A Case Series and Literature Review of Angiosarcoma With Malignant Effusion—A Challenging Cytologic Diagnosis With Dire Prognostic Implications
Jamie C. Y. Lam, Iris Y. H. Liu, Joanna K. M. Ng, Joshua J. X. Li

TL;DR
This paper discusses the challenges of diagnosing angiosarcoma with malignant effusion, highlighting its similarity to other cancers and poor prognosis.
Contribution
The paper presents a case series and literature review to improve diagnostic approaches for angiosarcoma with malignant effusion.
Findings
Angiosarcoma with malignant effusion is difficult to distinguish from metastatic adenocarcinoma.
Immunocytochemical markers and clinical context are crucial for accurate diagnosis.
The condition has a poor prognosis, emphasizing the need for early and accurate detection.
Abstract
Angiosarcoma with malignant effusion is an uncommon yet clinically aggressive presentation, which poses as a diagnostic pitfall with its overlapping cytomorphologic features with metastatic adenocarcinoma. In this article, two cases reported in the literature were reviewed for cytology, immunocytochemistry, and clinical course. Key clinical hints, useful cytological features, and immunocytochemical markers in the diagnostic approach of this entity are presented.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
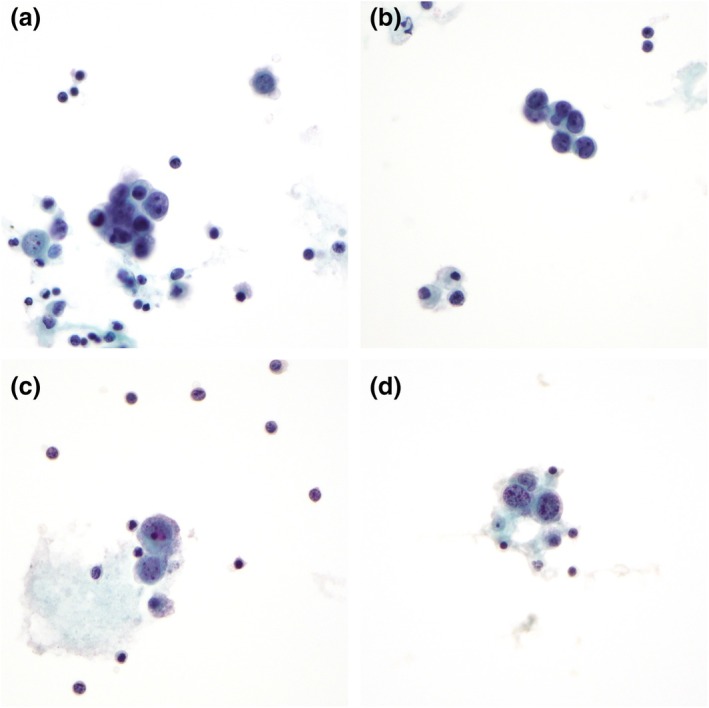 FIGURE 1
FIGURE 1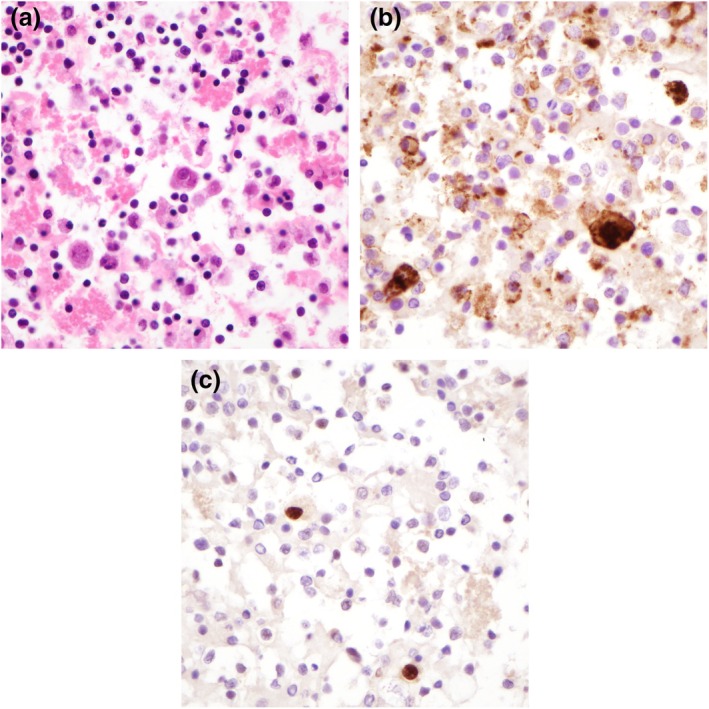 FIGURE 2
FIGURE 2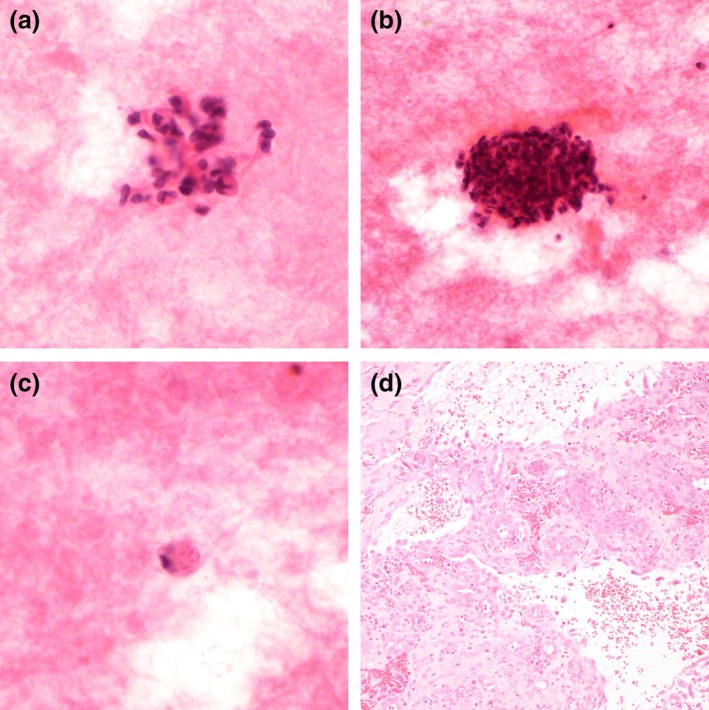 FIGURE 3
FIGURE 3| No | Age | Sex | Diagnosis | Primary | Effusion cavity | Effusion on presentation | Treatment | Outcome | Cytologic diagnosis | |
|---|---|---|---|---|---|---|---|---|---|---|
| Current series | 1 | 52 | F | Radiation‐associated angiosarcoma | Oropharynx/larynx | Pleural | No (5 months after diagnosis) | Chemotherapy (taxotere and cyclophosphamide) | DOD at 8 months | C5 |
| 2 | 94 | M | Angiosarcoma | Scalp | Pleural | No (during investigation) | Chest drain and pleurodesis | DOD at 1 month | C3 | |
| Dörr‐Jerat et al. [ | 3 | 73 | F | Epithelioid angiosarcoma | Unknown | Pleural | Yes | Chest drain | Not mentioned | C2 |
| Li et al. [ | 4 | 53 | F | Primary cardiac angiosarcoma | Heart | Pericardial | Yes | Pericardial window | DOD at 6 months | C5 |
| Ogino et al. [ | 5 | 67 | M | Radiation‐associated angiosarcoma | Unknown | Pleural | Yes (8 years after radiotherapy) | Chemotherapy | DOD | C5 |
| Kiwaki et al. [ | 6 | 60 | M | Primary cardiac angiosarcoma | Unknown | Pericardial | Yes | Defaulted | DOD at 13 months | C2 |
| Senthil Kumaran et al. [ | 7 | 41 | M | Angiosarcoma | Unknown | Pericardial | Yes | Chemotherapy (paclitaxel) | DOD at 2 months | C3 |
| Sharma et al. [ | 8 | 66 | M | Angiosarcoma | Scalp | Pleural | No (11 months after diagnosis) | Chemotherapy and radiotherapy | DOD | C5 |
| 9 | 82 | M | Angiosarcoma | Acetabulum | Pleural | Yes | Radiotherapy | DOD | C5 | |
| 10 | 73 | F | Angiosarcoma | Shin | Pleural | No (7 months after diagnosis) | Resection and radiotherapy | DOD | C5 | |
| 11 | 81 | F | Angiosarcoma | Breast | Pleural + peritoneal | No (23 months after diagnosis) | Mastectomy and chemotherapy | DOD | C5 | |
| 12 | 77 | F | Angiosarcoma | Breast | Pleural | No (11 months after diagnosis) | Mastectomy and chemotherapy | DOD | C5 | |
| 13 | 73 | M | Angiosarcoma | Axilla | Pleural | No (2 months after diagnosis) | Amputation | Lost to follow‐up | C5 | |
| Burns et al. [ | 14 | 23 | F | Primary cardiac angiosarcoma | Heart | Pericardial | Yes | Pericardial window and chemotherapy (adriamycin + ifosfamide, then gemcitabine + docetaxel) | AWD at 9 months | C2 |
| Durani et al. [ | 15 | 62 | M | Epithelioid angiosarcoma | Unknown | Pleural | Yes | Thoracentesis | Not mentioned | C2 |
| Geller et al. [ | 16 | 46 | M | Angiosarcoma | Not mentioned | Pleural | Not mentioned | Not mentioned | Not mentioned | C5 |
| Chen et al. [ | 17 | 69 | M | Angiosarcoma | Unknown | Pleural | Yes | Thoracentesis | DOD at 1 month | C2 |
| Riles et al. [ | 18 | 33 | M | Angiosarcoma | Unknown | Pericardial | Yes | Surgical exploration | DOD at 1 month | C2 |
| El‐Osta et al. [ | 19 | 64 | M | Primary cardiac angiosarcoma | Heart (right atrium) | Pericardial | Yes | Resection and adjuvant chemotherapy (paclitaxel) | DOD at 5 months | C1 |
| Saqi et al. [ | 20 | 41 | M | Primary cardiac angiosarcoma | Heart (right atrium) | Pericardial | Yes | Not mentioned | Not mentioned | C5 |
| Boucher et al. [ | 21 | 50 | F | Epithelioid angiosarcoma | Not mentioned | Pleural | Yes | Not mentioned | Not mentioned | C4 |
| Randall et al. [ | 22 | 52 | M | Angiosarcoma | Unknown | Pericardial | Yes | Pericardiocentesis | DOD at 2 months | C2 |
| Ott et al. [ | 23 | 60 | M | Angiosarcoma | Lung | Pleural | Yes | Resection | DOD at 2 months | C1 |
| Source | Cytomorphology | Other cytologic features | Immunocytochemistry |
|---|---|---|---|
| Current series | Single or small clusters of cells with marked nuclear irregularity, including nuclear folding, indentation and kidney‐bean‐like appearance, with nuclear enlargement and hyperchromasia | Vasoformative features—intracytoplasmic multivacuolation, lumina formation and close association with polymorphs | CD31+, ERG+; BerEp4−, calretinin− |
| Li et al. [ | Large discohesive cells with enlarged nuclei, severe nuclear membrane irregularity and nuclear pleomorphism and macronucleoli | CD31+, D2‐40+, desmin+, ERG+, factor VIII+; AE1/3−, CD45−, heppar1−, MOC31−, myogenin−, SALL4− | |
| Ogino et al. [ | Aggregates of cells with eccentric nuclei and prominent nucleoli | ||
| Geller et al. [ | Single or three‐dimensional clusters, multiple prominent or bar‐shaped nucleoli and chromatin strands, and abnormal mitoses | Vasoformative features—hemophagocytosis, cytoplasmic lumina/vacuoles containing red blood cells/neutrophils and endothelial wrapping | |
| Saqi et al. [ |
Small clusters of cells with scalloped borders Single pleomorphic epithelial‐appearing round cells with nuclei two to three times the size of the small lymphocytes, high nuclear‐to‐cytoplasmic ratios, round vesicular nuclei, and prominent nucleoli Isolated multinucleate tumor giant cells | Vasoformative features—erythron(hemo)phagocytosis and intracytoplasmic vacuoles | CD31+, CD34+ (focal); cytokeratin−, desmin−, EMA−, HHF‐35− (in corresponding tissue biopsy) |
| Boucher et al. [ | Loosely cohesive groups to single epithelioid, polygonal cells, with hyperchromasia, irregularly distributed coarse chromatin, single to multiple nuclei that are oval to round with marked pleomorphism, high nuclear–cytoplasmic ratio, and conspicuous eosinophilic macronucleoli | Low cellularity with bloody background | CD31+; cytokeratin− (in corresponding tissue biopsy) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Cardiac tumors and thrombi · Sarcoma Diagnosis and Treatment
Introduction
1
Diagnosis of malignant effusion is dependent on cytologic assessment. A broad range of causes underlie malignant effusion [1], and the plethora of possible diagnoses share multiple overlapping cytologic features. Non‐carcinomatous neoplasms, including lymphomas, melanomas, and sarcomas, are less frequently encountered differentials, which pose diagnostic challenges. In the case of sarcomas, specific cytomorphologic features may be lacking [2]. This is particularly problematic for angiosarcomas, as vasoformation can be mistaken for glandular differentiation and thus misinterpreted as adenocarcinomas [3, 4]. Such an issue is amplified by the frequent lack of correlation and examination of the primary tumor site in metastatic effusions and the differences in cytomorphology in exfoliative cytology compared to direct fine‐needle aspiration or tissue biopsy of primary lesions [5]. In this article, we present two cases of angiosarcoma with malignant effusion with a review of such cases available in the literature, aiming to detail the cytology, immunocytochemistry, and clinical course of angiosarcoma with malignant effusion for recognition of this uncommon but diagnostically significant entity.
Case Report
1.1
Case 1
1.1.1
A 52‐year‐old woman with a history of nasopharyngeal carcinoma, treated with chemotherapy and radiotherapy presented with bloody sputum. Positron emission tomography–computed tomography revealed an extensive tumor involving the oropharynx and larynx with suspected metastatic lung lesions. Biopsy confirmed the diagnosis of angiosarcoma, and the patient started palliative chemotherapy (taxotere and cyclophosphamide). The patient completed four cycles of chemotherapy with radiological response. However, the patient developed left‐sided pleural effusion with desaturation. Drainage was performed and the pleural fluid was sent for cytologic examination. The patient deteriorated and succumbed 8 months after presentation.
Cytospin preparation is of moderate cellularity and showed clusters of malignant cells in mostly small groups with ovoid outline (Figure 1a). The malignant cells demonstrated marked nuclear enlargement and irregularity with kidney‐bean‐like appearance (Figure 1b). Single to multiple nucleoli, including macronucleoli, were noted (Figure 1c). In the background were mononuclear cells and polymorphs with some clusters of malignant cells closely associated with polymorphs, suggestive of vascular lumen formation (Figure 1d). A cell block was prepared, and the malignant cells were immunoreactive to vascular markers (CD31 and ERG) (Figure 2).
Case 1. (a) Small clusters of ovoid malignant cells, pap stain, 400× magnification. (b) Irregular nuclei with kidney‐bean‐like appearance, pap stain, 400× magnification. (c) Single to multiple nucleoli and macronucleoli, pap stain, 400× magnification. (d) Malignant cells in close association with polymorphs and suggestion of lumen formation, pap stain, 400× magnification.
Cell block (agar block method) and immunocytochemistry. (a) Moderately cellular cell block preparation with malignant cells in a background of inflammatory cells, 400× magnification. (b) CD31, 400× magnification. (c) ERG, 400× magnification.
Case 2
1.1.2
A 94‐year‐old man presented with a right forehead mass for 6 months rapidly increasing in size, and with contact bleeding. He was seen by a dermatologist with high clinical suspicion of angiosarcoma. Initial skin biopsy from the forehead was non‐informative and before a repeat biopsy was performed, the patient developed left‐sided pneumothorax. Chest drain was inserted with pleural fluid sent for cytologic examination. Subsequent biopsy confirmed the diagnosis of angiosarcoma. Magnetic resonance imaging showed extensive tumor extension with orbital involvement. The patient deteriorated and succumbed 1 month after presentation.
On the smears, small clusters and singly spindled malignant cells were seen. The malignant cells displayed marked nuclear hyperchromasia and irregularity with nuclear folding and indentation (Figure 3a). Mitotic and apoptotic figures were noted (Figure 3b). Rare malignant cells with intracytoplasmic multivacuolation were noted (Figure 3c). These nuclear and cytoplasmic features corresponded with that of the issue biopsy (Figure 3d).
Case 2. (a) Spindled malignant cells with markedly irregular folded and indented nuclei, H&E, 400× magnification. (b) Mitotic and apoptotic figures, H&E, 400× magnification. (c) Intracytoplasmic multivacuolation, H&E, 400× magnification. (d) Corresponding tissue biopsy, 100× magnification.
Literature Review
1.2
Literature search using the medical subject headings (MeSH) “angiosarcoma,” “pleural effusion,” “peritoneal effusion,” and “cytology” yielded 16 relevant articles [3, 4, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19] describing 21 cases of angiosarcoma with malignant effusion. There were 5 cases of primary cardiac angiosarcoma, 3 epithelioid angiosarcomas, 1 radiation‐associated angiosarcoma, and 12 angiosarcomas not otherwise specified involving the pleural cavity only in 12 cases, and the pericardial cavity in 8. There was one case involving the peritoneal cavity, which also involved the pleural cavity. Of the 15 cases with follow‐up data, only one patient was alive with disease at 9 months; the remaining patients all died of disease, with the longest survival of 13 months (Table 1).
Approximately half (n = 10/21, 48%) were cytologically diagnosed as malignant (C5), with the remaining consisting of one suspicious (C4), one atypical (C3), seven negative (C2), and two nondiagnostic (C1) diagnoses. Two cases were misinterpreted as non–small cell carcinoma and suspicious for adenocarcinoma [3, 4]. Detailed cytologic descriptions were available in five articles. The lesional cells were discohesive or poorly cohesive, arranged in small clusters or single cells. Frequently reported cytomorphological features include marked nuclear irregularity and single to multiple prominent nucleoli. Vasoformative features were described in two articles, including hemophagocytosis, lumina, and vacuole formation. Another notable feature noted by Boucher et al. was the presence of a bloody background [3]. Positive immunocytochemical markers described were CD31, CD34, D2‐40, desmin, ERG, and factor VIII (Table 2).
Discussion
2
The incidence of sarcomas in leading to malignant effusion is significantly lower than carcinomas [20, 21]. Carcinomas with malignant effusions are often associated with dismal outcomes [22]. As for sarcomas, except for rare cases with radical treatment [23], involvement of serous cavities is unlikely to be compatible with long‐term survival [14, 15]. Compared to other sarcomas, angiosarcomas have a higher propensity for causing malignant effusions. Pericardial involvement in primary cardiac angiosarcomas is common, and the high risk of tumor bleeding and lung metastasis in angiosarcomas results in the classical presentation of bloody pleural effusion (hemothorax) [8, 21, 24]. As such, it is clinically relevant in recognizing such a presentation for making an accurate cytologic diagnosis.
As described in the current case series, angiosarcoma displays alarming cytomorphological features. Marked nuclear irregularity and single to multiple macronucleoli are consistent features noted by multiple authors [3, 7, 8, 13, 17]. In addition to the cytomorphologic features reported in the literature, mitotic and apoptotic figures were noted in Case 2 (Figure 3b), which can serve as a clue to the malignant behavior of the specimen. Vasoformation poses a diagnostic pitfall, as lumen formation and vacuolation can be mistaken for glandular formation, which resulted in misdiagnosis in two reported cases [3, 4]. Distinguishing features of angiosarcoma from adenocarcinoma are the lack of mucin production and a bloody background [3].
Additional literature on the cytomorphology of angiosarcomas on aspiration cytology, from excluded articles in the literature search and review of article references, was qualitatively reviewed. Two additional features were described in aspirates but not in effusion fluids, namely intracytoplasmic hemosiderin deposits and acinar‐like vascular structures [25, 26]. The lack of reports on such features in effusion cytology may be due to the small number of published cases that included cytomorphologic descriptions and that needle biopsy and aspiration may dislodge larger tissue fragments than passive tumor exfoliation [5].
Immunocytochemistry can be used to identify the singly malignant cells and to confirm vascular differentiation; useful markers include CD31, CD34, D2‐40, ERG, and factor VIII. At the same time, pertinent differentials should also be considered, and appropriate immunocytochemistry should be performed to exclude those diagnoses. The presence of prominent nucleoli and discohesiveness can suggest melanoma, while vacuolation can be seen in adenocarcinomas and macrophages. Supplementing vascular markers with macrophagic markers, melanoma markers, and cytokeratin [27] are good practices.
Specific clinical clues may be looked for when metastatic angiosarcoma is suspected. As in the current series, skin lesions and a history of radiotherapy were indicators of cutaneous angiosarcoma and radiation‐associated angiosarcoma, respectively. Primary cardiac sarcoma presents uniquely with heart failure symptoms, tamponade, and a cardiac mass. The progression of the primary lesion, metastatic deposits, and overall condition of the patient is rapid, and it is important to make a swift cytologic diagnosis to avoid treatment delay.
Conclusion
3
Angiosarcoma is distinctly associated with malignant effusion due to pericardial involvement in primary cardiac angiosarcoma and its bleeding tendency that often results in bloody effusion. Angiosarcoma can be recognized cytologically by its marked nuclear irregularity and single to multiple macronucleoli. However, features of vasoformation, lumen formation, and vacuolation overlap with adenocarcinomas and not uncommonly lead to misinterpretation. The lack of cohesiveness and a bloody background are hints differentiating these two overlapping entities. Clinical presentation and immunocytochemistry can contribute to achieving a correct diagnosis. The significance of recognizing this presentation lies in the quick disease tempo of metastatic angiosarcoma, and a quick cytologic diagnosis can ensure timely treatment.
Author Contributions
Jamie C. Y. Lam: data curation, investigation, visualization, writing – original draft. Iris Y. H. Liu: data curation, investigation, visualization, writing – original draft. Joanna K. M. Ng: investigation, resources, validation. Joshua J. X. Li: conceptualization, investigation, methodology, supervision, visualization, writing – review and editing.
Ethics Statement
The study was approved by the University of Hong Kong/Hospital Authority Hong Kong West institutional review board (reference number: 24–292).
Consent
The study was granted the exemption of requiring written informed consent by the University of Hong Kong/Hospital Authority Hong Kong West institutional review board.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1I. K. Poon , R. C. K. Chan , J. S. H. Choi , et al., “A Comparative Study of Diagnostic Accuracy in 3026 Pleural Biopsies and Matched Pleural Effusion Cytology With Clinical Correlation,” Cancer Medicine 12, no. 2 (2023): 1471–1481.35848750 10.1002/cam 4.5038 PMC 9883572 · doi ↗ · pubmed ↗
- 2J. J. X. Li , W. C. Chan , H. H. L. Chau , C. Wu , and G. M. Tse , “Cytologic Diagnosis of Metastatic Malignant Phyllodes Tumor of the Breast in Pleural Effusion,” Diagnostic Cytopathology 47, no. 6 (2019): 599–602.30829462 10.1002/dc.24151 · doi ↗ · pubmed ↗
- 3L. D. Boucher , P. E. Swanson , M. W. Stanley , J. F. Silverman , S. S. Raab , and K. R. Geisinger , “Cytology of Angiosarcoma. Findings in Fourteen Fine‐Needle Aspiration Biopsy Specimens and One Pleural Fluid Specimen,” American Journal of Clinical Pathology 114, no. 2 (2000): 210–219.10941336 10.1309/PXMU-LF 05-3894-W 29F · doi ↗ · pubmed ↗
- 4A. Sharma , J. J. Thangaiah , S. Shetty , and M. L. C. Policarpio‐Nicolas , “Bone and Soft Tissue Sarcomas in Cerebrospinal Fluid and Effusion: A 20‐Year Review at Our Institution,” Cancer Cytopathology 129, no. 10 (2021): 776–787.34233079 10.1002/cncy.22431 · doi ↗ · pubmed ↗
- 5J. K. M. Ng and J. J. X. Li , “Cytomorphologic Analysis of Pulmonary Neuroendocrine Tumors ‐ the Physical Effect of Abrasion and Aspiration on Cytomorphology,” Annals of Diagnostic Pathology 73 (2024): 152378.39342665 10.1016/j.anndiagpath.2024.152378 · doi ↗ · pubmed ↗
- 6N. M. Dörr‐Jerat , C. May , J. Knolle , S. Schmidt , and M. Krüger , “Case Report: Epithelioid Angiosarcoma of the Pleura,” Frontiers in Surgery 11 (2024): 1393159, 10.3389/fsurg.2024.1393159.38994239 PMC 11236686 · doi ↗ · pubmed ↗
- 7Y. Li , Y. M. Ahn , and S. Niu , “Primary Cardiac Angiosarcoma Initially Diagnosed on Pericardial Fluid Cytology With Histology and Autopsy Correlation,” Diagnostic Cytopathology 51, no. 9 (2023): E 263–E 266.37249363 10.1002/dc.25173 · doi ↗ · pubmed ↗
- 8H. Ogino , M. Tobiume , K. Kagawa , et al., “Radiation‐Associated Angiosarcoma Presenting as Massive Pleural Effusion,” Internal Medicine 61, no. 9 (2022): 1393–1397.34645765 10.2169/internalmedicine.8195-21PMC 9152858 · doi ↗ · pubmed ↗