History of Oral Mucosal Lesions in Oral Squamous Cell Carcinoma Patients
Arvi Keinänen, Johanna Snäll, Jaana Hagström, Johanna Uittamo

TL;DR
This study found that about a third of oral cancer patients had a history of oral mucosal lesions, and those with prior dysplasia were more likely to be diagnosed during routine check-ups.
Contribution
The study provides new insights into the relationship between prior mucosal lesions and the detection mode of oral squamous cell carcinoma.
Findings
32% of patients had a history of oral mucosal lesions before OSCC diagnosis.
Heavy alcohol users were less likely to have prior mucosal lesions or dysplasia.
Patients with prior dysplasia were more likely to be diagnosed during routine appointments.
Abstract
To evaluate the occurrence of previous mucosal dysplasia in patients with oral squamous cell carcinoma (OSCC) and to charaterise patient profile, types of previous oral mucosal lesions, and care-seeking in relation to earlier mucosal findings. Retrospective data of OSCC patients with a primary tumour were collected. The primary outcome variable was any history of oral mucosal findings; the secondary outcome variable was a history of previous oral mucosal dysplasia. The primary predictor variable was the mode of seeking treatment. Patient and tumour-related variables were compared between patients with and without anamnestic mucosal changes or findings. A total of 528 patients were included in the study. Of these patients, 169 (32.0%) had a history of an oral mucosal lesion. Oral mucosal dysplasia was detected in 34 patients (6.4%) before the OSCC diagnosis. Patients who had a history…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
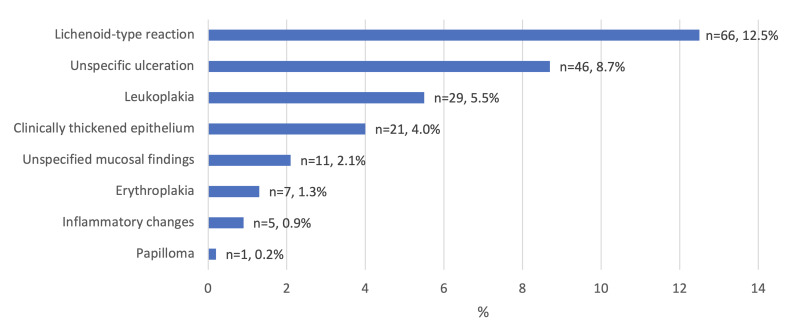 Fig 1
Fig 1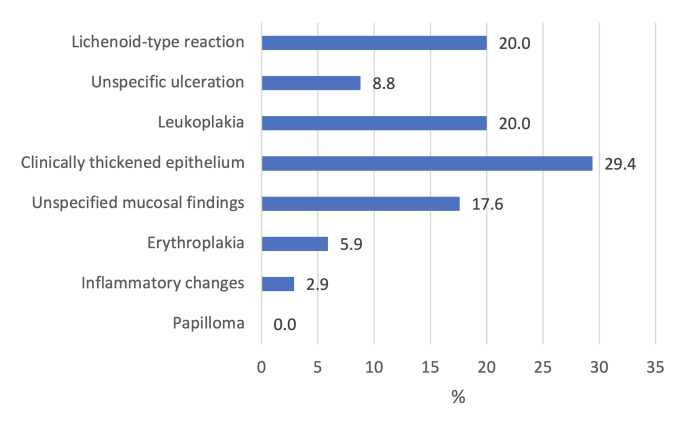 Fig 2
Fig 2|
Univariate |
Multivariate | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Previous oral mucosal finding present |
Previous oral mucosal finding present | ||||||||
|
95% CI for OR |
95% CI for OR | ||||||||
|
OR |
Lower |
Upper |
p-value |
OR |
Lower |
Upper |
p-value | ||
|
|
1.005 |
0.990 |
1.019 |
0.525 |
Heavy alcohol use | ||||
|
Sex (reference male) |
Yes |
0.350 |
0.215 |
0.571 |
<0.001 | ||||
|
Female |
2.183 |
1.504 |
3.166 |
<0.001 |
Incidental findings | ||||
|
|
Yes |
2.671 |
1.704 |
4.187 |
<0.001 | ||||
|
Current smoker |
0.298 |
0.202 |
0.439 |
<0.001 | |||||
|
Heavy alcohol use | |||||||||
|
Yes |
0.364 |
0.225 |
0.587 |
<0.001 | |||||
|
| |||||||||
|
Tis-T2 |
3.520 |
2.253 |
5.501 |
<0.001 | |||||
|
Site | |||||||||
|
Tongue | |||||||||
|
Yes |
1.518 |
1.049 |
2.195 |
0.027 | |||||
|
| |||||||||
|
Yes |
0.759 |
0.473 |
1.217 |
0.252 | |||||
|
| |||||||||
|
Yes |
0.487 |
0.276 |
0.860 |
0.013 | |||||
|
| |||||||||
|
Yes |
0.538 |
0.215 |
1.346 |
0.185 | |||||
|
Buccal | |||||||||
|
Yes |
2.039 |
1.065 |
3.904 |
0.032 | |||||
|
| |||||||||
|
General dentist, oral surgeon, or oral and maxillofacial surgeon |
2.081 |
1.373 |
3.156 |
<0.001 | |||||
|
| |||||||||
|
Yes |
2.566 |
1.656 |
3.976 |
<0.001 |
|
Univariate |
Multivariate | ||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Previous oral mucosal dysplasia present |
Previous oral mucosal dysplasia present | ||||||||
|
95% CI for OR |
95% CI for OR | ||||||||
|
OR |
Lower |
Upper |
p-value |
OR |
Lower |
Upper |
p-value | ||
|
|
1.009 |
0.982 |
1.037 |
0.505 |
Heavy alcohol use | ||||
|
Sex (reference male) |
Yes |
0.235 |
0.070 |
0.795 |
0.020 | ||||
|
Female |
1.122 |
0.557 |
2.261 |
0.747 |
Incidental findings | ||||
|
|
Yes |
6.195 |
3.004 |
12.774 |
< 0.001 | ||||
|
Current smoker |
0.329 |
0.151 |
0.720 |
0.005 | |||||
|
Heavy alcohol use | |||||||||
|
Yes |
0.250 |
0.075 |
0.830 |
0.024 | |||||
|
| |||||||||
|
Tis-T2 |
4.337 |
1.504 |
12.508 |
0.007 | |||||
|
Site | |||||||||
|
Tongue | |||||||||
|
Yes |
1.406 |
0.694 |
2.846 |
0.344 | |||||
|
| |||||||||
|
Yes |
0.844 |
0.340 |
2.095 |
0.715 | |||||
|
| |||||||||
|
Yes |
0.690 |
0.237 |
2.012 |
0.497 | |||||
|
| |||||||||
|
Yes |
0.504 |
0.067 |
3.823 |
0.508 | |||||
|
| |||||||||
|
Yes |
1.195 |
0.349 |
4.096 |
0.776 | |||||
|
| |||||||||
|
General dentist, oral surgeon, or oral and maxillofacial surgeon |
3.098 |
1.178 |
8.148 |
0.022 | |||||
|
| |||||||||
|
Yes |
6.009 |
2.937 |
12.294 |
< 0.001 |
|
| ||
|
Range |
19–98 | |
|
Mean/Median |
66.2/66.0 | |
|
No. of patients |
% of 528 | |
|
| ||
|
Male |
309 |
58.5 |
|
Female |
219 |
41.5 |
|
| ||
|
Non-smoker |
261 |
49.4 |
|
Current smoker |
267 |
50.6 |
|
| ||
|
No |
387 |
73.3 |
|
Yes |
141 |
26.7 |
|
| ||
|
Tis-T2 |
343 |
65.0 |
|
T3-4 |
185 |
35.0 |
|
| ||
|
Tongue |
269 |
50.9 |
|
Gingiva |
106 |
20.1 |
|
Floor of mouth |
84 |
15.9 |
|
Palate |
29 |
5.5 |
|
Buccal |
40 |
7.6 |
|
| ||
|
General dentist, oral surgeon, or oral and maxillofacial surgeon |
351 |
66.5 |
|
Other |
177 |
33.5 |
|
| ||
|
No |
423 |
80.1 |
|
Yes |
105 |
19.9 |
|
| ||
|
No |
359 |
68.0 |
|
Yes |
169 |
32.0 |
|
| ||
|
No |
494 |
93.6 |
|
Yes |
34 |
6.4 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Oral and gingival health research · Cancer Diagnosis and Treatment
Oral epithelial dysplasia is described as a growth anomaly produced by abnormal or atypical epithelial proliferation, resulting in a lesion with disturbed differentiation and maturation of epithelial tissue. These epithelial changes in the mucosa have a higher rate of developing into oral squamous cell carcinoma (OSCC) than does healthy mucosa.^ 11,23,39,41 ^ Clinically, dysplasia typically occurs as leukoplakia, erythroplakia, or erythroleukoplakia, but epithelial dysplasia is not always present in these benign lesions.^ 6,19,23 ^ Oral epithelial dysplasia is present in first biopsy in 40% of leukoplakia, 91% of erythroplakia, and < 10% of proliferative leukoplakia lesions.^ 33,38 ^ Oral lichen planus has been considered a premalignant lesion, although controversy about its classification exists in the literature.^ 36 ^ Other known oral mucosa-related risk factors for OSCC are human papilloma virus, candida, trauma caused by ill-fitting prostheses or other continuous mechanical irritation, and possibly autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome.^ 1,5,8,15,30 ^
OSCC comprises 90% of all oral carcinomas.^ 13,37 ^ Smoking and alcohol consumption are the main risk factors for development of OSCC-preceding dysplasia.^ 23 ^ Of oral epithelial dysplasia, 12.1% develops into malignancy.^ 21,23 ^ The OSCC disease-specific survival beyond 3 years is approximately 70% in patients with stage I tumours, but only 60% in patients with stage III or IV tumours.^ 7 ^ The 5-year mortality rate of OSCC is close to 50%.^ 16 ^
Thus, for early OSCC diagnosis, the detection, diagnosis, and follow-up of mucosal changes are essential. However, different mucosal changes are found in the oral mucosa, some of which are clinically similar and may mislead clinicians.^ 42 ^ Thus, oral disease diagnostics is challenging, especially for conditions that require specialised medical care. According to an Italian study, 55% of the referrals for specialised medical care lacked a clinical diagnosis.^ 31 ^
This study focused on early oral mucosal dysplasia in patients with OSCC. We examined patient profiles, the types of early oral lesions, and how patients sought care based on these earlier findings. We hypothesised that patients with dysplasia are often diagnosed with OSCC during routine healthcare visits and at an earlier stage of the disease.
MATERIALS AND METHODS
This study was approved by the Internal Review Board of the Head and Neck Centre, Helsinki University Central Hospital, Finland (HUS/66/2018).
Patient Material
Patient records from January 2016 to December 2020 at Helsinki University Hospital, Helsinki, Finland, were evaluated retrospectively. Patient data were retrieved from the multidisciplinary Head and Neck Tumour Board of Helsinki University Hospital, which maintains patient information on all patients treated in the university hospital region who have a primary diagnosis of OSCC.
Inclusion and Exclusion Criteria
All patients with a primary OSCC diagnosis evaluated at Helsinki University Hospital were included in the study. Patients with a history of previous oral cancer were excluded.
Study Design
The primary outcome variable was a history of earlier oral mucosal changes or findings. History of oral mucosal lesions was evaluated from patient records in the hospital database, which were based on anamnestic information and referral details. Oral mucosal lesions were divided into the following eight groups: lichenoid-type reaction (including lichen planus and lichenoid), leukoplakia, erythroplakia, clinically thickened epithelium, unspecific ulceration, inflammatory changes, papilloma, and unspecified mucosal findings (including benign findings without a specific description).^ 40 ^ Our secondary outcome variable was history of oral mucosal dysplasia.
The primary predictor variable was the mode of seeking OSCC treatment, defined as incidental (i.e., tumour noted in conjunction with routine care or control appointments) or other.
Explanatory variables were age, sex, smoking, heavy alcohol use, and tumour-related variables (tumour size, tumour site, and referring physician).
Patients were stratified by smoking status into non-smokers (non-smokers and former smokers who not smoked for ≥ 5 years) and current and former smokers (current smokers and former smokers who had not smoked for < 5 years).^ 17 ^ Alcohol use was determined according to the following Finnish Current Care Guidelines consumption limits for heavy alcohol use: ≥ 23 doses (≥ 287.5 g alcohol) per week for men and ≥ 12 doses (≥ 150 g alcohol) per week for women, as suggested by the Finnish Working Group for treatment of alcohol abuse.^ 14 ^ Tumour size was defined according to T categorisation as Tis-T2 (Tis, T1, or T2) or T3-4 (T3 or T4) based on TNM Staging of Lip and Oral Cavity cancers – AJCC 7th edition^ 10 ^ and 8th edition^ 2,22 ^ which were valid at the time of diagnosis.
Statistical Analysis
Associations between explanatory and predictor variables and outcome variables were assessed with logistic regression analysis. The Hosmer and Lemeshow goodness-of-fit test was used to assess logistic regression analyses. Before conducting multiple logistic regression analyses, Cramer’s V-test was used to detect possible multicollinearity of categorical explanatory variables. The significance level was set at 0.05. SPSS 28.0 (IBM; Armonk, NY, USA) and used for all statistical analyses.
RESULTS
Patient Material
Of 682 evaluated OSCC patients, 154 were excluded (119 patients had previous oral cancer and 35 had missing data from preceding visits). Thus, 528 patients with primary OSCC were included in the final analyses.
Median patient age was 66.2 years. Patients were more often men (58.5%). Half of the patients were smokers (50.6%) and 26.7% reported a history of heavy alcohol use. In all, 169 of 528 patients (32.0%) had a history of oral mucosal lesion (Table 1). The types and occurrence of one or more earlier mucosal lesions are presented in Fig 1. Dysplasia was found prior to malignancy in 6.4% of OSCC patients. History of oral mucosal lesions in OSCC patients with previously found dysplasia are presented in Fig 2.
Previous oral mucosal findings of 528 oral squamous cell carcinoma patients. Of 169 patients with anamnestic oral mucosal changes or findings, 66 had a lichenoid-type reaction, including patients with a history of oral lichen planus (n = 48, 9.1%).
Previous oral mucosal findings of oral squamous cell carcinoma patients with dysplasia (n = 34).
Univariate logistic regression analysis showed that OSCC in patients with an earlier oral mucosal finding was 2.6 times more likely to be found incidentally (p < 0.001). Moreover, a previously detected oral mucosal lesion was associated with female sex (odds ratio [OR] 2.183, p < 0.001). Earlier oral mucosal lesions were found statistically significantly less often in smokers (OR 0.298, p < 0.001), in patients with a history of heavy alcohol use (OR 0.364, p < 0.001), and in patients with tumours of the floor of the mouth (OR 0.487, p = 0.013). Patients with anamnestic mucosal lesions had statistically significantly smaller tumours (Tis-T2 tumours OR 3.520, p < 0.001) and were referred to further care more often by oral health professionals (OR 2.081, p < 0.001) (Table 2). Previous diagnoses of dysplasia were statistically significantly less often detected in smokers (OR 0.329, p = 0.005) and in patients with a history of heavy alcohol use (OR 0.250, p = 0.024). In patients with previous dysplasia, OSCC was found incidentally statistically significantly more often than as a result of the patient actively seeking treatment (OR 6.009, p < 0.001). Dysplasia was statistically significantly associated with smaller tumours (OR 4.337, p = 0.007), and patients with preceding dysplasia were referred to further care more often by oral health professionals (OR 3.098, p = 0.022) (Table 3).
Both multiple logistic regression analyses for anamnestic oral mucosal lesions and previous oral mucosal dysplasia included the variables “heavy alcohol use” and “incidental finding”. OSCC in patients with a history of oral mucosal lesions was 2.7 times more often found incidentally (adjusted OR [aOR] 2.671, 95% confidence interval [CI] 1.704–4.187, p < 0.001). In addition, anamnesis of oral mucosal lesion was independently associated with heavy alcohol use (aOR 0.350, 95% CI 0.215–0.571, p < 0.001) (Table 2). OSCC in patients with previously detected dysplasia was less often found in patients with a history of heavy alcohol use (aOR 0.235, CI 0.070-0.795, p = 0.020) and was more often found incidentally (aOR 6.195, CI 3.004–12.774, p < 0.001) (Table 3).
DISCUSSION
This study focused on earlier mucosal lesions of OSCC patients, patient profile, and care-seeking behaviour in relation to mucosal lesion history. We hypothesised that OSCC is often diagnosed in routine appointments in patients with a history of oral mucosal findings and previous oral mucosal dysplasia. Our hypothesis was confirmed. Suspicion of oral cancer was thus established more often in connection with a routine examination or an oral mucosal lesion follow-up visit. In addition, occurrence of earlier mucosal lesions was as high as 32.0% in OSCC patients. On the other hand, oral cancer is always preceded by a premalignant stage, but previous oral mucosal dysplasia was found in only 6.4% of these patients.^ 9,27,34 ^ These findings emphasise the need for more frequent identification of pre-malignant lesions.
Tumours of patients with a history of oral mucosal findings were more often Tis-T2 tumours and smaller than those of patients without preceding lesions. This is very likely the result of a follow-up of previous findings, which led to the early detection of OSCC. These patients did not necessarily have typical symptoms, such as pain, which would cause patients to seek treatment on their own, as described previously.^ 7,16,18,29,42 ^
In patients with a history of oral mucosal lesions, OSCC was more often located on the tongue and buccally. On the other hand, the floor of the mouth was less often the location of the earlier mucosal finding (Table 2). This is an interesting result, as the most typical locations for malignant findings in OSCC are the tongue and floor of the mouth.^ 3,24,32,35 ^ It is possible that clinicians more easily notice changes in the tongue and buccal mucosa and therefore these findings are more likely to be followed-up. Another explanation might be that cancer of the floor of the mouth is highly associated with alcohol use,^ 12 ^ which affects care-seeking, as we found. Treatment becomes increasingly challenging as the cancer progresses. Ensuring that these patients receive treatment before extensive tumour growth and spread is paramount. This could be accomplished by, for instance, public awareness campaigns, direct health advice given to this target group, and training of health professionals who meet these patients for oral examinations.
In our study, the most common observed previous lesion was the lichenoid-type reaction, which occurred in 12.5% of all OSCC patients (Fig 1) and in 20.0% of OSCC patients with previous oral mucosal dysplasia (Fig 2). The lichen planus is pathologically similar to the lichenoid reaction.^ 32,35 ^ Oral lichen planus and oral lichenoid reaction can both undergo malignant transformation. Malignant transformation may be linked to increased proliferative activity and decreased apoptosis rate of epithelial cells, which the inflammatory infiltrate may influence.^ 4 ^ Interestingly, in this study, clinically premalignant findings, oral leukoplakia and oral erythroplakia, were not the most commonly observed previous lesions in OSCC patients or in patients who had previous oral mucosal dysplasia.^ 20,26,28,33 ^ Because of these findings and the similarity of changes in the oral cavity, a biopsy is needed to confirm the diagnosis.^ 25,31 ^
In this study, dentists or oral and maxillofacial surgeons referred most of the patients (66.5%) for further OSCC care. These findings highlight the role of dentist, oral surgeon, or oral and maxillofacial surgeons in early OSCC diagnosis. The clinically important follow-up should be conducted by oral healthcare professionals in routine control appointments and in connection with other care.
The main limitation of this study is its retrospective design. Thus, information on the history of oral findings may have been missing due to incompleteness of the referral or because no preceding finding was made. However, based on our data, oral findings occurred in at least 32.0% of OSCC patients, and 6.4% of OSCC patients had previously-detected oral mucosal dysplasia. In addition, previous oral mucosal lesions were not always at the same site as the developing OSCC, and not all mucosal findings were premalignant. This is an important topic for further research, but larger and more treatment-oriented datasets are needed for comprehensive results.
CONCLUSIONS
The findings of this study highlight the need for follow-up of oral mucosal changes for early detection of precancerous dysplasia, as only 6.4% of OSCC patients had prior diagnoses of oral mucosal dysplasia. This calls for thorough examinations and early biopsies, emphasising the crucial role of dentists in identifying premalignant lesions and OSCC. Notably, 66.5% of OSCC cases were referred by dental professionals, underscoring their importance in detecting asymptomatic changes to identify OSCC early.
ACKNOWLEDGEMENTS
The Helsinki University Hospital Research Fund financially supported this work. Open access was funded by Helsinki University Library.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alnuaimi AD Wiesenfeld D O’Brien-Simpson NM Reynolds EC Mc Cullough MJ Oral Candida colonization in oral cancer patients and its relationship with traditional risk factors of oral cancer: A matched case-control study Oral Oncol 20155121391452549892110.1016/j.oraloncology.2014.11.008 · doi ↗ · pubmed ↗
- 2Amin MB Greene FL Edge SB Compton CC Gershenwald JE Brookland RK et al The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population‐based to a more “personalized” approach to cancer staging CA Cancer J Clin 201767293992809484810.3322/caac.21388 · doi ↗ · pubmed ↗
- 3Bánóczy J Follow-up studies in oral leukoplakia J Maxillofac Surg 19775697526535410.1016/s 0301-0503(77)80079-9 · doi ↗ · pubmed ↗
- 4Bascones-Ilundain C, Gonzalez-Moles MA, Esparza-G N, Gil-Montoya JA, Bascones-Mart A. Importance of apoptotic mechanisms in inflammatory infiltrate of oral lichen planus lesions. Anticancer Res 2006;26(1A):357-362.16475718 · pubmed ↗
- 5Bektas-Kayhan K Karagoz G Kesimli MC Karadeniz AN Meral R Altun M et al Carcinoma of the tongue: a case-control study on etiologic factors and dental trauma Asian Pacific J Cancer Prev 20141552225222910.7314/apjcp.2014.15.5.222524716961 · doi ↗ · pubmed ↗
- 6Bisht R Singh A Sikarwar V Darbari A Study over the clinical picture and histopathology of leukoplakia and to establish the correlation between causative factors in the patients of Garhwal hill region Nat J Maxillofac Surg 20134217710.4103/0975-5950.127647 PMC 396189124665172 · doi ↗ · pubmed ↗
- 7Boeve K Melchers LJ Schuuring E Roodenburg JL Halmos GB Van Dijk BA et al Addition of tumour infiltration depth and extranodal extension improves the prognostic value of the pathological TNM classification for early‐stage oral squamous cell carcinoma Histopathol 201975332933710.1111/his.13886 PMC 685168431021008 · doi ↗ · pubmed ↗
- 8Bruserud Ø Costea D-E Laakso S Garty B-Z Mathisen E Mäkitie A et al Oral tongue malignancies in autoimmune polyendocrine syndrome type 1Front Endocrinol 2018946310.3389/fendo.2018.00463 PMC 610968930177913 · doi ↗ · pubmed ↗