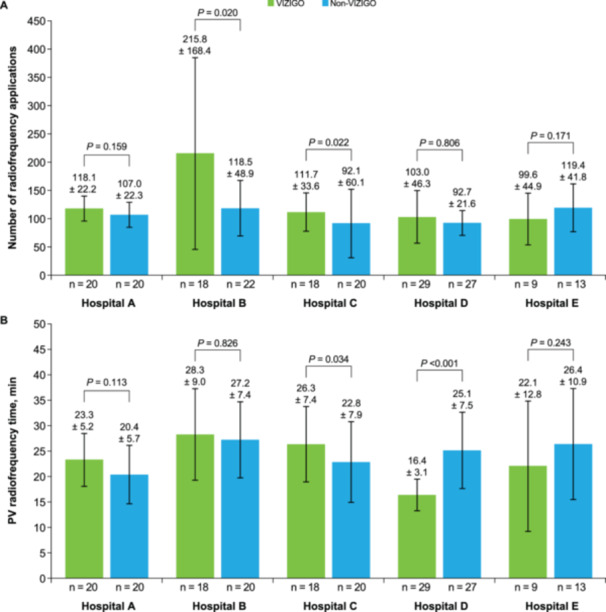 Figure 3
Figure 3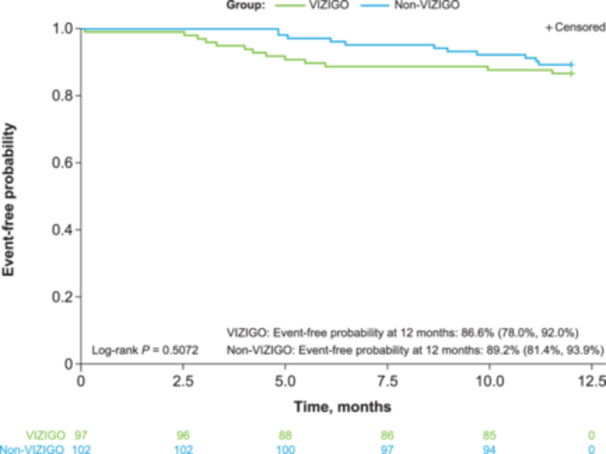 Figure 4
Figure 4| Characteristics | All ( | VIZIGO ( | Non‐VIZIGO ( |
|
|---|---|---|---|---|
| Age, years, mean ± SD | 69.7 ± 10.1 | 69.3 ± 11.1 | 70.1 ± 9.0 | 0.936 |
| Male sex, | 118 (59.3) | 59 (60.8) | 59 (57.8) | 0.773 |
| Weight, kg, mean ± SD | 63.6 ± 12.3 | 63.6 ± 10.4 | 63.5 ± 13.8 | 0.727 |
| Height, cm, mean ± SD | 161.9 ± 10.3 | 162.5 ± 9.4 | 161.4 ± 11.0 | 0.464 |
| BMI, kg/m2, mean ± SD | 24.1 ± 3.5 | 24.1 ± 3.4 | 24.2 ± 3.7 | 0.465 |
| Left ventricular ejection fraction, %, mean ± SD | 63.5 ± 11.4 | 64.08 ± 9.6 | 63.03 ± 12.9 | 0.830 |
| Left atrial diameter, mm, mean ± SD | 39.16 ± 6.5 | 38.42 ± 6.7 | 39.87 ± 6.2 | 0.075 |
| CHA2DS2‐VASc score, mean ± SD | 2.9 ± 1.8 | 2.7 ± 1.8 | 3.1 ± 1.8 | 0.188 |
| Comorbidity, | ||||
| Hypertension | 123 (61.8) | 54 (55.7) | 69 (67.6) | 0.108 |
| Diabetes | 32 (16.1) | 12 (12.4) | 20 (19.6) | 0.181 |
| Congestive heart failure | 33 (16.6) | 16 (16.5) | 17 (16.7) | > 0.999 |
| No vascular disease | 161 (80.9) | 84 (86.6) | 77 (75.5) | 0.050 |
| Prior stroke | 21 (10.6) | 12 (12.4) | 9 (8.8) | 0.492 |
| Prior transient ischemic attack | 3 (1.5) | 1 (1.0) | 2 (2.0) | > 0.999 |
| Prior thromboembolism | 7 (3.5) | 4 (4.1) | 3 (2.9) | 0.716 |
| CARTO mapping system, | 199 (100) | 97 (100) | 102 (100) | — |
| Diagnostic catheter, | ||||
| LASSO | 20 (10.1) | 8 (8.2) | 12 (11.8) | 0.483 |
| DECANAV | 22 (11.1) | 22 (22.7) | 0 (0) | < 0.001 |
| WEBSTER CS | 40 (20.1) | 20 (20.6) | 20 (19.6) | 0.862 |
| Soundstar | 178 (89.4) | 87 (89.7) | 91 (89.2) | > 0.999 |
| Pentaray | 178 (89.4) | 88 (90.7) | 90 (88.2) | 0.648 |
| Ablation catheter, | ||||
| SMARTTOUCH SF | 198 (99.5) | 96 (99.0) | 102 (100) | 0.487 |
| Unknown | 1 (0.5) | 1 (1.0) | 0 (0) | 0.487 |
| Sheath, | ||||
| VIZIGO | 97 (48.7) | 97 (100.0) | 0 (0) | < 0.001 |
| Agilis | 80 (40.2) | 0 (0) | 80 (78.4) | < 0.001 |
| Other | 21 (10.6) | 0 (0) | 21 (20.6) | < 0.001 |
| Unknown | 2 (1.0) | 0 (0) | 2 (2.0) | 0.498 |
| Substrate modification, | ||||
| Mitral isthmus | 4 (2.0) | 1 (1.0) | 3 (2.9) | 0.622 |
| Posterior wall | 30 (15.1) | 15 (15.5) | 15 (14.7) | > 0.999 |
| Other | 103 (51.8) | 47 (48.5) | 56 (54.9) | 0.396 |
| Parameters | All ( | VIZIGO ( | Non‐VIZIGO ( |
|
|---|---|---|---|---|
|
| ||||
| Fluid via catheter, mL | 772.6 ± 417.6 | 799.2 ± 337.8 | 748.1 ± 481.7 | 0.212 |
| Fluid via IV, mL | 1007.5 ± 320.8 | 961.3 ± 356.4 | 1051.1 ± 286.5 | 0.631 |
| Mapping time, min | 8.5 ± 4.2 | 8.0 ± 4.4 | 9.0 ± 4.0 | 0.179 |
| Time to left PVI, min | 19.0 ± 6.7 | 18.1 ± 7.5 | 19.9 ± 5.6 | 0.046 |
| Time to right PVI, min | 19.7 ± 8.7 | 16.5 ± 6.1 | 23.1 ± 9.9 | < 0.001 |
| Time to total PVI, min | 38.6 ± 11.3 | 34.6 ± 9.7 | 42.9 ± 11.4 | 0.002 |
| PV radiofrequency time, min | 23.5 ± 8.2 | 22.6 ± 8.3 | 24.3 ± 8.0 | 0.109 |
| Radiofrequency time, min | 34.9 ± 21.5 | 34.8 ± 26.3 | 35.0 ± 16.1 | 0.337 |
| Procedure time, min | 150.1 ± 57.3 | 149.4 ± 61.1 | 150.7 ± 53.9 | 0.637 |
| Fluoroscopy time, min | 12.8 ± 13.2 | 7.3 ± 10.4 | 18.3 ± 13.3 | < 0.001 |
| Fluoroscopy dose, mGy | 90.4 ± 196.6 | 45.9 ± 112.0 | 139.5 ± 251.5 | < 0.001 |
| Number of radiofrequency applications | 116.2 ± 70.3 | 129.2 ± 90.3 | 104.4 ± 41.7 | 0.041 |
| Left WACA | 46.1 ± 17.9 | 47.4 ± 18.8 | 44.9 ± 17.0 | 0.185 |
| Right WACA | 45.9 ± 15.5 | 45.2 ± 16.6 | 46.7 ± 14.5 | 0.398 |
| Maximum power, W | ||||
| Anterior | 43.5 ± 6.2 | 46.0 ± 3.7 | 41.2 ± 7.1 | < 0.001 |
| Posterior | 42.1 ± 6.4 | 44.8 ± 4.6 | 39.6 ± 6.8 | < 0.001 |
|
| ||||
| All PVs isolated by end of procedure | 199 (100) | 97 (100) | 102 (100) | ‐‐‐ |
| Parameters, | All ( | VIZIGO ( | Non‐VIZIGO ( |
|
|---|---|---|---|---|
|
| ||||
| Any PAE | 8 (4.0) | 3 (3.1) | 5 (4.9) | 0.722 |
| Cardiac tamponade/pericardial effusion | 2 (1.0) | 1 (1.0) | 1 (1.0) | > 0.999 |
| Major vascular access/bleeding | 6 (3.0) | 2 (2.1) | 4 (3.9) | 0.683 |
| Thromboembolism | 1 (0.5) | 1 (1.0) | 0 (0) | 0.490 |
| Atrioesophageal fistula | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Phrenic nerve paralysis/injury | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Severe pulmonary vein stenosis | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Device/procedure‐related death | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Stroke/cerebrovascular accident | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Myocardial infarction | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Transient ischemic attack | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Pericarditis | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Vagal nerve injury | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
| Unknown | 0 (0) | 0 (0) | 0 (0) | ‐‐‐ |
|
| ||||
| Repeat ablation | 0.408 | |||
| Yes | 17 (8.5) | 10 (10.3) | 7 (6.9) | |
| No | 175 (87.9) | 85 (87.6) | 90 (88.2) | |
| Unknown | 7 (3.5) | 2 (2.1) | 5 (4.9) | |
| Cardioversion | 0.519 | |||
| Yes | 6 (3.0) | 4 (4.1) | 2 (2.0) | |
| No | 180 (90.5) | 88 (90.7) | 92 (90.2) | |
| Unknown | 13 (6.5) | 5 (5.2) | 8 (7.8) | |
| AF/AT/AFL recurrence | 0.410 | |||
| Yes | 27 (13.6) | 13 (13.4) | 14 (13.7) | |
| No | 159 (79.9) | 80 (82.5) | 79 (77.5) | |
| Unknown | 13 (6.5) | 4 (4.1) | 9 (8.8) | |
| AAD status | ||||
| Not on AAD | 126 (63.3) | 60 (61.9) | 66 (64.7) | 0.769 |
| Placed on previous AAD at same dose | 29 (14.6) | 14 (14.4) | 15 (14.7) | > 0.999 |
| Placed on previous AAD at higher dose | 5 (2.5) | 1 (1.0) | 4 (3.9) | 0.369 |
| Placed on new AAD | 27 (13.6) | 16 (16.5) | 11 (10.8) | 0.301 |
| OAC use | 0.708 | |||
| Yes | 135 (67.8) | 63 (64.9) | 72 (70.6) | |
| No | 50 (25.1) | 27 (27.8) | 23 (22.5) | |
| Unknown | 14 (7.0) | 7 (7.2) | 7 (6.9) | |
- —This study was funded by Biosense Webster, Inc., part of Johnson & Johnson MedTech.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac Arrhythmias and Treatments · Cardiac pacing and defibrillation studies
Introduction
1
In atrial fibrillation (AF) catheter ablation procedures, steerable sheaths provide several advantages over non‐steerable sheaths, such as improved catheter access, stability, and tissue contact at ablation sites [1, 2, 3, 4]. The use of steerable sheaths has significantly improved single‐procedure AF ablation success rates in clinical trials and case–control analyses [1, 2, 5], with recent meta‐analyses of study data concluding that steerable sheaths are associated with better efficacy and a similar safety profile compared with non‐steerable sheaths [6, 7].
X‐ray fluoroscopy is widely used to guide catheter placement in ablation procedures, but radiation exposure can pose serious health risks to patients, operators, and laboratory staff. In addition, extended time wearing lead aprons by operators and staff may lead to the development of orthopedic problems [8, 9]. Visualizable steerable sheaths that incorporate three‐dimensional (3D) electroanatomical mapping systems can improve procedural efficiency by facilitating navigation and placement of the ablation catheter and can also reduce radiation exposure [10].
The CARTO VIZIGO Bidirectional Guiding Sheath (Biosense Webster Inc., Irvine, CA) is a steerable sheath that can be visualized using the compatible CARTO 3 EP Navigation System (Biosense Webster Inc.) without fluoroscopy [11]. Several studies have demonstrated significantly reduced fluoroscopy time with the VIZIGO sheath compared with non‐steerable and non‐visualizable steerable sheaths, along with comparable or improved procedural success, clinical effectiveness, and safety; however, these studies have been limited to single‐center settings [10, 12, 13, 14, 15, 16, 17].
The objective of the INSIGHT study was to further explore the real‐world impact of the VIZIGO steerable sheath on procedural efficiency, clinical effectiveness, and safety in paroxysmal AF catheter ablation in a cohort of patients treated particularly across multiple clinics in Japan.
Methods
2
Study Design
2.1
This non‐randomized, multicenter, retrospective cohort study included consecutive adults aged ≥ 18 years who underwent a de novo radiofrequency ablation for paroxysmal AF with a radiofrequency catheter at study sites in Japan (Nihon University School of Medicine, Nagano Chuo Hospital, Kobe City Medical Center General Hospital, Kameda Medical Center, and Saitama Red Cross Hospital). Patients were included if they had undergone radiofrequency ablation with a VIZIGO sheath between January 2020 and July 2021 or without a VIZIGO sheath between January 2019 and July 2021. Patients were required to have follow‐up data through 12 months after the index ablation procedure, with the exception of patients who died before their scheduled 12‐month follow‐up visit. Key exclusion criteria included a history of persistent AF or long‐standing persistent AF at the time of the ablation procedure, any prior left atrial ablation or cardiac‐related surgery before the ablation procedure, and enrollment in a potentially confounding drug or device trial at the time of the ablation procedure or within the 12‐month follow‐up period after the procedure.
The study was conducted according to the Declaration of Helsinki, Ethical Guidelines for Life Science and Medical Research Involving Human Subjects, and the Act on the Protection of Personal Information. All included patients provided informed consent according to the Ethical Guidelines for Life Science and Medical Research Involving Human Subjects.
Ablation Procedures
2.2
Catheter ablation procedures were typically conducted using a THERMOCOOL SMARTTOUCH SF Catheter (Biosense Webster Inc.) in conjunction with the CARTO mapping system. Ablation procedures were conducted with either the VIZIGO sheath with or without fluoroscopy or a non‐VIZIGO sheath with fluoroscopy. PENTARAY and/or LASSO (Biosense Webster Inc.) catheters were used for mapping and verification of pulmonary vein isolation (PVI). Pulmonary veins (PVs) were isolated using a point‐by‐point ablation technique, with isolation of the PVs documented. Ablations beyond PVI, such as cavotricuspid or mitral isthmus ablations or ablations targeting non‐PV foci, were performed when these arrhythmias were either induced by burst atrial pacing or observed clinically.
Study Outcomes
2.3
Primary procedural efficiency outcomes for the cohort comparative analysis included fluoroscopy time and dose. Fluoroscopy details were compared further in sequential case order for the study centers. Other procedural efficiency outcomes included volume of fluid delivered, mapping time, time to PVI, total procedure time, radiofrequency time (PV and total), number of radiofrequency applications, maximum power, and catheter stability. The number of radiofrequency applications and PV radiofrequency time were also assessed by study center level. Case data from CARTO was extracted from the CARTONET cloud‐based storage and artificial intelligence analytics platform to evaluate catheter stability. The stability values used for analysis denote the mean catheter displacement during the first 90% of the ablation time for each lesion. This allowed for removal of the purposeful motion to reposition the catheter for the next lesion site.
Acute PVI outcomes included first pass PVI, return of conduction, and PVI by the end of the procedure. Longer‐term clinical effectiveness outcomes through 12 months of follow‐up included reablation; cardioversion; AF, atrial tachycardia (AT), and atrial flutter (AFL) recurrence after a 90‐day blanking period through 12 months; single‐procedure freedom from AF/AT/AFL recurrence after a 90‐day blanking through 12 months; antiarrhythmic drug status; and oral anticoagulant use. Safety outcomes included device‐ and procedure‐related primary adverse events (PAEs) within 7 days of index procedure, which included phrenic nerve paralysis/injury, stroke/cerebrovascular accident, transient ischemic attack, thromboembolism, myocardial infarction, pericarditis, vagal nerve injury, and major access complication/bleeding. Device‐ or procedure‐related death, atrioesophageal fistula, and severe pulmonary vein stenosis up to 90 days and cardiac tamponade/pericardial effusion up to 30 days post‐index procedure were also considered PAEs.
Statistical Analysis
2.4
Continuous data were summarized as mean ± standard deviation and tested based on Wilcoxon rank sum test for VIZIGO compared with non‐VIZIGO procedures. Categorical data were summarized as frequencies and percentages and tested based on Fisher's exact test for VIZIGO compared with non‐VIZIGO procedures. Empirical prediction plots and linear mixed‐effects models were used to estimate average fluoroscopy time and dose by study site for each ablation case sequence. Kaplan–Meier survival analysis was performed to obtain estimates and 95% confidence intervals (CI) for freedom from AF/AT/AFL recurrence after a 90‐day blanking period and reablation at any time. Statistical analyses were performed using SAS, version 3.8 (SAS Institute Inc., Cary, NC, USA).
Results
3
Baseline Patient Characteristics and Index Ablation Procedure Details
3.1
A total of 199 patients met the inclusion and exclusion criteria, with 97 patients undergoing ablation with a VIZIGO sheath and 102 with a non‐VIZIGO sheath. Of the 25 operators who performed these ablations, 15 performed procedures using both the VIZIGO and non‐VIZIGO sheaths, 3 performed procedures using only the VIZIGO sheath, and 7 performed procedures using only non‐VIZIGO sheaths. Overall, the mean age was 69.7 years and 59.3% (118/199) of the participants were male (Table 1). Baseline patient characteristics were similar between the VIZIGO and non‐VIZIGO groups.
In the non‐VIZIGO group, the Agilis NxT steerable sheath (Abbott Inc, St. Paul, MN) was used in 78.4% (80/102) of patients. The majority (68.8% [137/199]) of patients underwent ablation with substrate modification, including posterior wall in 15.1% (30/199), with no significant differences between VIZIGO and non‐VIZIGO groups (Table 1).
Procedural Efficiency Outcomes
3.2
Procedural efficiency outcomes are summarized in Table 2. Significantly shorter mean times were achieved in the VIZIGO group vs. the non‐VIZIGO group for time to left PVI (18.1 ± 7.5 vs. 19.9 ± 5.6 min, p = 0.046), right PVI (16.5 ± 6.1 vs. 23.1 ± 9.9 min, p < 0.001), and total PVI (34.6 ± 9.7 vs. 42.9 ± 11.4 min, p = 0.002). The non‐VIZIGO group was associated with an average of 9.5 min longer time to PVI, adjusting for the number of radiofrequency applications (p < 0.001). The mean fluoroscopy time was significantly shorter (7.3 ± 10.4 vs. 18.3 ± 13.3 min, p < 0.001), and the mean fluoroscopy dose was significantly lower (45.9 ± 112.0 vs. 139.5 ± 251.5 mGy, *p *< 0.001) with the VIZIGO sheath compared with non‐VIZIGO sheaths (Table 2). When comparing the cases sequentially among study centers, average fluoroscopy time (slope: –0.38 [95% CI: –0.82, 0.07] vs. slope: –0.25 [95% CI: –0.73, 0.24]) and dose (slope: –5.76 [95% CI: –14.24, 2.72] vs. slope: –4.61 [95% CI: –19.14, 9.93]) decreased quicker and were consistently lower using the VIZIGO sheath as more cases were done (Figure 1). The mean PV radiofrequency time was comparable in the VIZIGO group (22.6 ± 8.3 min) and the non‐VIZIGO group (24.3 ± 8.0 min). While the mean number of radiofrequency applications was significantly higher overall in the VIZIGO group compared with the non‐VIZIGO group (129.2 ± 90.3 vs. 104.4 ± 41.7, p = 0.041), there were no significant differences between groups when comparing left‐ and right‐sided wide area circumferential ablation. Radiofrequency mean maximum power was significantly higher in the VIZIGO group vs. the non‐VIZIGO group for anterior (46.0 ± 3.7 vs. 41.2 ± 7.1 W, p < 0.001) and posterior (44.8 ± 4.6 vs. 39.6 ± 6.8 W, p < 0.001) applications. There were no significant differences between the VIZIGO and non‐VIZIGO groups in total catheter stability or for left‐ and right‐sided wide area circumferential ablation (Figure 2). All other procedural efficiency and PVI measures were similar in the VIZIGO and non‐VIZIGO groups.
Fluoroscopy time (A) and fluoroscopy dose (B) for patients in the VIZIGO and non‐VIZIGO groups by case sequence. Data are mean ± SD averaged for each site. SD, standard deviation.
Catheter location stability for patients in the VIZIGO and non‐VIZIGO groups. Data are mean ± SD. SD, standard deviation; WACA, wide area circumferential ablation.
The mean number of radiofrequency applications and PV radiofrequency time varied by study site (Figure 3). At two study sites, the number of radiofrequency applications was significantly higher in the VIZIGO than in the non‐VIZIGO group (*p *≤ 0.022; Figure 3A). At the remaining three study sites, there was no significant difference in the number of radiofrequency applications between the VIZIGO and non‐VIZIGO groups. PV radiofrequency time was significantly longer in the VIZIGO than in the non‐VIZIGO group at one study site (p = 0.034), was significantly shorter in the VIZIGO than in the non‐VIZIGO group at another site (p < 0.001), and did not differ significantly between the VIZIGO and non‐VIZIGO groups at the remaining three sites (Figure 3B).
Number of radiofrequency applications (A) and PV radiofrequency time (B) by study site. Data are mean ± SD. PV, pulmonary vein; SD, standard deviation.
For the 15 operators who performed procedures using both the VIZIGO and non‐VIZIGO sheaths, mean fluoroscopy time (13.6 ± 13.9 min), radiofrequency time (31.5 ± 12.3 min), and time to total PVI (34.6 ± 8.6) were similar to those observed for the overall group of operators (12.8 ± 13.2, 34.9 ± 21.5, and 38.6 ± 11.3 min, respectively).
Safety
3.3
Device/procedure‐related PAE rates were similar in the VIZIGO and non‐VIZIGO groups (3.1% [3/97] vs. 4.9% [5/102], p = 0.722; Table 3). In the VIZIGO group, PAEs were reported in 3 patients and comprised cardiac tamponade/pericardial effusion (1 patient), major vascular access/bleeding (2 patients), and thromboembolism (1 patient, who also experienced major vascular access/bleeding), while in the non‐VIZIGO group, PAEs were reported in 5 patients and comprised cardiac tamponade/pericardial effusion (1 patient) and major vascular access/bleeding (4 patients). There were no reports of atrioesophageal fistula, phrenic nerve paralysis/injury, severe pulmonary vein stenosis, stroke, transient ischemic attack, myocardial infarction, pericarditis, or vagal nerve injury. No procedure‐related deaths occurred.
Clinical Effectiveness
3.4
Effectiveness outcomes are summarized in Table 3. After 12 months of follow‐up, clinical effectiveness outcomes, including repeat ablation, cardioversion, and AF/AT/AFL recurrence, were similar in the VIZIGO and non‐VIZIGO groups. Kaplan–Meier estimates of single‐procedure freedom from AF/AT/AFL recurrence at 12 months were 86.6% (95% CI: 78.0%, 92.0%) in the VIZIGO group and 89.2% (95% CI: 81.4%, 93.9%) in the non‐VIZIGO group (p = 0.5072, Figure 4). The 12‐month success rate (85.1%) was similar for the group of operators (n = 15) who used both VIZIGO and non‐VIZIGO sheaths. Most patients in the VIZIGO and non‐VIZIGO groups were not on an antiarrhythmic medication at 12 months (61.9% [60/97] and 64.7% [66/102], respectively), while most were on oral anticoagulant therapy at 12 months (64.9% [63/97] and 70.6% [72/102], respectively).
Kaplan–Meier single procedure survival from AF/AT/AFL recurrence. Single‐procedure survival was defined as freedom from recurrence after a 90‐day blanking period and reablation at any time. AF, atrial fibrillation; AFL, atrial flutter; AT, atrial tachycardia.
Discussion
4
In the current study, use of the VIZIGO sheath in paroxysmal AF ablation procedures significantly shortened fluoroscopy time and significantly lowered fluoroscopy dose compared with use of a non‐VIZIGO sheath. We observed no differences in procedural safety or effectiveness, with a low incidence of device/procedure‐related PAEs in both the VIZIGO and non‐VIZIGO groups (3.1% and 4.9%, respectively) and a > 85% single‐procedure freedom from AF/AT/ATL recurrence through 12 months in both the groups.
The VIZIGO design allows for sheath visualization on the CARTO map during a procedure without depending solely on fluoroscopy. Accordingly, the results of the current study are consistent with previous studies that have reported a significantly lower fluoroscopy dose and/or time with the VIZIGO sheath vs. fixed or other steerable sheaths [10, 12, 13, 14, 15, 16, 17]. While the rate of procedures that did not employ fluoroscopy was not recorded in the current cohort, previous studies have confirmed that VIZIGO can be incorporated into zero fluoroscopy workflows. Bertini et al. first described zero fluoroscopy workflow in two cases of AF ablation using the VIZIGO sheath under 3D electroanatomic mapping and intracardiac echocardiography guidance [18]. Subsequently, in a US single‐center study, 99% of 142 procedures that used the VIZIGO sheath were performed without fluoroscopy [13], while at a Hungarian clinic, 88% of 50 VIZIGO procedures used no fluoroscopy after the transseptal puncture [14]. In contrast, non‐visualized steerable sheaths, such as the Agilis sheath used in nearly 80% of procedures in the non‐VIZIGO group in the current study, cannot be incorporated into zero fluoroscopy workflows. Overall, results from this and previous studies support use of the VIZIGO sheath in minimal fluoroscopy workflows and in the transition to zero fluoroscopy procedures if desired [13].
Another advantageous feature of the VIZIGO sheath is that it is bidirectional, with deflections of 180° in both directions, which allows for greater access to sites beyond the PV [11].
In the current study, PVI was achieved by the end of the procedure in all the patients regardless of sheath type, although time to PVI was significantly shorter in the VIZIGO group, at 35 min, vs. 43 min in the non‐VIZIGO group. The overall procedure time was not reduced with the VIZIGO sheath in this study, possibly due to the time needed to generate a 3D matrix of the right atrium for visualization of the sheath before proceeding to the left atrium. It is also possible that operators may have had a learning curve as they adjusted to the new VIZIGO technology.
An analysis of the number of radiofrequency applications and PV radiofrequency time by study site demonstrated some differences across the hospitals included in this study. The number of radiofrequency applications varied substantially but was higher with the VIZIGO sheath than with non‐VIZIGO sheaths at four of the five participating hospitals, although this difference did not reach statistical significance at two of those hospitals. This finding suggests that ablation of additional targets was pursued more frequently with the VIZIGO than with non‐VIZIGO sheaths. The differences in the number of radiofrequency applications and PV radiofrequency time may reflect differences in operator experience or hospital protocols; nevertheless, the trends observed with the VIZIGO compared with the non‐VIZIGO sheath were generally consistent across study sites in this multicenter study.
Our findings showed that using the VIZIGO sheath with reduced fluoroscopy and alternative imaging enabled operators to achieve similar catheter stability as with non‐VIZIGO sheaths with fluoroscopy. Other studies have reported greater catheter stability with the VIZIGO sheath vs. non‐steerable sheaths [13, 15]. While the small studies conducted so far have not shown a difference in long‐term clinical outcomes with VIZIGO vs. other sheaths, catheter and contact‐force stability is known to be a predictor of 12‐month postablation success [19].
The limitations of this study include the non‐randomized retrospective study design, lack of adjustment for confounding factors, and limited generalizability to patients outside of Japan. This study was not aimed to compare the costs between using VIZIGO vs. non‐VIZIGO sheaths. As these costs can vary by region, future evaluations may be beneficial to understand cost impact.
Conclusions
5
These real‐world data demonstrate that when treating paroxysmal AF by radiofrequency ablation, use of the VIZIGO sheath can significantly shorten fluoroscopy time and reduce fluoroscopy dose, thereby alleviating the burden of heavy protective equipment, while improving procedural efficiency without compromising safety or acute and longer‐term clinical effectiveness of AF ablation.
Ethics Statement
The study was conducted according to the Declaration of Helsinki, Ethical Guidelines for Life Science and Medical Research Involving Human Subjects, and the Act on the Protection of Personal Information.
Consent
All included patients provided informed consent according to the Ethical Guidelines for Life Science and Medical Research Involving Human Subjects.
Conflicts of Interest
Yasuo Okumura received research grants unrelated to this study from Johnson & Johnson K.K. and Biosense Webster Inc.; scholarship funds from Nippon Boehringer Ingelheim, remuneration from Daiichi‐Sankyo, AstraZeneca, Bayer Healthcare, Bristol Myers Squibb, and Johnson & Johnson K.K.; and belongs to the endowed departments of Boston Scientific Japan, Biotronik Japan, Abbott Medical Japan, Japan Lifeline, and Medtronic Japan. Akira Mizukami received speaking fees from Johnson & Johnson K.K., Medtronic Japan Co. Ltd., and Abbott Japan LLC. Osamu Inaba received speaking fees and research funding from Johnson & Johnson K.K., Boston Scientific Japan K.K., and Medtronic Japan Co. Ltd. Daisuke Yamagishi received speaking fees from Johnson & Johnson K.K., Toray Industries Inc., Toray Medical Inc., Japan Lifeline Inc., Synaptic Medical Japan Inc., and Nihon Kohden Inc.; grants from Biosense Webster Inc., part of Johnson & Johnson MedTech. Yi Wang is a contractor providing biostatistical support for Biosense Webster Inc., part of Johnson & Johnson MedTech. Atsushi Kobori receives speaking fees from Johnson & Johnson K.K., Boston Scientific Japan, Abbott Medical Japan, Japan Lifeline, and Medtronic Japan. The other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. Piorkowski , C. Eitel , S. Rolf , et al., “Steerable Versus Nonsteerable Sheath Technology in Atrial Fibrillation Ablation: A Prospective, Randomized Study,” Circulation: Arrhythmia and Electrophysiology 4 (2011): 157–165.21248246 10.1161/CIRCEP.110.957761 · doi ↗ · pubmed ↗
- 2C. Piorkowski , H. Kottkamp , J. H. Gerds‐li , et al., “Steerable Sheath Catheter Navigation for Ablation of Atrial Fibrillation: A Case–Control Study,” Pacing and Clinical Electrophysiology 31 (2008): 863–873.18684284 10.1111/j.1540-8159.2008.01101.x · doi ↗ · pubmed ↗
- 3W. Ullah , R. J. Hunter , A. Mc Lean , et al., “Impact of Steerable Sheaths on Contact Forces and Reconnection Sites in Ablation for Persistent Atrial Fibrillation,” Journal of Cardiovascular Electrophysiology 26 (2015): 266–273.25346514 10.1111/jce.12573 · doi ↗ · pubmed ↗
- 4M. W. Deyell , G. Wen , Z. Laksman , et al., “The Impact of Steerable Sheaths on Unblinded Contact Force During Catheter Ablation for Atrial Fibrillation,” Journal of Interventional Cardiac Electrophysiology 57 (2020): 417–424.30701358 10.1007/s 10840-019-00514-1 · doi ↗ · pubmed ↗
- 5S. Matsuo , T. Yamane , T. Date , et al., “Completion of Mitral Isthmus Ablation Using a Steerable Sheath: Prospective Randomized Comparison With a Nonsteerable Sheath,” Journal of Cardiovascular Electrophysiology 22 (2011): 1331–1338.21649779 10.1111/j.1540-8167.2011.02112.x · doi ↗ · pubmed ↗
- 6M. Mhanna , A. Beran , A. Al‐Abdouh , et al., “Steerable Versus Nonsteerable Sheath Technology in Atrial Fibrillation Ablation: A Systematic Review and Meta‐Analysis,” Journal of Arrhythmia 38 (2022): 570–579.35936032 10.1002/joa 3.12742 PMC 9347204 · doi ↗ · pubmed ↗
- 7X. Jin , Y. Zhou , Y. Wu , and M. Xie , “Safety and Efficacy of Steerable Versus Non‐Steerable Sheaths for Catheter Ablation of Atrial Fibrillation Systematic Review and Meta‐Analysis,” BMJ Open 13 (2023): e 068350.10.1136/bmjopen-2022-068350 PMC 1051459837734901 · doi ↗ · pubmed ↗
- 8U. Canpolat , M. Faggioni , D. G. Della Rocca , et al., “State of Fluoroless Procedures in Cardiac Electrophysiology Practice,” Journal of Innovations in Cardiac Rhythm Management 11 (2020): 4018–4029.32368376 10.19102/icrm.2020.110305 PMC 7192123 · doi ↗ · pubmed ↗