Impact of Vitamin E‐Coated Membrane Hemodiafilter on Serum Albumin Redox State in the Acute Kidney Injury Pig Hemodialysis Model
Shouichi Fujimoto, Masahide Koremoto, Shushi Yamamoto, Hiroshi Umeno, Yusuke Sano, Toshihiro Tsuruda

TL;DR
This study shows that a vitamin E-coated hemodiafilter helps preserve serum albumin and its reduced form in pigs with acute kidney injury during hemodiafiltration.
Contribution
The novel finding is that vitamin E-coated hemodiafilters minimize the reduction of serum albumin and its reduced form in an acute kidney injury model.
Findings
Serum albumin levels decreased less in the vitamin E-coated group compared to the non-coated group.
Reduced albumin (RedALB) levels were significantly higher in the vitamin E-coated group.
A significant positive correlation was found between serum albumin and RedALB levels.
Abstract
Several studies have evaluated the biocompatibility of dialysis membranes. The use of vitamin E‐coated membranes has been reported multilaterally in in vitro and clinical studies. Nevertheless, the effect of vitamin E‐coated membranes on the redox state of serum albumin, which forms the largest fraction of reactive sulfhydryl groups, has not been reported. Hemodiafiltration (HDF) with and without a vitamin E‐coated hemodiafilter (V‐RATM group and ABHTM groups, respectively) was performed in an acute kidney injury pig model to determine whether changes in the serum albumin, the oxidized albumin (OxiALB), and the reduced albumin (RedALB) levels differ between the two groups. Analyses were conducted 22–24 times in the V‐RATM group and 16–18 times in the ABHTM group, excluding missing data. The serum albumin levels decreased in both groups after nephrectomy; however, the decrease observed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
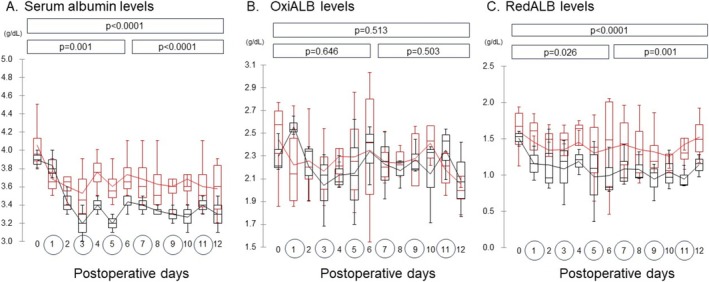 FIGURE 1
FIGURE 1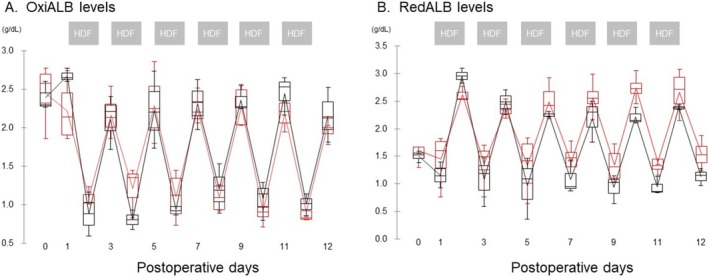 FIGURE 2
FIGURE 2| V‐RA | ABH |
| |
|---|---|---|---|
| [Pre HDF at POD1] | 1.60 ± 0.31 | 1.51 ± 0.11 | 0.857 |
| [Averaged over HDF treatments] | |||
| Pre HDF | 1.38 ± 0.36 | 1.04 ± 0.31 |
|
| 2 Hr IN | 1.91 ± 0.34 | 1.68 ± 0.25 |
|
| 2Hr OUT | 2.50 ± 0.32 | 2.25 ± 0.22 |
|
| 2Hr changes (IN → OUT) | 0.56 ± 0.31 | 0.55 ± 0.34 | 0.779 |
| 4Hr IN | 2.08 ± 0.36 | 1.80 ± 0.25 |
|
| 4Hr OUT | 2.58 ± 0.29 | 2.38 ± 0.31 |
|
| 4Hr changes (IN → OUT) | 0.46 ± 0.27 | 0.54 ± 0.26 | 0.506 |
| 4Hr OUT → next Pre HDF | −1.12 ± 0.34 | −1.29 ± 0.26 | 0.196 |
- —Asahi Kasei Medical Co. LTD
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Acute Kidney Injury Research · Muscle and Compartmental Disorders
Introduction
1
Several in vitro studies have investigated the biocompatibility of dialysis membranes [1, 2, 3]. Vitamin E‐coated dialyzer membranes are superior to conventional dialyzer membranes in terms of controlling the progression of renal anemia and inhibiting blood coagulation during maintenance hemodialysis therapy [4, 5, 6]. However, few studies have examined the usefulness of vitamin E‐coated dialyzers on reduced albumin in the context of dialysis therapy for acute kidney injury. Patients undergoing dialysis develop oxidative stress, which generates increased levels of protein oxidation products and misfolded proteins, leading to a poor prognosis. The regulation of albumin redox is central to the mechanisms of protein homeostasis (proteostasis) and immune dysfunction (immunoproteostasis) [7, 8].
A previous study evaluating the efficacy of dialysis membranes in an in vivo pig hemodialysis model [9] revealed that pigs that underwent hemodialysis/hemodiafiltration using vitamin E‐coated membranes had lower advanced oxidation protein product levels early after commencing dialysis than those with vitamin E‐non‐coated membranes. Furthermore, reduced fibrinogen adhesion capacity to the dialysis membrane was observed in these pigs on postoperative day 1 (POD 1). Determining the redox state of serum albumin, an oxidative stress marker that forms the largest fraction of reactive sulfhydryl (free thiol groups) and acts as an effective antioxidant system in plasma [10], is difficult but essential. The level of the human non‐mercaptoalbumin (HNA) fraction (oxidative forms) in serum albumin is correlated with the risk of death from cardiovascular diseases in normoalbuminemic patients undergoing hemodialysis [11]. However, no previous studies have evaluated the serum albumin redox state in patients with acute kidney injury during hemodialysis therapy.
Therefore, this study aimed to investigate whether the serum albumin redox state, as a primary endpoint during hemodiafiltration (HDF) treatment for acute kidney injury, differs between two types of membranes (a vitamin E‐non‐coated or vitamin E‐coated membrane) using samples from a recently reported study [9].
Methods
2
Animals and Post On‐Line HDF With Pig Model
2.1
All animal experiments conducted in this study were approved by the Animal Experiment Committee at Miyazaki University (approval numbers: 2018‐017 and 2019‐035) and Asahi Kasei Medical (approval numbers: Ohito 18‐002 and Ohito 19‐010). Two groups were created based on the type of hemodiafilter (with the same membrane area and materials) used to perform HDF: the ABH^TM^ and V‐RA^TM^ groups, which used the vitamin E‐non‐coated hemodiafilter ABH^TM^‐15PA and the vitamin E‐coated hemodiafilter V‐15RA, respectively (Asahi Kasei Medical Co. Ltd., Tokyo, Japan).
Treatment Conditions for HDF
2.2
For HDF treatment, four pigs were assigned to the V‐RA^TM^ group, while three pigs were assigned to the ABH^TM^ group. The experiment was performed using a post‐dilution online HDF setting with the following parameters: Qb (blood flow rate) = 200 mL/min, Qd (dialysate flow rate) = 500 mL/min, and Qf (filtrate flow rate) = 50 mL/min as an additional substitute; the treatment time was 240 min per session, and six treatments were performed every other day for 2 weeks [9].
Preparation of OxiALB/RedALB as a Standard Reagent and Measurement of OxiALB/RedALB Levels
2.3
Supplemental Methods present the detailed methods used for the liquid chromatography‐mass spectrometry (LC/MS) analyses of OxiALB and RedALB [12, 13, 14]. Based on a pre‐examined analysis using porcine albumin as a standard reagent, the molecular weights of OxiALB and RedALB were measured and detected using approximately 66 862 and 66 743 binding cysteine types, respectively (Supplement Figure and Method S1, S2).
Statistical Analysis
2.4
All statistical analyses were performed using the XLSTAT ver.2018 software (Addinsoft, Paris, France). An analysis of the covariance model was performed using the day of HDF as the covariate and the measurement data as the dependent variable to evaluate the comparability of the two types of membranes for HDF (ABH^TM^ vs. V‐RA^TM^). Additionally, the Mann–Whitney U test was used to compare data acquired at the same point in both hemodiafilters. The level of statistical significance was set at 5% for all analyses (p < 0.05). All values are presented as the mean ± standard deviation.
Results
3
HDF treatment was performed for the V‐RA^TM^ group (total 24 sessions; four pigs, six sessions each) and the ABH^TM^ group (total 18 sessions; three pigs, six sessions each). Data analysis was conducted using 22–24 values for the V‐RA group and 16–18 values for the ABH group, excluding missing data.
Figure 1 presents changes in albumin levels across PODs 1–12. Serum albumin concentration during HDF was persistently higher in the V‐RA^TM^ group than in the ABH^TM^ group, except on POD 1 (Figure 1A). No significant differences in OxiALB levels were observed between the two groups (Figure 1B). However, the RedALB levels were lower in the ABH^TM^ group (Figure 1C). A positive correlation was observed between serum albumin and RedALB levels (Pearson's correlation coefficient 0.528, p‐value < 0.0001).
The changes in the total albumin, OxiALB, and RedALB levels, including the changes with and without hemodiafiltration, from postoperative day (POD) 0 to 12. (A) ALB: Serum total albumin. (B) OxiALB:Oxidized albumin. (C) RedALB: Serum reduced albumin. The red and black lines represent the changes in V‐RATM and ABHTM groups, respectively. The line in the graph shows the average. The p‐values in the box were obtained for the analysis of the covariance model between two types of hemodiafilters from POD 0 to 6, POD 6 to 12, and POD 0 to 12. The numbers in the circles represent the day of the HDF procedure. [Color figure can be viewed at wileyonlinelibrary.com]
OxiALB levels decreased significantly over time during HDF (Figure 2A); however, no significant difference was observed between the two groups. In contrast, RedALB levels at the start of each HDF increased significantly compared to those at the end of each HDF in both groups (Figure 2B); however, the levels at the end of HDF in the V‐RA^TM^ group (n = 4) were higher than those in the ABH^TM^ group (n = 3) during the fourth and fifth HDF treatments (p = 0.057).
Changes in the pre‐ and post‐values of OxiALB and RedALB levels during hemodiafiltration from postoperative day (POD) 0 to 12. The red and black lines represent the changes in V‐RATM and ABHTM groups, respectively. The line in the graph shows the average. [Color figure can be viewed at wileyonlinelibrary.com]
Table 1 shows RedALB levels before the first HDF treatment on POD1 and the changes in RedALB levels in the V‐RA^TM^ and ABH^TM^ groups during HDF using hemodiafilters. Albumin levels before the 1st HDF treatment on POD1 did not differ between the two groups. RedALB levels increased after the start of HDF treatment compared to those before HDF treatment in both groups. However, the RedALB levels in the V‐RA^TM^ group, including those at the inlet and outlet at 2 and 4 h, were significantly higher than those in the ABH group. In contrast, the degree of increase in RedALB levels before and after hemodiafiltration (inlet and outlet) at 2 and 4 h after the start of HDF treatment did not differ between the two groups. RedALB levels that were elevated at the end of HDF were lower at the start of the next HDF; the extent of the decline did not differ between the two groups (Figure 2B, Table 1).
Discussion
4
The lower the albumin levels, the higher the risks of acute kidney injury and subsequent mortality. Notably, both albumin and its redox state levels could be crucial in the progression of kidney disease [15, 16, 17]. There is a decrease in RedALB levels, with a corresponding increase in the ratio of the oxidized form (percent of OxiALB/(OxiALB and RedALB)) in critically ill patients and post‐surgery patients [7, 8, 18, 19]. For hemodialysis patients, the human mercaptalbumin fraction (RedALB) of human albumin increased 3–5 h after starting hemodialysis and then decreased to subnormal levels [20, 21] which is consistent with the present results.
Until recently, no studies have examined redox status in acute kidney injury using a 2‐week‐long dialysis model. The current study used an in vivo pig acute kidney injury model in the V‐RA^TM^ group (vitamin E‐coated membranes) and demonstrated a lesser decline in serum albumin and RedALB levels during HDF compared to the ABH^TM^ group, although the authors hypothesized that the levels of OxiALB would decrease and that of RedALB would increase in vitamin E‐coated membranes before beginning the present research (Figure 1A,C).
Serum albumin levels are known to decrease after surgery and during systemic inflammation. The causes are thought to be hepatic reprioritization of protein synthesis (the suppression of albumin synthesis and increased synthesis acute phase protein) [11, 22], redistribution of serum proteins (an increase in capillary permeability), and an increase in protein catabolism. The decreases in the serum albumin levels immediately after bilateral nephrectomy observed in the present study may be attributed to these causes, as hepatic dysfunction was not observed in either group (Figure 1A, Table 1).
Why was the subsequent decline in serum albumin levels less in group V‐RA^TM^ than in group ABH^TM^ ? The advantage of coating dialysis membranes with vitamin E is that this molecule increases at the same time the biocompatibility of the biomaterials and the antioxidant protection of blood components [23]. RCTs on these membranes have demonstrated promising results with benefits to oxidative stress, inflammation, vascular damage, and clinical management of anemia. Meta‐analyses [24, 25], while showing the positive effect of using a vitamin E‐coated membrane on the reduction of oxidative stress biomarkers, demonstrated an improvement in the inflammatory status. Considering the above, the lower decline in serum albumin levels in group V‐RA^TM^ may be related to the increase in reduced albumin with the vitamin E‐coated membrane, resulting in the suppression of inflammation and increased synthesis of albumin.
Patients who undergo HD show higher oxidized albumin and lesser reduced albumin levels compared to healthy controls; however, the oxidized albumin fraction decreases while the reduced albumin fraction increases after HD treatment [16, 20, 26, 27]. Furthermore, these effects were significantly more pronounced in patients treated with high‐flux than low‐flux dialyzers [28, 29, 30]. In dialysis‐dependent acute renal failure, the levels of antioxidant vitamins such as α‐tocopherol were reduced and directly correlated with albumin and total antioxidant capacity of serum (ex. oxygen radical absorbance capacity: ORAC). The reduction in the ORAC was more pronounced during dialysis with cellulose acetate than with polysulfone membranes [31]. In contrast, irreversibly oxidized HNA‐2 levels show no variation during hemodialysis [20, 28] and increase over the course of plasmapheresis treatments of commercial human albumin and remain elevated 12 days after the last plasmapheresis procedure [32]. The V‐RA^TM^ and ABH^TM^ groups differed from each other in terms of the hemodiafilters used in the present study; however, the properties and area of the membranes and dialysis method were identical in both groups [9]. Additionally, previous reports comparing vitamin E‐non‐coated hemodiafilter ‘ABH^TM^’ with vitamin E‐coated hemodiafilter ‘V‐RA^TM^’ in human clinical studies reported that the effect of albumin leakage from both hemodiafilters during post‐dilution HDF is not significantly different [33]. Considering this, it is possible that in the present study, the decrease in oxidized albumin with the vitamin E‐coated polysulfone membrane was not dependent on the removal performance but was more likely due to its effects on proteostasis and immunometabolic complications.
RedALB levels increased and OxiALB levels decreased after HDF compared to before HDF treatment, respectively, and both returned to baseline levels at the next HDF treatment, suggesting that dialyzable uremic solutes may contribute to inducing intermolecular sulfhydryl‐disulfide exchange reactions. However, in the present study, there was no significant difference between the two groups in the extent of the increase in RedALB levels after HDF. Taking the above into account, the vitamin E‐coated membrane may have suppressed postoperative reduction in the synthesis ability of RedALB.
The potential limitations of this study are as follows: The authors did not compare the effects of oral Vitamin E administration with those of the dialysis membrane. Furthermore, the authors did not conduct a sufficient analysis of mortality, organ failure, and inflammatory and innate immunity. Future studies should explore these aspects to elucidate the comparative effects of the two membrane types.
In conclusion, the present study revealed that HDF using a vitamin E‐coated hemodiafilter rescued the reduction of serum albumin and increased RedALB levels in a pig model of acute kidney injury. Thus, vitamin E‐coated hemodiafilters may be useful in the HDF in postoperative acute renal failure owing to their excellent biocompatibility. Nonetheless, further studies should clarify the usefulness of vitamin E‐coated dialyzer membranes in clinical practice and investigate the mechanisms underlying changes in the serum albumin redox state.
Author Contributions
S.F., S.Y., and H.U. contributed to the first original study design and interpretation of results (Yamamoto et al. [9]). S.F. and M.K. contributed to writing the manuscript. H.U. and Y.S. contributed to measuring the blood samples. M.K. contributed to the statistical design and statistical analysis. T.T. revised the manuscript. All authors have read and approved the final version of the manuscript.
Conflicts of Interest
Masahide Koremoto, Hiroshi Umeno, and Yusuke Sano are employees of Asahi Kasei Medical Corporation.
Supporting information
Data S1.
Data S2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Kawanishi , M. Koremoto , and C. F. M. Franssen , “Clotting Propensity of Surface‐Treated Membranes in a Hemodialysis Set‐Up That Avoids Systemic Anticoagulation,” Seminars in Nephrology 43 (2023): 151482.38262850 10.1016/j.semnephrol.2023.151482 · doi ↗ · pubmed ↗
- 2R. Takatsuji , M. Koremoto , Y. Fujimoto , Y. Saida , and Y. Hatanaka , “Flexible Inner Surface of Polysulfone Membranes Prevents Platelet Adhesive Protein Adsorption and Improves Antithrombogenicity In Vitro,” International Journal of Artificial Organs 47 (2024): 774–782.39229822 10.1177/03913988241269465 PMC 11823271 · doi ↗ · pubmed ↗
- 3H. Tsukao , K. Kokubo , H. Takahashi , et al., “Activation of Platelets Upon Contact With a Vitamin E‐Coated/Non‐Coated Surface,” Journal of Artificial Organs 16 (2013): 193–205.23381644 10.1007/s 10047-013-0686-4 · doi ↗ · pubmed ↗
- 4V. Panichi , A. Rosati , S. Paoletti , et al., “A Vitamin E‐Coated Polysulfone Membrane Reduces Serum Levels of Inflammatory Markers and Resistance to Erythropoietin‐Stimulating Agents in Hemodialysis Patients: Results of a Randomized Cross‐Over Multicenter Trial,” Blood Purification 32 (2011): 7–14.21242686 10.1159/000321369 · doi ↗ · pubmed ↗
- 5T. Sanaka , T. Mochizuki , E. Kinugasa , et al., “Randomized Controlled Open‐Label Trial of Vitamin E‐Bonded Polysulfone Dialyzer and Erythropoiesis‐Stimulating Agent Response,” Clinical Journal of the American Society of Nephrology 8 (2013): 969–978.23599410 10.2215/CJN.04680512 PMC 3675844 · doi ↗ · pubmed ↗
- 6M. S. Islam , Z. A. Hassan , F. Chalmin , et al., “Vitamin E‐Coated and Heparin‐Coated Dialyzer Membranes for Heparin‐Free Hemodialysis: A Multicenter, Randomized, Crossover Trial,” American Journal of Kidney Diseases 68 (2016): 752–762.27344212 10.1053/j.ajkd.2016.05.013 · doi ↗ · pubmed ↗
- 7F. Galli , D. Bartolini , and C. Ronco , “Oxidative Stress, Defective Proteostasis and Immunometabolic Complications in Critically Ill Patients,” European Journal of Clinical Investigation 54, no. 9 (2024): 14229, 10.1111/eci.14229.38676423 · doi ↗ · pubmed ↗
- 8F. Galli , “Protein Damage and Inflammation in Uraemia and Dialysis Patients,” Nephrology, Dialysis, Transplantation 22, no. Suppl 5 (2007): v 20–v 36, 10.1093/ndt/gfm 294.17586842 · doi ↗ · pubmed ↗