Redo bilateral lung transplantation in a previous heart-lung transplant recipient for invasive pulmonary scedosporiosis
Akshay Chauhan, Nischal Ranganath, John P. Scott, Paschalis Vergidis, Anja C. Roden, Philip J. Spencer, Mauricio A. Villavicencio, Richard C. Daly, Sahar A. Saddoughi

TL;DR
A rare case of redo-bilateral lung transplant in a heart-lung transplant recipient was successfully managed with surgery and antifungal treatment.
Contribution
This case report presents a successful surgical and medical management approach for a rare complication in heart-lung transplant recipients.
Findings
The patient showed no issues with bronchial anastomosis healing after the redo-bilateral lung transplant.
A combination of inhaled antifungal drugs led to a positive 1-year outcome for the patient.
The case demonstrates a viable strategy for managing invasive pulmonary scedosporiosis in transplant recipients.
Abstract
Redo-bilateral lung transplant in previous heart-lung transplant is a rare operation. We describe our surgical and medical management experience with a heart-lung transplant recipient who developed chronic lung allograft dysfunction and invasive Scedosporium apiospermum infection. The patient underwent a redo-bilateral lung transplant followed by a combination of inhaled voriconazole, caspofungin, and olorofim for a prolonged period. We observed no issues with bronchial anastomosis healing, and the patient is doing well on 1-year follow-up. This report outlines a successful management approach to this rare complication of heart-lung transplant recipients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
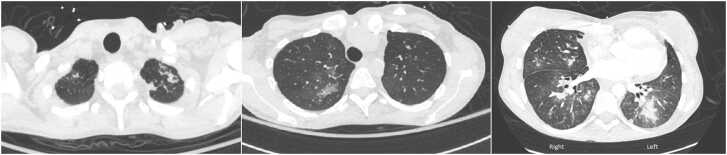 Figure 1
Figure 1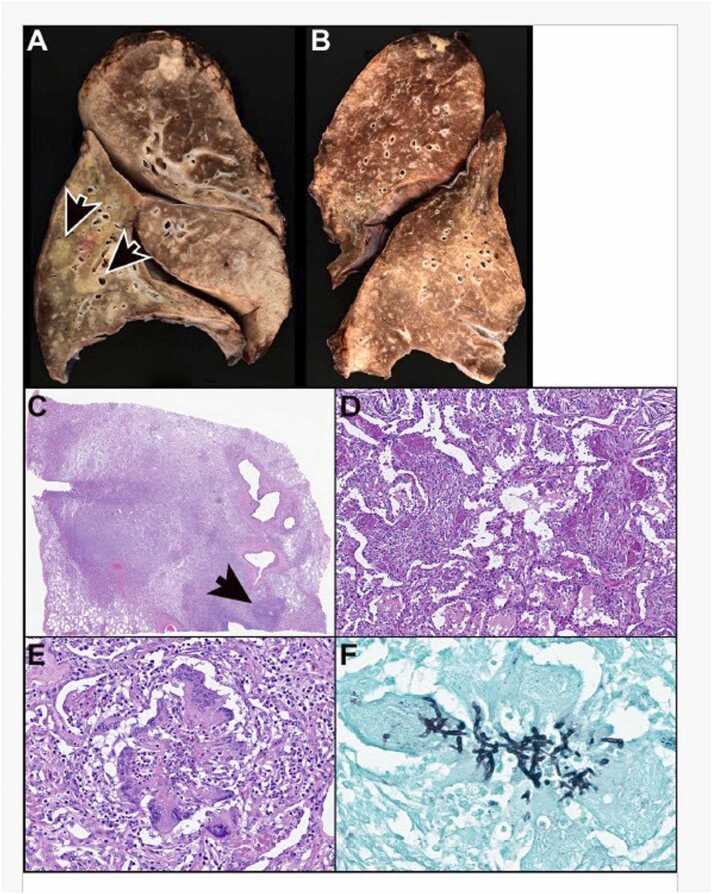 Figure 2
Figure 2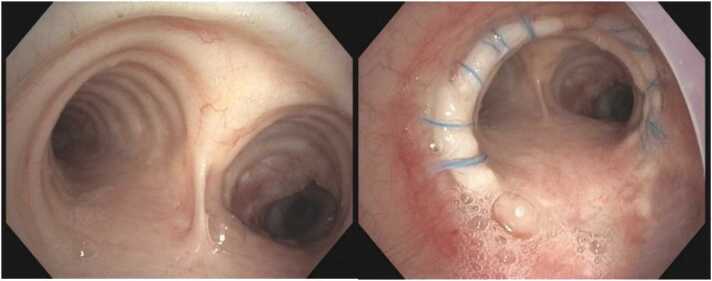 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Parasitic Infections and Diagnostics · Pneumocystis jirovecii pneumonia detection and treatment
Background
Redo-lung transplants in patients with prior heart-lung transplants are rare but are expected to become more frequent due to rising numbers of combined procedures. We report a case of a heart-lung transplant recipient with chronic lung allograft dysfunction (CLAD) and severe, treatment-resistant pulmonary scedosporiosis necessitating redo-bilateral lung transplant. This represents the first documented case of refractory Scedosporium apiospermum infection in such recipients treated with this approach,1 underscoring both technical challenges and pharmacological advancements in post-transplant infection management.
Case report
The patient is a 35-year-old woman who underwent combined heart-lung transplant 7 years ago presented with stage 3 CLAD and progressive respiratory failure. Her sputum culture had growth of Scedosporium apiospermum, for which she received posaconazole and caspofungin. She had failed prior therapy with voriconazole, and olorofim was not available before transplant. Despite antimicrobial susceptibility–directed therapy, the patient continued to have progression of chronic respiratory failure with persistent isolation of Scedosporium spp. in lower respiratory cultures. Serum galactomannan was negative and 1-3-B-D-glucan was positive (91 pg/ml). Computed tomography of the chest showed features of CLAD and right lower lobe consolidation (Figure 1). Her cardiac allograft function was preserved. Given the concern for poorly controlled invasive fungal infection and CLAD-BOS (bronchiolitis obliterans syndrome) type, the decision was made to proceed with redo-lung transplant. Certainly, the decision to proceed with transplant was not taken lightly, given the surgical complexity of the case in combination with the difficult infection that we knew had seeded the airway.Figure 1. Preoperative computed tomography scan of the chest with contrast demonstrating consolidative nodular opacity in the left lower lung with scattered opacities throughout the remaining lungs, with bronchial and lung parenchyma changes suggestive of CLAD. CLAD, chronic lung allograft dysfunction.Figure 1
The patient underwent a bilateral lung transplant via a transverse thoraco-sternotomy (clamshell) incision. The prior heart-lung transplant had been performed through a midline sternotomy, resulting in dense adhesions that were meticulously dissected and removed. Hilar dissection and the remaining transplant procedure were supported by veno-arterial extracorporeal membrane oxygenation (ECMO). The ascending aorta was cannulated with an 18 Fr fem-flex cannula, while venous drainage was achieved using a 21 Fr multistage venous cannula placed in the right atrium via the right common femoral vein. Hilar dissection, pneumonectomy, and anastomoses of the pulmonary artery and vein cuffs were performed as standard. Donor-to-donor bronchial anastomosis was completed with a 4-0 SH PDS suture, using continuous running sutures on the membranous portion and interrupted sutures on the cartilaginous section. Donor lung ischemia time was under 6 hours. Postoperatively, the patient required a tracheostomy but was successfully weaned from the ventilator by day 14. Patient was managed with triple immunosuppressive therapy—tacrolimus, mycophenolate, and prednisone—along with additional perioperative steroids. Tacrolimus trough levels were maintained within the target range of 6 to 10 mg/ml. The lower target for tacrolimus reflects the patient's long-term use of the drug and the presence of Scedosporium infection. Histopathology of the explanted lungs revealed severe tissue-invasive fungal pneumonia, obliterative bronchiolitis, and intimal fibrosis in scattered pulmonary arteries (Figure 2). Operative cultures grew Scedosporium spp. complex with diagnosis consistent with invasive pulmonary scedosporiosis.Figure 2. Explanted allograft lungs, International Society for Heart and Lung Transplantation (ISHLT) grade2 AXBXC1D1 and obstructive pneumonia. (A) While scattered peribronchiolar (A) and perivascular (B) chronic inflammation is suggestive of B1R and A2 rejection, respectively, those findings can also be seen in infectious processes; therefore, the explanted lungs are graded as AXBX. Also note multinucleated giant cells with cholesterol clefts (arrow A) that are suggestive of obstruction. (C) A bronchiole (arrow) is occluded by young fibrosis (note, fibroblasts occluding the airway lumen) consistent with obliterative bronchiolitis (grade C1 rejection). (D) A Verhoeff Van Gieson (VVG) stain highlights the single elastic lamina of the bronchiole (arrow). (E) This small airway is focally completely occluded by collagen fibrosis (also indicating grade C1 rejection). (F) A single elastic lamina outlines the occluded part of the bronchiole (arrow). Note, a pulmonary artery (arrowhead C) exhibits eccentric intimal fibrosis consistent with grade D1 rejection. This is better visualized using a VVG stain (D) which highlights the external and internal elastic lamina of the pulmonary artery. Magnification, hematoxylin & eosin (H&E) ×10 (A), ×20 (B, C), VVG ×4 (D), ×4 (E), VVG ×4 (F).Figure 2
There were no airway complications post surgery (Figure 3). Persistent isolation of Scedosporium from respiratory secretions post-transplant and histopathological confirmation of invasive disease in the explanted lungs prompted a treatment regimen comprising olorofim, inhaled voriconazole, and caspofungin during hospitalization of 1 month. This salvage regimen was selected based upon susceptibility testing (Table 1), as well as guideline recommendations supporting voriconazole as agent of choice for scedosporiosis. Upon discharge, she continued olorofim combined with aerosolized liposomal amphotericin B. By 3 months post-transplant, she transitioned to olorofim monotherapy. Bronchoalveolar lavage cultures initially grew Scedosporium for up to 6 weeks after olorofim initiation, subsequently yielding negative results. We observed no further microbiologic relapse, continued improvement in respiratory status and the patient continues to do well at 1-year follow-up.Figure 3. Post redo-lung transplant bronchoscopy images at 2 months follow-up, demonstrating healed suture line and healthy donor bronchial mucosa.Figure 3. Table 1Antimicrobial Susceptibility Profile of Scedosporium apiospermumTable 1. Antifungal agents testedMinimum Inhibitory Concentration (MIC)(mcg/ml)BreakpointsMicafungin0.03aCaspofungin≤0.015aTerbinafine>2aPosaconazole1aVoriconazole1aIsavuconazole8aAmphotericin B2aFosmanogepix≤0.008aIbrexafungerp2aOlorofim0.25aaNo established breakpoints available.
Discussion
Surgically, the concern in a redo-lung transplant after heart-lung transplant is the vascularity of the recipient's bronchial stump. After a heart-lung transplant in the immediate postoperative period, retrograde perfusion via the pulmonary circulation supports the blood supply to the donor bronchus. Over 1 to 2 months, collaterals arising from coronary circulation supply the donor carina and the proximal bronchus, and donor-to-donor bronchial anastomosis in such patients heals appropriately without complications.3 The redo-lung transplant was performed 7 years after the first transplant and the bronchus on the recipient's side was well collateralized. We did not encounter any airway complications in the postoperative period.
Medically, Scedosporium pulmonary infection poses significant treatment challenges owing to high-level resistance to common antifungals, with voriconazole and posaconazole considered first-line therapy.4 Despite improved survival with adjunctive surgery and treatment with voriconazole, mortality from invasive scedosporiosis remains high (up to 58%).5 A recent multinational survey demonstrated that pretransplant Scedosporium isolation was considered an absolute contraindication to lung transplant in 10% of centers.6 Fortunately, novel antifungal agents, including olorofim and fosmanogepix, have recently emerged as antimicrobials with in vitro and in vivo activity against rare molds, including Scedosporium and Lomentospora spp. Olorofim acts through reversible inhibition of the catalytic activity of dihydroorotate dehydrogenase, thereby preventing de novopyrimidine biosynthesis necessary for fungal cell wall synthesis.7 As noted in this case of treatment-refractory pulmonary Scedosporium infection, the use of olorofim as a combination antifungal regimen in the setting of redo-lung transplant may provide a novel salvage strategy for infection.
CRediT authorship contribution statement
Akshay Chauhan: Conceptualization, Methodology, Writing – original draft, Visualization. Nischal Ranganath: Writing – review & editing, John P. Scott: Writing – review & editing. Paschalis Vergidis: Writing – review & editing. Anja C. Roden: Writing – review & editing. Philip J. Spencer: Writing – review & editing. Mauricio A. Villavicencio: Writing – review & editing. Richard C. Daly: Writing – review & editing. Sahar A. Saddoughi: Supervision, Conceptualization, Methodology, Writing – review & editing, Project administration.
Disclosure statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
We acknowledge the lung and heart transplant teams who take excellent care of our transplant patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coster J.N.Chan E.G.Furukawa M.Pilewski J.M.Nguyen M.H.T.Sanchez P.G.Sequential redo-bilateral lung transplantation in recipient with prior heart-lung transplantation with tracheal anastomosis JTCVS Tech 1920231601633732435510.1016/j.xjtc.2023.03.017PMC 10268495 · doi ↗ · pubmed ↗
- 2Stewart S.Fishbein M.C.Snell G.I.Revision of the 1996 working formulation for the standardization of nomenclature in the diagnosis of lung rejection J Heart Lung Transplant 262007122912421809647310.1016/j.healun.2007.10.017 · doi ↗ · pubmed ↗
- 3Singh S.P.Nath H.Mc Giffin D.Kirklin J.Coronary tracheal collaterals after heart-lung transplant Am J Cardiol 922003149014921467559710.1016/j.amjcard.2003.08.071 · doi ↗ · pubmed ↗
- 4Lackner M.Hoog G.Sd Verweij P.E.Species-specific antifungal susceptibility patterns of Scedosporium and Pseudallescheria species Antimicrob Agents Chemother 562012263526422229095510.1128/AAC.05910-11PMC 3346635 · doi ↗ · pubmed ↗
- 5Husain S.Muñoz P.Forrest G.Infections due to Scedosporium apiospermum and Scedosporium prolificans in transplant recipients: clinical characteristics and impact of antifungal agent therapy on outcome Clin Infect Dis 40200589991561469710.1086/426445 · doi ↗ · pubmed ↗
- 6Rammaert B.Puyade M.Cornely O.A.Perspectives on Scedosporium species and Lomentospora prolificans in lung transplantation: results of an international practice survey from ESCMID fungal infection study group and study group for infections in compromised hosts, and European Confederation of Medical Mycology Transpl Infect Dis 212019 e 1314110.1111/tid.1314131283872 · doi ↗ · pubmed ↗
- 7Seyedmousavi S.Chang Y.C.Youn J.H.In vivo efficacy of olorofim against systemic scedosporiosis and lomentosporiosis Antimicrob Agents Chemother 652021 e 004342110.1128/aac.00434-21PMC 844812734252298 · doi ↗ · pubmed ↗