Emphysematous Cystitis in an Immunocompetent Patient on an SGLT2 Inhibitor
Kailey N Nguyen, Dipesh R Bista

TL;DR
This paper reports a rare case of bladder infection with gas caused by a diabetes medication in a man with diabetes.
Contribution
It highlights a possible link between SGLT2 inhibitors and severe urinary infections.
Findings
A diabetic male developed emphysematous cystitis caused by Klebsiella pneumoniae.
The patient was on empagliflozin, an SGLT2 inhibitor, suggesting a potential risk.
This case emphasizes the need for awareness of such infections in patients on SGLT2 inhibitors.
Abstract
Emphysematous cystitis is a rare, severe infection of the urinary bladder caused by gas-forming organisms like Escherichia coli and Klebsiella pneumoniae (K. pneumoniae). Common risk factors are female sex, chronic urinary infection, immunosuppression, diabetes mellitus, and neurogenic bladder. We report a case of K. pneumoniae emphysematous cystitis in a diabetic male patient being treated with empagliflozin. With this case report, we aim to highlight the potential role of an SGLT-2 inhibitor such as empagliflozin in developing severe urinary infections such as emphysematous cystitis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
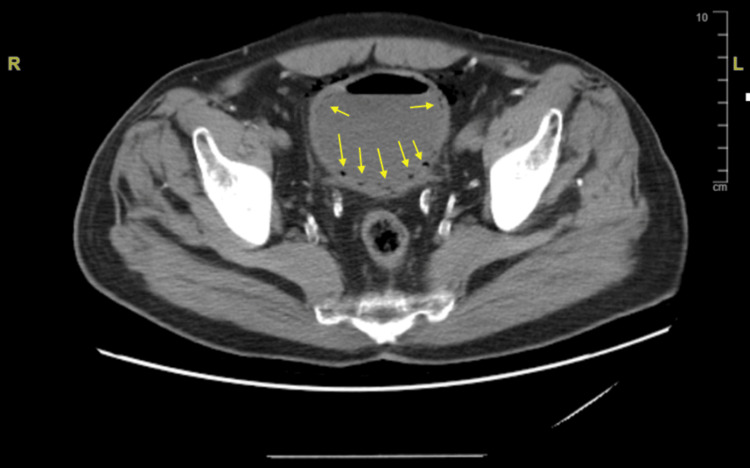 Figure 1
Figure 1| Vitals | Patient | Normal Range |
| Blood pressure | 176/76 | <120/80 mmHg |
| Pulse rate | 74 | 60-100 beats per minute |
| Respiratory rate | 16 | 12-20 breaths per minute |
| Arterial oxygen saturation | 97% on room air | 95-100% |
| Markers | Patient | Normal Range |
| Turbidity | S1 Cloudy | Clear |
| pH | 6.0 | 5.0-8.0 |
| Protein | 2+ | Negative |
| Glucose | 3+ | Negative |
| Blood | 3+ | Negative |
| Leukocyte esterase | 2+ | Negative |
| Nitrites | Negative | Negative |
| Bilirubin | Negative | Negative |
| Urobilinogen | Negative | Negative |
| Ketones | Trace | Negative |
| Urine microscopy | ||
| White blood cells | 100+ | 0-5 per high power field |
| Red blood cells | 100+ | 0-3 per high power field |
| Bacteria | Light | Absent |
| Epithelial cells | Rare | Few per high power field |
| Blood Test Results | Patient | Normal Range |
| Comprehensive metabolic panel | ||
| Glucose | 208 | 70–99 mg/dL |
| Blood urea nitrogen | 30 | 7–18 mg/dL |
| Creatinine | 1.79 | 0.70–1.30 mg/dL |
| Sodium | 138 | 136–145 meq/L |
| Potassium | 4.0 | 3.6–5.0 meq/L |
| Chloride | 106 | 98–107 meq/L |
| Carbon dioxide | 27 | 21–32 meq/L |
| Calcium | 8.9 | 8.5–10.1 mg/dL |
| Total bilirubin | 0.3 | 0.0–11.1 mg/dL |
| Alkaline phosphatase | 120 | 40–129 U/L |
| Aspartate aminotransferase | 24 | 0–40 U/L |
| Alanine aminotransferase | 30 | 0–41 U/L |
| Total protein | 6.3 | 6.1–7.9 g/dL |
| Albumin | 3.0 | 3.9–5.2 g/dL |
| Complete blood count | ||
| White blood cell | 10.1 | 3.7–10.3 k/µL |
| Red blood cell | 4.66 | 4.50–6.00 M/µL |
| Hemoglobin | 13.6 | 13.5–18.0 g/dL |
| Hematocrit | 41.0 | 40.0–52.0% |
| Mean corpuscular volume | 88.0 | 80.0–99.0 fL |
| Mean corpuscular hemoglobin concentration | 33.2 | 27.0–33.0 pg |
| Platelet | 198 | 140–440 k/µL |
| Mean platelet volume | 10.3 | 8.5–12.0 fL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Disease Case Reports and Treatments · Diverticular Disease and Complications · Biliary and Gastrointestinal Fistulas
Introduction
Emphysematous cystitis (EC) is a rare infection of the urinary bladder associated with the presence of air within the bladder wall. The most common bacteria leading to emphysematous cystitis are Escherichia coli (E. coli) and* Klebsiella pneumoniae* (K. pneumoniae) [1]. Emphysematous cystitis is classically described in elderly females with a history of diabetes mellitus. Other risk factors have been described as chronic urinary tract infection, neurogenic bladder, long-term indwelling urinary catheter, and immunosuppression [2]. Sodium-glucose cotransporter 2 (SGLT2) inhibitor, such as empagliflozin, is a class of anti-diabetic medication that inhibits the sodium-glucose transporter from reabsorbing glucose from the lumen of the proximal convoluted tubules, leading to increased glucose excretion in the urine and lowered serum glucose. Here we present a case of EC in a diabetic 76-year-old male without prior history of urinary tract infection who had been treated with empagliflozin for diabetes mellitus. Our literature review showed that this is only the second case report suggesting a link between EC and an SGLT2 inhibitor such as empagliflozin.
Case presentation
The patient is a 76-year-old male with past medical history significant for type 2 diabetes mellitus, hypertension, coronary artery disease, peripheral artery disease, bilateral below-knee amputation, and chronic obstructive pulmonary disease not currently on steroids who presented for evaluation of two weeks of dysuria and three days of hematuria described as “blood spotting in the urine.” The patient also endorsed lower back pain and suprapubic abdominal pain that started nine days prior and had since dissipated. He also reported gas coming out of his urethra after urination.
Home medications included empagliflozin, insulin detemir, insulin lispro, atorvastatin, ferrous sulfate, losartan-hydrochlorothiazide, vitamin B12, and vitamin D3.
Vital signs were all within normal limits except for elevated blood pressure (Table 1). Physical exam was only notable for suprapubic tenderness and absent costovertebral angle tenderness.
Urine analysis was significant for elevated glucose levels and findings consistent with urinary tract infection (Table 2).
Blood tests were also performed. A comprehensive metabolic panel was significant for elevated glucose levels; serum creatinine and blood urea nitrogen levels were also elevated, but they appeared to be the patient's baseline. Comprehensive blood count with differential was within normal limits (Table 3). Hemoglobin A1c level was found to be 9.7.
Computed tomography (CT) scan of the abdomen and pelvis without contrast showed severe emphysematous cystitis, with bladder gas dissecting into peri-cystic fat, and an under-distended bladder. There was no hydronephrosis, and the prostate was noted to be mildly enlarged.
Computed tomography of the abdomen and pelvis The presence of air (yellow arrows) within the urinary bladder wall demonstrates findings consistent with emphysematous cystitis.
The patient was diagnosed with emphysematous cystitis and treated empirically with piperacillin-tazobactam, then transitioned to ceftriaxone given the lack of overt multidrug resistance risk factors. Urine culture eventually grew Klebsiella pneumoniae. On discharge, the patient was switched to oral ciprofloxacin according to sensitivity results to complete a three-week course of antibiotics. Empagliflozin was held on admission and later discontinued upon discharge due to concerns that it was exacerbating the infection via glycosuria.
Discussion
Emphysematous cystitis is a rare complication of urinary tract infection. It is caused by organisms such as Enterobacter aerogenes, Proteus mirabilis, Staphylococcus aureus, Streptococci, Clostridium perfringens, Candida albicans, but most commonly E. coli and K. pneumoniae [1]. It is suggested that glucose fermentation by these bacteria forms gas within the bladder, leading to the characteristic finding of gas penetration into the bladder wall. Risk factors include old age and female sex, diabetes mellitus, immunosuppressant, neurogenic bladder, recurrent urinary tract infections [1,3]. Interestingly, classic urinary tract infection (UTI) symptoms, such as dysuria, increased frequency, and urgency, are not always present. A case series consisting of 53 cases reported that only about 53.3% of cases had classical UTI symptoms. More common presenting symptoms were abdominal pain, noted in 65.6% of cases, and hematuria, which was noted in 82.3% of cases [4]. Emphysematous cystitis presents on a wide spectrum ranging from asymptomatic to severe life-threatening illness, with the most severe cases associated with emphysematous pyelonephritis and urosepsis [5]. Mortality associated with EC has been reported to be between 1.78% to 7%, but increased to 14% when associated with another emphysematous infection of the urinary tract, such as emphysematous pyelonephritis [5,6]. The diagnostic method of choice is a CT scan, checking for the presence of gas within the bladder wall. Treatment ranges from antibiotics, which could be oral for mild, uncomplicated cases, to intravenous antibiotics, which are necessary in most cases. Up to 10% of cases have been reported to need surgical intervention like partial cystectomy, total cystectomy, or surgical debridement [5].
Sodium-glucose cotransporter 2 (SGLT2) inhibitors such as empagliflozin are being increasingly used in patients with type 2 diabetes mellitus due to their cardiovascular and reno-protective effects [7]. They inhibit sodium-glucose co-transporter-2, which under normal conditions reabsorbs filtered glucose in the proximal convoluted tubules. Thus, SGLT2 inhibitors allow more glucose to be excreted in the urine, leading to higher-than-normal levels of glucose in the urine. Huang et al. proposed that, along with the presence of gas-forming bacteria and impaired tissue perfusion, glycosuria is one of the three conditions thought to be critical in developing EC [3].
In their review analysis of thirteen trials of different SGLT2 inhibitors, Kittipubul et al. concluded that although SGLT2 inhibitors such as empagliflozin cause glycosuria, they do not increase the risk of urinary tract infections [8]. However, it is worth noting that in 2015, the Food and Drug Administration (FDA) issued a warning about the increased risk of severe UTI associated with SGLT2 inhibitors due to nineteen cases of life-threatening urosepsis and pyelonephritis reported within eighteen months since the approval of canagliflozin, the first SGLT2 inhibitor [9]. In 2018, the FDA issued another warning about the increased risk of necrotizing perineal infection requiring surgical debridement in patients taking SGLT2 inhibitors. This risk is estimated to be 200% higher with SGLT2 inhibitors than with other anti-diabetic drug classes [10]. Thus, we reckon the plausibility of increased risk of severe infection like EC in patients taking SGLT 2 inhibitors. Additionally, although the consensus is that SGLT2 inhibitors should be discontinued immediately upon the occurrence of severe infection [11,12], there is no established guidance on when and if SGLT2 inhibitors should be restarted in these patients after the infection has been treated. In our literature review, we also found one other case report of EC potentially being linked to SGLT2 inhibitor use [13].
Conclusions
Emphysematous cystitis is a rare and potentially fatal infection of the urinary bladder, classically presenting in elderly diabetic females. We presented a case of emphysematous cystitis in a male patient with diabetes mellitus taking an SGLT2 inhibitor. Our patient only presented with mild symptoms such as dysuria and hematuria. He did not experience more severe complications, such as bladder perforation, and was managed non-surgically with intravenous antibiotics followed by a prolonged course of oral antibiotics for three weeks. In our literature review, a meta-analysis suggested that being on an SGLT2 inhibitor does not increase the risk of UTI, but on the other hand, there have been FDA warnings on increased risk of severe urinary tract infection as well as necrotizing perineal infection. Therefore, it is plausible to assume that taking an SGLT2 inhibitor increased the risk of more severe infection, like emphysematous cystitis, in this patient with uncontrolled diabetes mellitus. Given expanding indications for SGLT2 inhibitor use in patients with and without diabetes mellitus, we reckon more research is needed to investigate the role of SGLT2 inhibitors in the development of severe urinary tract infections to help further guide our management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Emphysematous cystitis in the absence of known risk factors: an unusual clinical entity South Med J Kelesidis T Osman S Tsiodras S 94294610220091966805110.1097/SMJ.0b 013e 3181 adf 18c PMC 8056330 · doi ↗ · pubmed ↗
- 2Emphysematous cystitis: an incidental finding with varying outcomes Ann R Coll Surg Engl Tan TJ Parmar K Mukherjee A Sonawane P Badrakumar C 879010520233563891710.1308/rcsann.2022.0020 PMC 9773271 · doi ↗ · pubmed ↗
- 3Mixed acid fermentation of glucose as a mechanism of emphysematous urinary tract infection J Urol Huang JJ Chen KW Ruaan MK 1481511461991205657610.1016/s 0022-5347(17)37736-4 · doi ↗ · pubmed ↗
- 4Emphysematous cystitis: illustrative case report and review of the literature Medicine (Baltimore) Grupper M Kravtsov A Potasman I 47538620071722075510.1097/MD.0b 013e 3180307 c 3a · doi ↗ · pubmed ↗
- 5Emphysematous cystitis: a review of 135 cases BJU Int Thomas AA Lane BR Thomas AZ Remer EM Campbell SC Shoskes DA 172010020071750687010.1111/j.1464-410X.2007.06930.x · doi ↗ · pubmed ↗
- 6Emphysematous cystitis: a case report and literature review of 113 cases Urol Ann Ranjan SK Navriya SC Kumar S Mittal A Bhirud DP 3123151320213442127210.4103/UA.UA_61_20PMC 8343293 · doi ↗ · pubmed ↗
- 7Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2025 Diabetes Care American Diabetes Association Professional Practice Committee 0206482025
- 8Genitourinary tract infections in patients taking SGLT 2 inhibitors: JACC review topic of the week J Am Coll Cardiol Kittipibul V Cox ZL Chesdachai S Fiuzat M Lindenfeld J Mentz RJ 156815788320243863177610.1016/j.jacc.2024.01.040 · doi ↗ · pubmed ↗