Crimean-Congo hemorrhagic fever with severe bradycardia treated with Theophylline
Murat Aydın, Nurten Nur Aydın

TL;DR
A 30-year-old man with Crimean-Congo hemorrhagic fever developed severe bradycardia, which was successfully treated with theophylline.
Contribution
This case report demonstrates the successful use of theophylline to treat severe bradycardia in CCHF.
Findings
Severe bradycardia is a rare but serious complication of CCHF.
Theophylline treatment improved cardiac function in a CCHF patient with bradycardia.
Pharmacological intervention can be effective in managing cardiac complications of CCHF.
Abstract
Crimean-Congo hemorrhagic fever (CCHF) is a tick-borne viral hemorrhagic fever caused by Nairovirus and characterized by fever, myalgia, arthralgia, and hemorrhagic manifestations. Severe bradycardia is a rare complication of the disease. We present a 30-year-old male patient with CCHF who developed severe bradycardia, which was successfully treated with intravenous and oral theophylline. This case highlights the need to recognize cardiac complications in CCHF and highlights the role of pharmacological interventions in improving patient outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
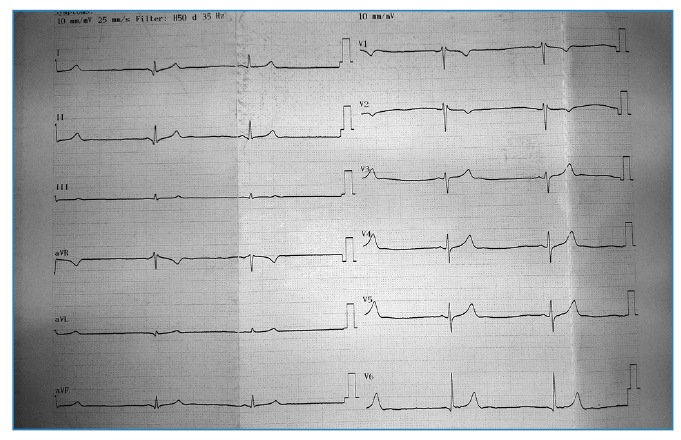 Figure 1
Figure 1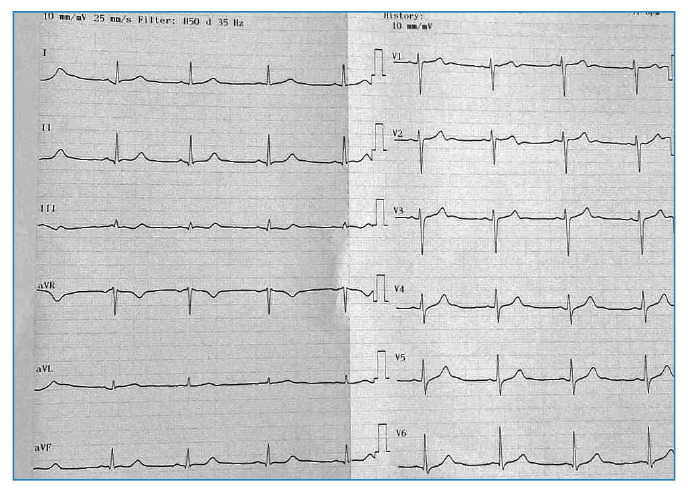 Figure 2
Figure 2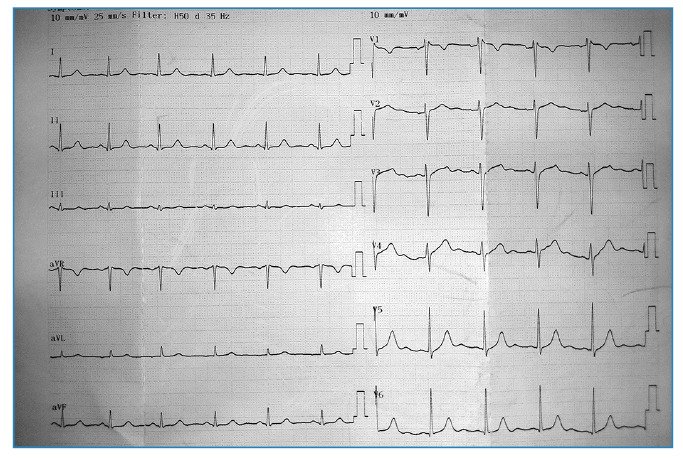 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Vectors · Mosquito-borne diseases and control · Fire effects on ecosystems
INTRODUCTION
Crimean-Congo hemorrhagic fever (CCHF) is an acute zoonotic viral infection caused by Nairovirus, primarily transmitted through tick bites or direct contact with infected animal tissues1. The disease is endemic in various regions, including the Middle East, Africa, and parts of Eastern Europe2. Typically, patients present with nonspecific symptoms such as fever, headache, and myalgia. However, the disease may progress to thrombocytopenia, disseminated intravascular coagulation (DIC), and hemorrhagic manifestations3. Cardiac complications in CCHF are uncommon, with bradycardia occurring in approximately 4% of cases4. Although severe bradycardia is often transient and self-limiting, it may necessitate specific pharmacological treatment5.
Despite the recognition of bradycardia as a complication of CCHF, a comprehensive search of major databases, including the Cochrane Library, LILACS, SciELO, MEDLINE, PubMed, and PMC (PubMed Central), revealed no studies specifically addressing the use of theophylline in treating bradycardia associated with CCHF. This report details the clinical progression and successful treatment of a patient with CCHF who developed severe bradycardia, thereby underscoring the therapeutic potential of theophylline in such scenarios.
CASE REPORT
A 30-year-old man was admitted to the emergency room after experiencing malaise, anorexia, fever, and diffuse muscle and joint pain for three days. Upon physical examination, he appeared lethargic yet hemodynamically stable. His vital signs included a heart rate of 88 beats per minute, blood pressure of 115/75 mmHg, and a body temperature of 38.5°C. Laboratory tests indicated leukopenia (2,750/mm³), thrombocytopenia (51,000/mm³), elevated liver enzymes (alanine aminotransferase, ALT: 177 U/L; aspartate aminotransferase, AST: 270 U/L), and elevated levels of creatine kinase (CK: 992 U/L) and lactate dehydrogenase (LDH: 720 U/L). A definitive diagnosis of CCHF was confirmed by polymerase chain reaction (PCR) testing of a blood sample.
The patient received symptomatic and supportive care, including intravenous fluids and antipyretics. Ribavirin was not administered. During the first three days of hospitalization, the patient's condition remained stable, with slight fluctuations in laboratory parameters.
On the fourth day, the patient reported increased fatigue and dizziness. A physical examination at this time revealed marked bradycardia with a heart rate of 35-40 beats per minute (Figure 1), although his blood pressure remained stable at 110/70 mmHg. Laboratory tests showed a further decrease in platelet count (29,000/mm³) and significantly elevated liver enzymes (ALT: 532 U/L; AST: 871 U/L) as well as persistently elevated LDH (1,092 U/L) and CK (825 U/L). Following a cardiology consultation, symptomatic bradycardia was confirmed, and intravenous theophylline (200 mg twice daily) was initiated. Over the next five days, the patient's heart rate gradually increased to 51 beats per minute (Figure 2), and he was transitioned to oral theophylline.
FIGURE 1:Electrocardiogram showing severe bradycardia on the fourth day of hospitalization.
FIGURE 2:Electrocardiogram after five days of treatment with theoph.
Subsequent laboratory tests showed normalization of platelet counts and white blood cells, reductions in ALT, AST, LDH, and CK levels, and increased heart rate to 67 beats per minute (Figure 3). The patient was discharged on the 12th day of hospitalization.
FIGURE 3:Electrocardiogram before discharge.
DISCUSSION
Cardiac complications are rarely observed in CCHF, with bradycardia occurring in approximately 4% of cases4. Although bradycardia is often transient and benign, it can present significant clinical challenges. The precise mechanism underlying bradycardia in CCHF remains elusive, but several hypotheses exist. One proposed mechanism is viral myocarditis, which involves direct myocardial infiltration by viruses, potentially affecting electrical conduction6. Another hypothesis suggests that cytokine production or direct myocardial damage could be responsible7.
In this instance, the bradycardia was severe and necessitated pharmacological intervention. Theophylline, a methylxanthine derivative, has been effectively used to manage bradycardia. Its efficacy in this context has been corroborated by previous studies8 ^,^ 9. For this patient, intravenous theophylline led to rapid symptomatic improvement, and subsequent oral therapy facilitated further stabilization, allowing for an uneventful discharge.
Notably, Ribavirin, commonly employed as an antiviral agent in CCHF, has also been associated with bradycardia10. However, Ribavirin was not administered in this case, eliminating its potential contribution to the observed bradycardia.
Comparative studies of other viral hemorrhagic fevers, such as dengue fever, have also identified bradycardia as a potential complication11. However, the literature on this complication in CCHF is limited, predominantly describing cases that are self-limited. The severity of bradycardia observed in this patient underscores the necessity for close cardiac monitoring in individuals with CCHF, especially those exhibiting significant systemic inflammation or multisystem involvement. While severe bradycardia in CCHF is typically transient and self-resolving, pharmacological intervention may be required in certain cases to prevent adverse outcomes.
This case highlights the importance of early detection and targeted pharmacological management. The successful use of theophylline in this patient demonstrates its potential as a valuable treatment option for severe bradycardia in infectious diseases. Further research is needed to better understand the pathophysiology and to optimize the treatment of cardiac complications in CCHF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nasirian H New aspects about Crimean-Congo hemorrhagic fever (CCHF) cases and associated fatality trends: A global systematic review and meta-analysis Comp Immunol Microbiol Infect Dis 2020691014291014293206219010.1016/j.cimid.2020.101429 · doi ↗ · pubmed ↗
- 2Frank MG Weaver G Raabe V Crimean-Congo Hemorrhagic Fever Virus for Clinicians-Epidemiology, Clinical Manifestations, and Prevention Emerg Infect Dis 20243058548633866654810.3201/eid 3005.231647 PMC 11060446 · doi ↗ · pubmed ↗
- 3Ergonul O Crimean-Congo haemorrhagic fever Lancet Infect Dis 2006642032141655424510.1016/S 1473-3099(06)70435-2PMC 7185836 · doi ↗ · pubmed ↗
- 4Erol S Özkurt Z Özden K Parlak M Erol MK Transient bradycardia in patients with Crimean-Congo hemorrhagic fever Turk J Med Sci 2012425753756
- 5Sidhu S Marine JE Evaluating and managing bradycardia Trends Cardiovasc Med 20203052652723131169810.1016/j.tcm.2019.07.001 · doi ↗ · pubmed ↗
- 6Taghdiri A Inflammation and arrhythmogenesis: a narrative review of the complex relationship Int J Arrhythm 2024254212
- 7Aksakal E İba Yılmaz S Alay H Turan OE Öztürk M Ceyhun G Electrocardiographic Evaluation of Patients with Crimean-Congo Hemorrhagic Fever New Trends in Medicine Sciences 202343102107
- 8Perrine JA Barber J Mc Knight RL Rowe AS Theophylline for Spinal Cord Injury Associated Bradycardia J Pharm Pract 20233635795833505081510.1177/08971900211064701 · doi ↗ · pubmed ↗