Late Periprosthetic Joint Infection After a Total Hip Arthroplasty Caused by Peptoniphilus Species: A Case Report and Literature Review
Daisuke Inoue, Tamon Kabata, Yu Yanagi, Musashi Ima, Satoru Demura

TL;DR
A 65-year-old woman had a late hip infection caused by Peptoniphilus species, treated with two-stage surgery and specific antibiotics.
Contribution
Highlights Peptoniphilus species as a causative agent in late joint infections and recommends treatment strategies.
Findings
Peptoniphilus species can cause late periprosthetic joint infections.
Two-stage revision surgery is effective for treating such infections.
Clindamycin and cephalosporins are recommended for postoperative antibiotic therapy.
Abstract
In this report, we present the clinical course of a 65-year-old woman who underwent a two-stage revision total hip arthroplasty (THA) for a late periprosthetic joint infection (PJI) caused by Peptoniphilus species (Peptoniphilus sp.). Furthermore, we conducted a literature review to contribute to the growing body of evidence regarding PJI caused by Peptoniphilus sp. Recognizing Peptoniphilus sp. as a potential causative pathogen in late PJI is important. Treatment should involve a two-stage revision surgery, with clindamycin (CLDM) and cephalosporins recommended for postoperative antibiotic therapy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
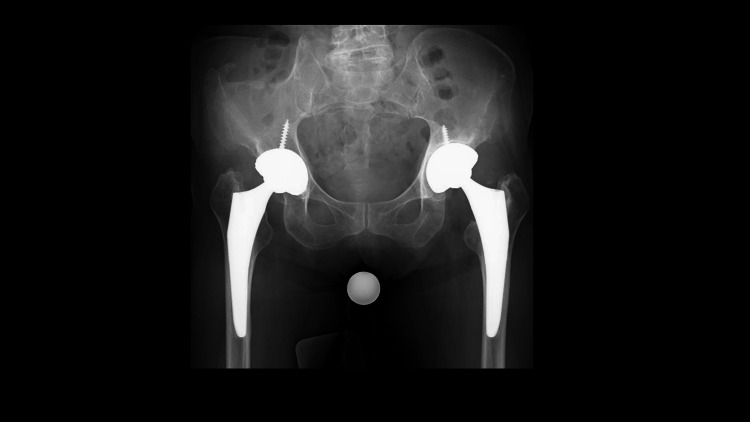 Figure 1
Figure 1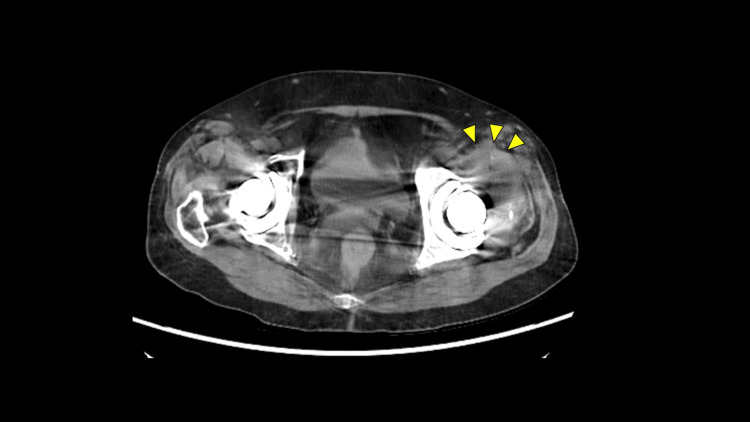 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5| Lab test | Results |
| WBC (/μl) (normal: 3300-8600) | 6450 |
| Neutrophil (%) (normal: 40.7-77.0) | 66.4 |
| Hb (g/dl) (normal: 11.6-14.8) | 11.6 |
| Plt (×10³) (normal: 158-348) | 373 |
| CRP (mg/dl) (normal: <0.3) | 0.4 |
| ESR (1 hr) (normal: < 20) | 54 |
| Name of the study | Years | Treatment | Antibiotics | Others |
| Enault C et al. [ | 2020 | One stage (Failed) | After one stage revision IV: OFLX After DAIR IV: VCM+CTM Po: CLDM+RFP | One-stage revision failed. Additional operation (DAIR) was done. |
| Sarantis M et al. [ | 2022 | Two-stage | IV: DAP+CTRX; Po: CLDM | Cement spacer: tobramycin + vancomycin |
| Current study | 2025 | Two-stage | IV: CLDM+CEZ; Po: CLDM+CEX | Cement spacer: amikacin + vancomycin |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Orthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes
Introduction
Total hip arthroplasty (THA) is an effective orthopedic surgical procedure for patients with symptomatic, advanced hip osteoarthritis. However, with the increasing number of primary THA procedures due to longer life expectancy and improved implant quality, perioperative complications following primary THA have also increased [1]. Among these complications, periprosthetic joint infections (PJIs) are particularly challenging, as they often require multiple surgical interventions to eradicate the infection, resulting in poor clinical outcomes [2]. The incidence of acute PJIs following primary THA is approximately 0.5%, while the rate of late PJIs is lower than that of acute surgical site infection (SSI) or PJI [3]. Anaerobic microorganisms account for 3%-6% of all PJIs, with most cases caused by Gram-positive cocci or Gram-negative bacilli, such as Staphylococcus aureus and Escherichia coli [4]. To the best of our knowledge, *Peptoniphilus *species (*Peptoniphilus *sp.) are extremely rare as the organism profile of PJI, meanwhile, they sometimes act as part of polymicrobial infections and are commonly found in chronic wounds and diabetic ulcers. [5].
Herein, we report the clinical course of a 65-year-old woman who underwent a two-stage revision THA for late PJI caused by Peptoniphilus sp. Additionally, we conducted a literature review to contribute to the growing body of evidence regarding late PJI caused by Peptoniphilus sp., as, to the best of our knowledge, this condition has been reported in only two previous studies [6,7].
Case presentation
The patient was diagnosed with athetoid cerebral palsy. At the age of 47 years, she occasionally experienced bilateral coxalgia, although the pain did not limit her activities of daily living. By 62 years of age, the bilateral coxalgia had worsened, and the patient was referred to our hospital. Hip radiographs revealed end-stage osteoarthritis in the right hip joint and advanced osteoarthritis in the left hip joint, both due to acetabular dysplasia. A primary cementless THA of the right hip was performed via the anterolateral approach using a computed tomography (CT)-based navigation system. One month later, the left hip underwent primary cementless THA. For the acetabular component, a Trident PSL acetabular cup (Stryker, Mahwah, NJ, USA) was implanted, while an Accolade II (Stryker, Mahwah, NJ, USA) was inserted into the femoral canal. At six months postoperatively, the patient was pain-free in both hips and able to walk steadily without using a T-cane.
At one year postoperatively, a hip radiograph revealed a radiolucent line (RLL) around the proximal shoulder of the left femoral stem, despite the absence of bilateral hip pain. However, the patient developed left-sided hip pain upon weight-bearing as the RLL around the proximal shoulder of the left femoral stem and acetabular cup slightly expanded (Figure 1).
Preoperative hip radiograph A radiolucent line appears in the left acetabular implant and the shoulder of the femoral implant.
A hip CT revealed a fluid collection in the left hip joint. The fluid was aspirated and tested (Figure 2).
Preoperative computed tomography (CT) scan of the hipFluid collection is observed in the left hip joint.
No organisms were isolated, although the leukocyte elastase test result was 3+. Routine blood test results showed a slight elevation in the values of inflammatory markers, including an erythrocyte sedimentation rate (ESR) of 54 mm/h (normal: <20 mm/h) and a C-reactive protein (CRP) level of 0.4 mg/dL (normal: <0.3 mg/dL) (Table 1).
According to the 2018 International Consensus Meeting criteria, this case was inconclusive for late PJI but was suspicious of low-grade late PJI [8]. Therefore, the diagnosis was confirmed intraoperatively using an alpha-defensin test and frozen section analysis.
Operative procedure and postoperative clinical course
The posterolateral approach was used with the patient in the lateral decubitus position. Fluid collection was aspirated, and the alpha-defensin test result was positive. Inflammatory synovial tissue from the hip joint and proximal femur around the femoral stem was collected to identify the causative organism. Frozen sections revealed multiple multinucleated neutrophilic infiltrates (10>400 high-power fields (HPF)). After intraoperative tissue samples and joint fluid were obtained, the acetabular cup was removed using an explant device (Zimmer, Inc., Warsaw, IN, USA), and the femoral implant was extracted using the Steinman pin technique [9]. Inflammatory and necrotic tissue was resected. Subsequently, the hip joint and femoral canal were irrigated using diluted 0.2% povidone-iodine. Finally, an antibiotic-loaded bone cement spacer containing vancomycin (6 g) and amikacin (1.2 g) was inserted into the acetabular side and femoral canal (Figure 3).
Hip radiograph from the first surgery All implants in the left hip joint were removed, and an antibiotic-loaded cement spacer was inserted into the acetabular and femoral canal.
Postoperatively, *Peptoniphilus *sp. were isolated from intraoperative tissue samples and joint fluid using enrichment culture microbiological techniques [10]. Based on microbiological sensitivity results, a two-week course of antibiotic-specific therapy with intravenous clindamycin (CLDM) and cefazolin (CEZ) was initiated immediately, followed by a switch to oral CLDM and cefalexin (CEX) for four weeks. At six weeks postoperatively, laboratory results showed minimal inflammatory changes, with an ESR of 25 mm/h and a CRP level of 0.1 mg/dL. Oral antibiotic suppression therapy was continued until final reimplantation at eight weeks postoperatively.
In the final operation, a posterolateral approach was used with the patient in the lateral decubitus position. Intraoperatively, the soft tissues appeared in good condition, and bone stock was adequate. Tissue samples from the hip joint and femoral canal were collected for cultures and histological analysis. Frozen sections showed no evidence of multiple multinucleated neutrophilic infiltration (5≦400 HPF). Based on these findings, final reimplantation was performed. The acetabular cup (G7 Osseo-Ti multihole 58 mm, Zimmer, Inc.) was press-fitted into the acetabulum using CT-based hip navigation, followed by insertion of a Zweymüller-type long femoral stem (Alloclassic SLL, Zimmer, Inc.) into the femoral canal (Figure 4).
Hip radiograph from the two-stage revision surgery
Postoperatively, the patient was allowed full weight-bearing ambulation and received intravenous CLDM and CEZ for two weeks, followed by a switch to oral CLDM and CEX. Chronic suppression therapy was continued for six months postoperatively. At the final follow-up, one year after the final implantation, laboratory results showed no signs of inflammation, with an ESR of 12 mm/h and a CRP level of 0.1 mg/dL. Radiographs showed no RLL around the acetabular and femoral implant (Figure 5).
Hip radiograph obtained during the last follow-up (one year after the two-stage revision surgery)
Finally, the patient was able to walk independently without pain or other relevant symptoms in the affected hip.
Discussion
Late PJI after THA caused by Peptopniphilus sp. is considered rare, as this organism is a causative agent in polymicrobial infections associated with other infectious diseases [11]. In particular, a previous study reported that *Peptopniphilus *sp. is the most prevalent organism in the colonization of chronic wounds. In fact, only two previous studies have reported cases of late PJI after primary THA caused by *Peptopniphilus *sp. (Table 2).
Enault et al. reported a case of late PJI in a 66-year-old female patient, which included extensive osteolysis. They initially attempted a one-stage revision for late PJI; however, additional treatment, including debridement, antibiotics, irrigation, and retention, was required due to the failure to eradicate the infection [6]. Meanwhile, Sarantis et al. reported a case of late PJI in a 68-year-old female patient following primary THA. They treated the infection with a two-stage revision, which successfully eradicated the late PJI [7]. Including our report, revision surgery for this low-grade infection caused by *Peptopniphilus *sp. is considered safe using a two-stage approach.
Culture isolation is crucial for the treatment of PJI, as appropriate antimicrobial therapy cannot be administered without identifying the causative organism. Importantly, previous reports and the present case report indicate that the identification of this organism in late PJI after THA has been achieved using enrichment culture techniques, implant sonication, and the 16S rRNA gene sequencing method, rather than standard culture methods. Therefore, it is necessary to recognize in advance that this organism can be a causative agent of late PJI, including implant loosening, and to perform alternative isolation methods other than standard culture methods. Regarding antibiotic therapy, the use of CLDM may lead to favorable clinical outcomes based on previous studies and this case report, although penicillin and cephalosporin are included in the antibacterial spectrum covering *Peptopniphilus *sp. In cases of late PJI, where biofilm formation occurs around bone, soft tissue, or implants, CLDM may be a reasonable choice, as previous studies have demonstrated its effective intracellular translocation [12]. Therefore, regardless of intravenous or oral administration, CLDM may be a valuable option based on the results of microbiological sensitivity tests.
One of the limitations could be that this is a case report and a literature review. Hence, these findings cannot be generalized because of the rare condition. As a scope for future research, a longer follow-up of the treatment for late PJI is required to generalize the way to use antibiotics in terms of the recurrence of PJI. Case series with longer follow-up will be needed in order to validate and generalize these findings.
Conclusions
We report the clinical course of a patient who underwent a two-stage revision THA for late PJI caused by *Peptoniphilus *sp., along with a review of the literature. Importantly, previous reports and the present case indicate that identification of this organism in late PJI after THA can be achieved using enrichment culture techniques, implant sonication, and the 16S rRNA gene sequencing method, rather than standard culture methods. Therefore, recognizing Peptoniphilus sp. as a potential causative organism in late PJI is crucial. According to previous papers and our findings, a two-stage revision approach is considered safe and effective for this low-grade infection caused by *Peptopniphilus *sp. We recommend that CLDM be used with cephalosporins for postoperative antibiotic therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030 J Arthroplasty Schwartz AM Farley KX Guild GN Bradbury TL Jr 08535202010.1016/j.arth.2020.02.030PMC 723974532151524 · doi ↗ · pubmed ↗
- 2Health state utility in patients with osteoarthritis of the hip and total hip arthroplasty J Arthroplasty Bozic KJ Chiu VW Slover JD Immerman I Kahn JG 12922620112160202310.1016/j.arth.2011.03.033 · doi ↗ · pubmed ↗
- 3The incidence of deep prosthetic infections in a specialist orthopaedic hospital: a 15-year prospective survey J Bone Joint Surg Br Phillips JE Crane TP Noy M Elliott TS Grimer RJ 9439488820061679900110.1302/0301-620X.88B 7.17150 · doi ↗ · pubmed ↗
- 4Prosthetic joint infection Clin Microbiol Rev Tande AJ Patel R 3023452720142469643710.1128/CMR.00111-13PMC 3993098 · doi ↗ · pubmed ↗
- 5Polymicrobial nature of chronic diabetic foot ulcer biofilm infections determined using bacterial tag encoded FLX amplicon pyrosequencing (b TEFAP)P Lo S One Dowd SE Wolcott RD Sun Y Mc Keehan T Smith E Rhoads D 03200810.1371/journal.pone.0003326 PMC 255609918833331 · doi ↗ · pubmed ↗
- 6Surgical site infection after hip replacement due to a novel Peptoniphilus species, provisionally named 'Peptoniphilus nemausus' sp. nov Anaerobe Enault C Aujoulat F Pantel A 1020716120203130675410.1016/j.anaerobe.2019.102071 · doi ↗ · pubmed ↗
- 7Sonication fluid isolation of Peptoniphilus asaccharolyticus after total hip arthroplasty Cureus Sarantis M Argyrou C Tzefronis D Stasi S Macheras G 014202210.7759/cureus.21419 PMC 885590035198324 · doi ↗ · pubmed ↗
- 8Hip and knee section, outcomes: proceedings of International Consensus on Orthopedic Infections J Arthroplasty Abblitt WP Ascione T Bini S 09534201910.1016/j.arth.2018.09.03530348557 · doi ↗ · pubmed ↗