Successful wire placement into eccentric calcified plaque using intravascular lithotripsy
Hiroshi Abe, Dai Ozaki, Takashi Tokano, Tohru Minamino

TL;DR
Intravascular lithotripsy can safely help place wires into hard-to-treat, oddly shaped calcified artery plaques, improving PCI outcomes.
Contribution
Demonstrates a novel technique using IVL to safely manage eccentric calcified coronary lesions.
Findings
IVL enabled successful wire placement into an eccentric calcified plaque without complications.
Low-pressure balloon expansion after IVL facilitated wire embedding and improved procedural safety.
The approach may reduce the risk of coronary perforation in complex calcified lesions.
Abstract
Eccentric calcified lesions pose significant challenges in percutaneous coronary intervention (PCI), as they are associated with an increased risk of coronary artery perforation and suboptimal stent expansion. Moreover, long-term outcomes with drug-eluting stents (DESs) in these lesions are less favorable. Intravascular lithotripsy (IVL) has emerged as a treatment option for calcified lesions. However, its efficacy in managing eccentric calcified lesions remains uncertain. A 70-year-old male presented with angina starting a week ago. He was diagnosed with unstable angina, and a coronary computed tomography showed severe stenosis with calcified plaque in the right coronary artery. The coronary angiography confirmed severe, calcified, eccentric stenosis in the right coronary artery. Intravascular ultrasound (IVUS) showed an eccentric lesion with calcified plaque, and the diameter of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
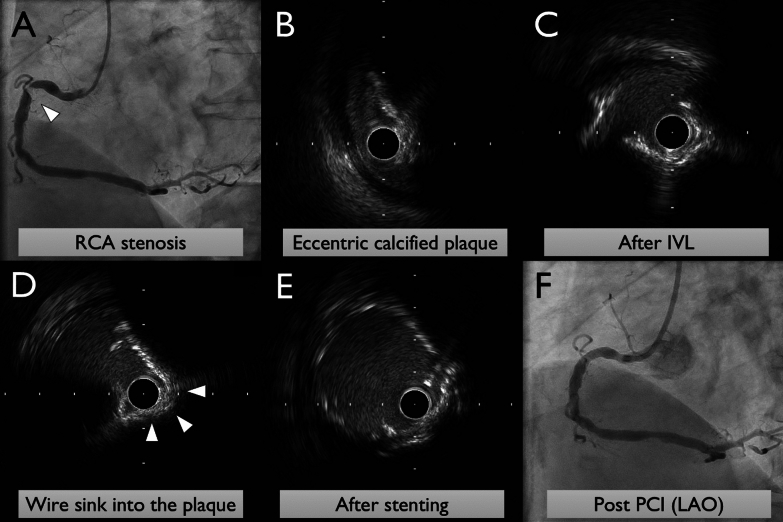 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics · Aortic aneurysm repair treatments
Background
Eccentric calcified lesions pose significant challenges in percutaneous coronary intervention (PCI), as they are associated with an increased risk of coronary artery perforation [1] and suboptimal stent expansion [2]. Moreover, long-term outcomes with drug-eluting stents (DESs) in these lesions are less favorable [3]. Intravascular lithotripsy (IVL) has emerged as a treatment option for calcified lesions. However, its efficacy in managing eccentric calcified lesions remains uncertain.
Case presentation
A 70-year-old male presented with angina starting a week ago. He was diagnosed with unstable angina, and a coronary computed tomography showed severe stenosis with calcified plaque in the right coronary artery. The coronary angiography confirmed severe, calcified, eccentric stenosis in the right coronary artery (Fig. 1A). Intravascular ultrasound (IVUS) showed an eccentric lesion with calcified plaque, and the diameter of the vessels before and after the lesion was about 6.2 mm on average (Fig. 1B). Due to the high risk of vessel perforation associated with rotablator and orbital atherectomy systems, intravascular lithotripsy was performed using a 3 mm balloon, without pre-dilatation using any other balloon. Oversizing may lead to balloon rupture in eruptive calcified plaque, and an undersized balloon aims to ensure emitter contact with the calcified segment. The crack formation was observed on IVUS. IVUS image shows both the guidewire and IVUS catheter being partially embedded within the concavity of the calcified nodule, and a 4 mm balloon was used for low-pressure expansion to expand the calcified crackles (Fig. 1C). This allowed the wire to sink into the calcified plaque and enabled balloon expansion within the calcified region (Fig. 1D). The risk of coronary perforation was deemed reduced, and a 5 mm × 15 mm drug-eluting stent was successfully placed (Fig. 1E) without complications (Fig. 1F).Fig. 1. Images of coronary angiography and intravascular ultrasound during primary percutaneous coronary intervention. A Coronary angiography (CAG) showing severe, calcified, eccentric stenosis in the right coronary artery. B Intravascular ultrasound (IVUS) image reveals the eccentric calcified lesion. C The guidewire and IVUS catheter are partially embedded within the concavity of the calcified nodule. D IVUS image after expansion using a 4 mm balloon, showing expanded calcified crackles and the wire sinking into the calcified plaque. E Successful expansion and placement of a 5 mm × 15 mm drug-eluting stent. F Final CAG demonstrated good stent expansion
Conclusions
The approach for eccentric calcified lesions remains challenging. However, as demonstrated in this case, achieving relatively safe treatment of eccentric calcified plaques may be possible depending on how cracks form within the plaque. The additional balloon dilation following IVL could allow the wire to enter the calcified plaque, enhancing procedural safety and effectiveness.