Is uterine artery embolisation a safe and effective modality to treat submucosal fibroids?
Rayhab Mashal, Neeral Patel, Bhavna Pitrola, Thomas Sewell, Asmaa Al-Kufaishi, Shabnam Taheri, Mohamad Hamady

TL;DR
Uterine artery embolisation effectively reduces submucosal fibroids with high patient satisfaction and low severe side effects.
Contribution
Demonstrates UFE's efficacy in reducing submucosal fibroid volume and its safety profile with minimal severe adverse events.
Findings
UFE reduced submucosal fibroid volume by 64% and achieved over 90% devascularization in 94.8% of cases.
84.5% of patients were discharged without further intervention, indicating high patient satisfaction.
Severe adverse events occurred in only 3.2% of patients, with pelvic infections being the most significant.
Abstract
• Uterine fibroid embolization (UFE) reduced the median volume of dominant submucosal leiomyomas by 64% and achieved over 90% devascularization in 94.8% of cases. • High patient satisfaction was observed, with 84.5% of patients successfully discharged without needing further intervention. • Severe adverse events were rare, affecting only 3.2% of patients, with pelvic infections being the most significant. • Mild adverse events occurred in 16.8% of patients, including infections requiring antibiotics and persistent vaginal discharge. • A multidisciplinary approach is essential for managing patients with submucosal leiomyomas undergoing UFE to ensure optimal treatment outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
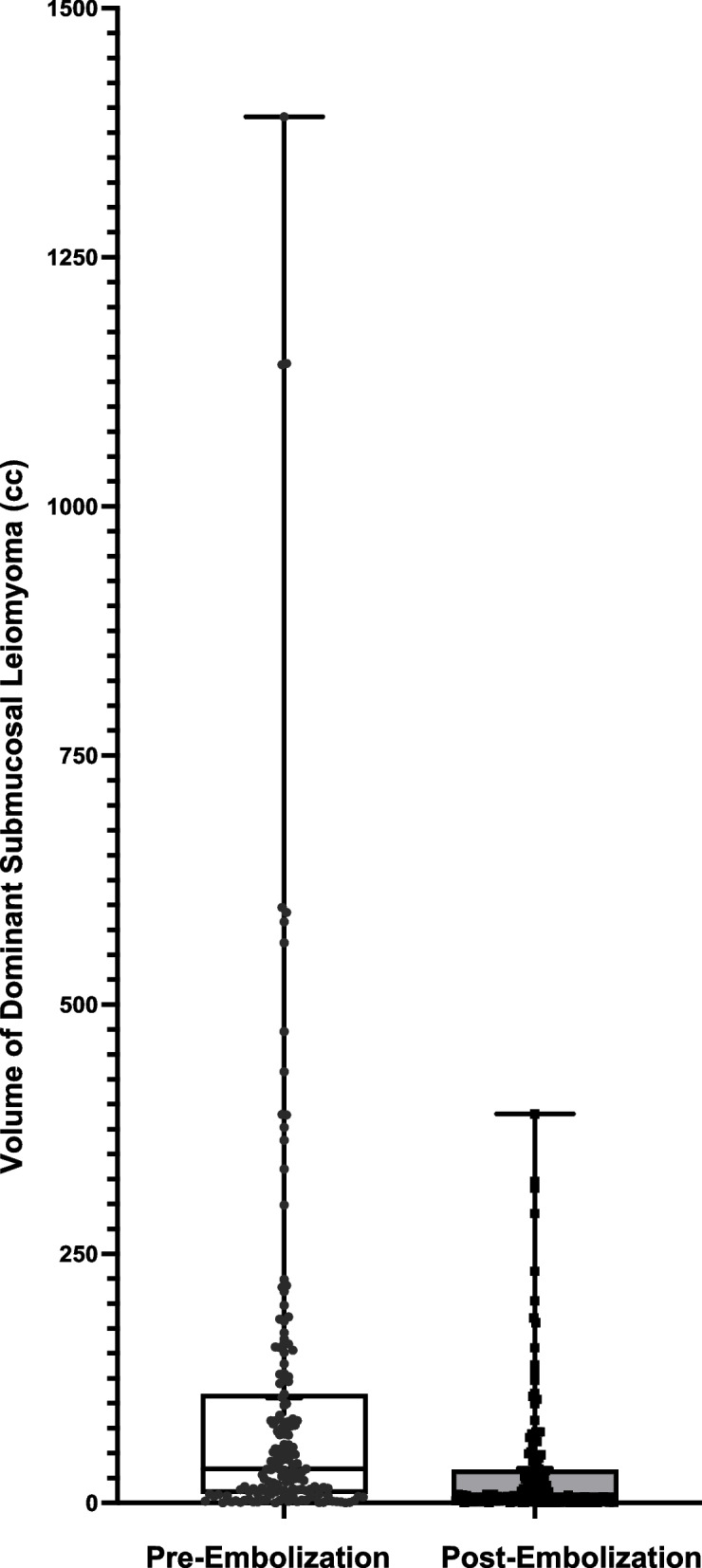 Figure 1
Figure 1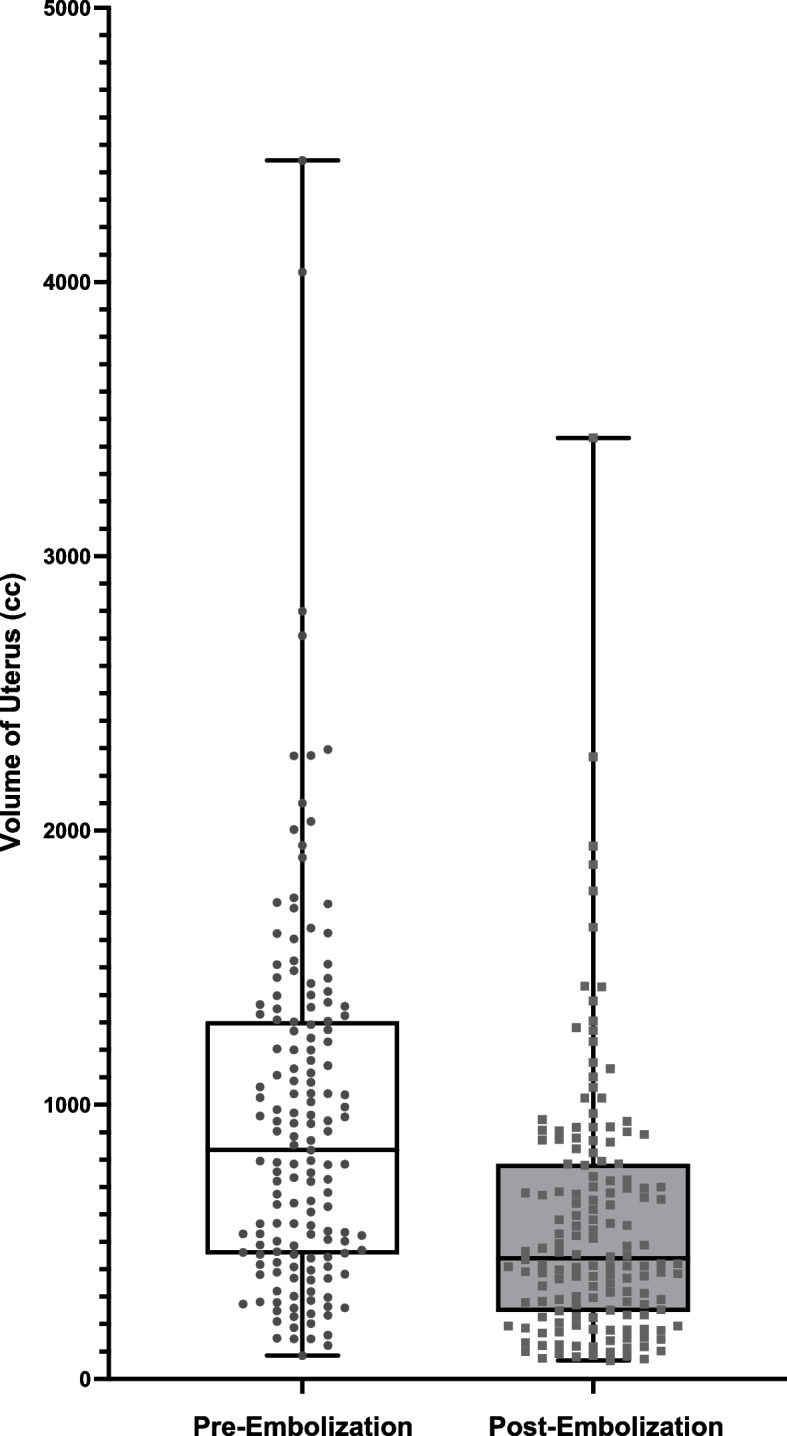 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Endometriosis Research and Treatment · Gynecological conditions and treatments
Introduction
Uterine leiomyomas are classified according to their location into three subtypes: submucosal, intramural, and subserosal leiomyomas [1, 2]. Submucosal leiomyomas are further classified into Type 0, which are mostly within the endometrial cavity; Type 1, which extend into the endometrial cavity with less than 50% of their components being intramural; and Type 2 leiomyomas, which have more than 50% of their components in the intramural region [2].
Among the different types of leiomyomas, submucosal leiomyomas are often regarded as the most troublesome variety because of their association with abnormal and often very heavy menstrual bleeding, along with reproductive issues such as infertility, recurrent miscarriages, or premature labour [3–5].
First introduced in 1976, hysteroscopic transcervical resection of submucosal leiomyoma is widely recognised the gold standard treatment for symptomatic submucosal leiomyomas and is considered a simple, safe, highly effective and minimally invasive (usually a day-case) procedure [6, 7]. However, there are limitations associated with this, including the size, number and location of the leiomyomas as well as the depth of invasion into the myometrium. If the submucosal leiomyomas are too large or deeply embedded within the myometrium, an abdominal myomectomy is usually considered [6, 7]. Laparoscopic myomectomy is associated with a faster recovery and is preferred, if feasible, but less ideal for patients with a greater number or larger fibroids [8]. However, as with TCRF, there are also limitations with abdominal myomectomy including an increased risk of intra-uterine adhesion formation which may affect fertility and/or an increased risk of perinatal complications [6, 7]. Data suggests that the risk of intra-uterine adhesion formation was as high as 31% following resection of a single leiomyoma and up to 45% for multiple leiomyomas [9].
Although a substantial body of evidence exists supporting UFE as an effective treatment option for patients with symptomatic leiomyomas, the role of UFE in patients with submucosal leiomyomas remains controversial, especially among the gynecologial community [10–14]. The main concerns are increased risk of pelvic infection, expulsion or prolapse of the leiomyoma into the endometrial cavity and persistent vaginal discharge [4, 6, 7]. There are limited studies that have evaluated the efficacy and outcome of UFE on submucosal leiomyomas specifically. The aim of this study was to evaluate the contemporary outcomes of UFE in patients with submucosal leiomyomas treated at a tertiary referral centre.
Materials & methods
The local Ethics Committee waived the need for approval for the registration and use of retrospective analysis of anonymized data. Each patient signed an informed consent form for the intervention.
Information was collected from the local Radiology Information System (RIS), the Picture Archiving and Communication System (PACS), and the comprehensive, integrated electronic health record system (Cerner Millennium®, Oracle Health).
Patient demographics
Data were collected from 155 patients identified with submucosal leiomyomas who underwent UFE between January 2013 and December 2022. The average age of the patients was 47.3 years (range 34–59 years).
Uterine and fibroid data collection and follow-up
All patients underwent preoperative MRI examinations of the pelvis. We utilised T2-weighted sequences (sagittal and axial), which are part of our MRI gynaecological fibroid protocol, to obtain various measurements. The collected data included size (craniocaudal (CC) x anteroposterior (AP) x transverse (TS) dimensions) and volume (CC x AP x TS × 0.52) of the uterus and the dominant submucosal fibroid both pre- and post-embolization. The post-IV contrast T1-weighted images in the sagittal plane were used to estimate the percentage of devascularization. The study recorded the number of submucosal, intramural, and subserosal leiomyomas for each patient. It then focused primarily on the volume and size of the submucosal leiomyoma.All patients had a follow-up post contrast Magnetic Resonance Imaging (MRI) study to review devascularization of leiomyomas, approximately 6 months post-UFE. They were also reviewed in the Gynaecology and Interventional Radiology clinics.
Criteria for technical and clinical success
The procedure was technically standardised. Super selective catheterisation of the uterine arteries was performed using a coaxial microcatheter technique. The embolic particles used were Contour™^P^ polyvinyl alcohol (Boston Scientific), with particle sizes of 355–500 microns or 500–710 microns, or Embozene™ microspheres (Boston Scientific), with particle sizes of 500–700 microns or 700- 900 microns.
The procedure was considered technically successful if blood flow was significantly reduced in both uterine arteries to 10 heartbeats. If only one uterine artery was successfully embolised, it is deemed a technical failure, except in cases where only a single uterine artery existed [15]. Clinical success was also recorded. Clinical success was defined as the resolution or satisfactory improvement of the patients presenting symptoms, such as menorrhagia or bulk-related pain, bloating, urinary urge, or constipation, without additional therapy [15].
Procedural adverse outcomes and further interventions
Post-procedural adverse outcomes were categorized into two primary groups. The first group comprised patients who experienced adverse events, which were documented and classified as mild, moderate, or severe based on the Society of Interventional Radiology (SIR) adverse event classification system [16]. Mild adverse events included persistent vaginal discharge beyond 8 weeks [17] or a pelvic infection requiring antibiotics alone. Severe adverse events encompassed pelvic infections that necessitated either a TCRF or an emergency total abdominal hysterectomy.
The second group comprised patients who required additional procedures. This group included those needing a second UFE procedure due to only one uterine artery being embolized during the initial treatment, as well as patients needing either a planned or unplanned TCRF, a myomectomy, or a hysterectomy for persistent symptoms. A planned TCRF was considered during the initial consultation when a large submucosal leiomyoma was identified, and both the consulting Interventional Radiologist and Gynecologist deemed UAE beneficial prior to the TCRF. A large fibroid was subjectively determined to be ≥ 10 cm.
Detailed information was gathered, including the timing, type of reintervention, clinical outcome, and length of hospital stay.
Statistical analysis
Discrete variables were presented as patient counts and percentages, while continuous variables were expressed as mean ± standard deviation. Differences between groups were evaluated using the paired t-test. Data collection was conducted with Excel (Microsoft, Washington, US), and statistical analysis was performed using GraphPad Prism (GraphPad LLC, San Diego, US). A *P-*value of less than 0.05 was considered statistically significant.
Results
Patient symptoms and prior procedures
From January 2013 to December 2022, a total of 724 patients underwent UFE for symptomatic uterine leiomyomas. Among these, 155 patients were identified as having submucosal leiomyomas.
Symptoms included heavy menstrual bleeding with clots in 134 patients (86%), prolonged menstrual cycles in 14 patients (9%), irregular menstrual cycles in 46 patients (30%), urinary frequency and urgency in 102 patients (66%), vaginal discharge in 50 patients (3.2%), exhaustion in 118 patients (76%), bloating in 132 patients (85%), and constipation in 15 patients (9.6%).
Nineteen (12%) of the patients had previously undergone myomectomy, 10 (6.5%) had a prior TCRF, and 4 (2.6%) had undergone hysteroscopy in the past.
Uterine and fibroid data
Table 1, Figs. 1 and 2 compare the volumes of uterine and dominant submucosal leiomyomas before and after embolization. The median uterine volume pre-embolization was 834.9 cc (range 85.0–4444.0 cc), with a post-embolization median volume of 440.4 cc (range 67.1–3432.0 cc). The median percentage decrease in uterine volume was 39.9% (range 0.2–91.0%). Table 1. Comparison of Uterus Volume and Dominant Submucosal Leiomyoma Volume Pre- and Post-Embolization. Review of Successful Devascularization Post-Embolization of Different Leiomyomas. Review of the Number of Submucosal Leiomyomas in Each Patient**Pre-EmbolizationPost-EmbolizationChange (%)*****P-*Value****Uterus Volume (cc)Median834.9440.439.9< 0.0001Median CI 95%680.2–970.6388.2–543.636.1–43.3Range85.0–4444.067.1–3432.00.2–91.0Mean949.2 ± 54.2574.3 ± 38.139.0 ± 1.6Mean CI 95%842.0–1056.3499.0–649.636.0–42.0Dominant Submucosal Volume (cc)Median34.208.364.0< 0.0001Median CI 95%24.2–51.35.7–13.957.7–69.7Range0.1–1391.00.01–390.41.5–99.7Mean105.5 ± 16.234.9 ± 5.460.9 ± 2.2Mean CI 95%73.6–137.424.3–45.556.5–65.3Number of Submucosal LeiomyomasMedian2.0Median CI 95%2.0–3.0Range1.0–10.0Mean2.7 ± 0.2Mean CI 95%2.4–3.0Devascularization of Submucosal Fibroids (%)Median100Median CI 95%100—100Range0–100Mean96.09 ± 1.5Mean CI 95%93.2–99.0Devascularization of Other Fibroid Subtypes – Intramural/Subserosal (%)**Median100Median CI 95%100—100RangeMean95.25 ± 1.3Mean CI 95%92.8–97.8Fig. 1Volume of dominant submucosal leiomyoma pre- and post-embolizationFig. 2Volume of uterus pre- and post-embolization
Patients presented with 1 to 10 submucosal leiomyomas (median 2). For intramural leiomyomas, the number ranged from 0 to 50 (median 10). Subserosal leiomyomas varied between 0 and 13 (median 2). The median pre-embolization volume of the dominant submucosal leiomyoma was 34.20 cc (range 0.1–1391.0 cc), while the post-embolization volume was 8.3 cc (range 0.01–390.4 cc). The median percentage decrease in volume was 64% (range 1.5—99.7%).
Technical success
Effective devascularization of submucosal fibroids exceeding 90% was achieved in 94.8% of patients. Likewise, 94.3% of patients obtained over 90% devascularization of the subserosal/intramural leiomyomas.
Complications
Table 2 outlines the observed complications. Twenty-one patients (13.5%) reported persistent vaginal discharge after UFE. While vaginal discharge following UFE is common, it typically resolves within 8 weeks [17]. Therefore, if a patient continued to experience this after two months, it was recorded as a complication. Table 2. Review of Complications and Further Procedures**Number of Patients****Percentage (%)**Interval between UAE and Second Procedure (Days) Median [Range]Complications – Requiring Emergency TreatmentMild Adverse Event (A) (38) Vaginal Discharge2113.5- Pelvic Infection –Antibiotics only53.211 [11–14]Severe Adverse Event (C) (38) Pelvic Infection –TCRF31.956 [5–81] Pelvic Infection –Total Abdominal Hysterectomy21.36, 26Further Procedures – Persistent Symptoms Post-UAE Second UAE21.3305, 720 Planned TCRF Post-UAE31.962 [4–417] Unplanned TCRF53.2369 [97–538] Myomectomy10.6563 Hysterectomy85.11188 [340–1455] Symptoms Improved – Discharged13184.5-One patient started hormonal treatment (Desogestrel) as her symptoms (menorrhagia) were persistent post-UFE. Her symptoms have improved and she has since been discharged from clinicOne patient had persistent symptoms post-UFE, but decided against any further intervention or medical management
Overall, 10 patients (6.5%) developed pelvic infections (Table 3). Five patients (3.2%) were successfully treated with antibiotics alone, three patients (1.9%) required a TCRF, while two patients (1.3%) underwent an emergency total abdominal hysterectomy (TAH) for an infected, necrotic fibroid. One of the patients who required an emergency TCRF did not respond to two courses of antibiotic treatment. She was initially treated with intravenous antibiotics 60 days post-UFE. The patient returned to the Emergency Department 80 days post-UFE with offensive vaginal discharge and urinary retention and was found to have a protruding necrotic fibroid. The patient underwent an eventful TCRF the following morning. Table 3. Details of patients with pelvic infectionPatient numberPresenting ComplaintDays after UAEMicrobiology ResultsAntibiotic, Route(per oral PO, intravenous IV) and DurationAdmission into hospital and how many days in hospitalOutcomeOutcome FibroidEmbolic size (Red = Right,Blue = Left)Embolic amount(vials)High Vaginal SwabUrine Microbiology Culture and Sensitivity (MC + S)Blood CulturePelvic Infection – Requiring Antibiotics OnlyPatient 1Right lower abdominal pain, fever and dark brown PV discharge2Candida AlbicansNo growthNo growthIV Cefuroxime and Metronidazole 2/7Stepped down to PO Co-amoxiclav for 7 daysYes – 2Discharged on oral antibiotic Co-amoxiclav 7-days courseDischarged from clinicPVA 355–5002.5PVA 500–7102PVA 355–5002Patient 1Fever, vomiting and minimal PV bleeding13Yeasts isolatedNo growthNo growthIV Cefuroxime and Metronidazole 3/7Yes—3Discharged on oral Cefalexin and Metronidazole 7-day courseDischarged from clinicPVA 355–500No recordPatient 2Fever9No growthNo growthNo growth-No-Discharged from clinicPVA 355–50012Patient 3Sepsis post-procedureFever4No growthNo growthNo growthIV Cefuroxime and MetronidazolePO Ciprofloxacin14Cefalexin, Ciprofloxacin and Metronidazole – 7-day courseDischargedPVA 355–5006PVA 500–7101Patient 4Fever, prolapsing fibroid*** Seen in ED and GP 4 times in five months with four courses of antibiotics***(presented to two different hospitals at 28 days then 112 days post procedure)28Staphylococcus aureusNo growthNo growthIV antibiotics on first presentation at different hospitalIV Co-amoxiclavFibroid passed PVDischarged on PO Co-amoxiclav 2/52Discharged from clinicPVA 355–5003PVA 355–5003PVA 500–7101Patient 5Fever11---IV Cefuroxime and MetronidazoleYes—5Discharged on PO antibiotics 2/52Discharged from clinic355–5004500–7101Pelvic Infection – Requiring TCRFPatient 6Fever and abdominal painAttended different hospital ED with avulsed fibroidRe-attended ED for TCRFNo recordNo record----Discharged from clinic700 Embozene Microspheres2700 Embozene Microspheres2Patient 7Fevers and abdominal pain60No growthNo growthNo growthIV Ceftriaxone and Metronidazole + STAT Amikacin 3/7Yes—3Discharged on oral Clindamycin & Ciprofloxacin for 14 daysTCRF for necrotic fibroid-followed by discharge from clinic355–5001 vial500–7101 vialsFevers and large necrotic fibroid prolapsing through cervix80Anaerobes + + + isolatedNo growthNo growthIV Co-amoxiclav 2/7Yes—2Discharged on oral Metronidazole and Ciprofloxacin for 7 daysDischarged from clinicPVA355–5001vialPVA500–7101vialPatient 8Fever20No recordNo recordNo recordNo recordNo record-Discharged from clinicEmbozene Microspheres 7002Embozene Microspheres 7002Pelvic Infection – Requiring Emergency TAH & BSOPatient 9Fever, abdominal pain26Scanty anaerobesNot performedNot performedIV Cefuroxime and Metronidazole escalated to IV MeropenemYes – 14 daysTAHTAHHistopathology: Histopathology: ischaemic and necrotic change, acute inflammation suggestion abscessPVA355–5002 vialsPVA355–5002 vialsPatient 10Fever, abdominal pain, prolapsing fibroid (21 cm)6Gram negative bacilli—Escherichia coliGram negative bacilli—Escherichia coliGram negative bacilli—Escherichia coliIV Ceftriaxone and Metronidazole and GentamicinYes – 12 daysTAHDischarged on oral Co-amoxiclav 7 daysTAHHistopathology:Uterus shows changes following UAE and secondary acute inflammation. Single leiomyoma—active endometritis following UAE. The leiomyoma has prolapsed through the cervixPVA 355–5003 vialsPVA355–5003 vials
Four patients were noted to pass their dominant submucosal leiomyoma per vagina, without any further intervention.
Table 2 illustrates the interval between the initial UFE procedure and the onset of complications. Patients treated with antibiotics alone for pelvic infections presented between 1 and 14 days post-UFE. Three patients with pelvic infections underwent TCRF at 5, 56, and 81 days post-UFE, respectively. The two patients who required emergency TAH had their surgeries at 6 and 26 days post-UFE.
Three patients had a planned TCRF prior to UFE because of the large size (≥ 10 cm) of their submucosal leiomyomas. These patients underwent uncomplicated TCRF procedures between 4 and 417 days after UFE, with a median interval of 62 days.
Twenty patients reported persistent symptoms during their follow-up appointments in the gynaecology clinic. Two patients (1.3%) underwent a second UFE procedure at 305 and 720 days post-UFE. In both cases, only one uterine artery was embolized during the initial procedure due to vasospasm and failure to cannulate the contralateral artery.
Three patients chose to undergo TCRF due to persistent heavy menstrual bleeding, while two opted for the procedure because of ongoing troubling vaginal discharge beyond 8 weeks. These procedures were performed between 97 and 538 days post-UAE (Table 2). One patient’s TCRF was delayed due to cardiac issues. When the procedure was eventually performed, no intracavity or submucosal fibroid was found, and thus no resection was required.
One patient opted for a myomectomy, which was performed 563 days post-UFE. Eight patients opted for a total abdominal hysterectomy (TAH) due to persistent symptoms, with these procedures occurring between 340 and 1455 days post-UFE.
Two patients had further clinic reviews for ongoing symptoms. One patient with persistent menorrhagia chose conservative management with Desogestrel, which has effectively controlled her symptoms, leading to her discharge from the clinic. Another patient, who did not wish to pursue further treatment for her symptomatic leiomyomas, was also discharged from the clinic.
Overall, 131 patients were satisfied with their results after undergoing UFE and were discharged from the clinic without the need for any further intervention, including a second embolization. The remaining patients were reviewed in the clinic following their secondary interventions. All but two of these patients have since been discharged. The two patients still under clinic review are awaiting TAH due to persistent fibroid-related symptoms and need to lower their body mass index before being considered for the procedure.
Discussion
A literature search was conducted to review studies evaluating complications in patients with submucosal leiomyomas following UFE. This search was challenging due to the limited amount of literature specifically addressing this subject, as most studies focus on all subtypes of leiomyomas. However, the most pertinent studies were reviewed and compared against our objectives and data. Table 4 summarizes the most relevant studies, highlighting their findings, conclusions, and limitations. Table 4. Summary of relevant studies, highlighting the findings, conclusions and limitationsStudyAimMain FindingsConclusionLimitationsBoris-Radeleff et al. [Boris-Radeleff 2009] [18]Retrospective review of 20 patients. Evaluated the frequency, probability and factors associated with expulsion of submucosal leiomyoma after UFEReviewed technical and clinical results at their one-year follow upTechnical success in all 20 patients with 2 (10%) minor and 1 (5%) major complicationsComplications:▪ Transient, post-procedural hypotension▪ Small post-interventional inguinal haematoma▪ One-day hospitalization for a patient with vaginal bleeding related to the expulsion of a dominant submucosal leiomyoma10 (out of 20) patients expelled their dominant submucosal fibroid in a time frame of 4 weeks- 3 months post-UFE, 19 patients without complicationsStatistically significant reduction in submucosal leiomyoma size and uterine volumeAll patients reported a reduction in their symptoms and were satisfied with their post-UFE resultsA limited number of patients Namkung et. al [Namkung 2018] [4]Retrospective review of 8 patientsEvaluating the safety and effectiveness of hysteroscopic myomectomy after UFE for large sized submucosal leiomyomas with deep myometrial invasionMean volume of the submucosal leiomyomas was 87.7 cm^3^, reviewed on MRIReduction in volume after UFE was 83.3%UFE was followed by a hysteroscopic myomectomy and all women improved symptoms with no recurrence one-year laterConcluded that there were no complications observed in patients post-UFEStudy was not reviewing patients with submucous leiomyomas who exclusively had a UFE but patients who underwent hysteroscopic myomectomy following UAEAl-Fozan et. al [Al Fozan 2002] [19]Presented a number of cases of septic uterus leading to early hysterectomyFive out of seven patients had submucous leiomyomas▪ Three patients were found to have septic uterine necrosis at surgery▪ Two patients had necrotic myomasAl Fozan argued that despite some authors viewing myoma expulsion as a complication, it may be a natural phenomenon with submucous leiomyomas and a cervical culture pre-UAE is recommended to avoid performing UAE in the presence of infectionSmall number of patients reviewedPelage et. al [Pelage 2000] [20]Prospectively cohort of 6 patients with submucosal fibroids out of 80 patients, evaluated the effectiveness and safety of UFE in the management of symptomatic uterine leiomyoma▪ Four women complained of necrotic fragments of a pedunculated submucosal leiomyoma expelled through the cervix during the first month post-procedure▪ Only 1 patient (17%) underwent a hysterectomy due to acute septic uterine necrosis 17-days post-UAE. Although this was put down to a large submucosal leiomyoma, a size was not specified in this caseFive patients reported no improvement of symptoms▪ Four patients underwent further myomectomy▪ One patient underwent a hysterectomySuperselective arterial embolization of the uterine arteries is an effective means of controlling symptomatic uterine leiomyomaSmall cohort (although only one patient developed septic necrotic uterus)Results did not specify which patients had submucous leiomyomasUnclear which subtype of leiomyomas the five patients who did not experience any improvement hadRajan et. al [Rajan 2004] [21]Retrospective review of UFE performed over a three-year period to identify risk factors (including location and size of dominant leiomyoma) for the development of intrauterine infection following UFE414 UFE procedures were performed in 410 patients148 patients (36.1%) had submucosal leiomyomas5 patients (3.4%) developed infectious complications and all were within the submucosal patient group▪ 4 patients required antibiotics alone▪ 5 th patient underwent a TCRF, however, during attempted hysteroscopic removal of the leiomyoma, the uterus was perforated and the patient underwent a hysterectomySignificant difference in the occurrence of intrauterine infectious complications in patients with submucosal leiomyomas versus those without (P = 0.006) with univariate analysisAuthors described this association was not significant with multivariate analysis, including embolic agent used (P = 0.71), quantity of embolic agent (P = 0.33), size (P = 0.74) and location (P = 1.0) of dominant leiomyoma and use of prophylactic pre-procedure antibiotics (P = 0.81)Authors concluded that of the variables examined, none were found to be predictive of developing intrauterine infectious complicationsUsing transvaginal ultrasound imaging to review size and location of the leiomyomas
The two main sources of evidence are Boris-Radeleff et al. [18] and Rajan et al. [21]. Boris-Radeleff et al. assessed the frequency, probability, and factors associated with the expulsion of submucosal leiomyoma following UFE, along with the technical and clinical outcomes at one-year follow-up. Technical success was achieved in all 20 patients, with 2 (10%) minor complications and 1 (5%) major complication. These complications included transient post-procedural hypotension, a small post-interventional inguinal hematoma, and a one-day hospitalization for a patient with vaginal bleeding due to the expulsion of a dominant submucosal leiomyoma. Although half of the patients experienced leiomyoma expulsion, this occurred without requiring medical intervention in 95% of cases (19 out of 20 patients). The study also revealed a statistically significant (P = 0.05) decrease in both the size of submucosal leiomyoma and overall uterine volume. All patients reported an improvement in their symptoms and expressed satisfaction with their post-UFE outcomes.
Rajan et al. [21] conducted a retrospective review of UFE procedures performed over three years to identify risk factors for intrauterine infection post-UFE. They assessed various factors, including the location and size of the dominant leiomyoma. The study involved 414 UFE procedures in 410 patients, with 148 patients (36.1%) having submucosal leiomyomas. Among these, 5 patients (3.4%) developed infectious complications, all of whom had submucosal leiomyomas. Four patients were treated with antibiotics alone, while the fifth required a TCRF. During the hysteroscopic removal of the leiomyoma, the uterus was perforated, necessitating a hysterectomy.
The incidence of intrauterine infectious complications was significantly higher in patients with submucosal leiomyomas compared to those without (P = 0.006), according to univariate analysis. However, multivariate analysis showed that this association was not significant when considering the embolic agent used (P = 0.71), the quantity of the embolic agent (P = 0.33), the size (P = 0.74) and location (P = 1.0) of the dominant leiomyoma, and the use of prophylactic pre-procedure antibiotics (P = 0.81). The authors concluded that none of the variables examined were predictive of developing intrauterine infectious complications. They noted limitations in their study, such as the relatively small sample size (414 patients) and the use of transvaginal ultrasound imaging to assess the size and location of the leiomyomas.
The literature addressing our primary objective is relatively sparse. Many of the studies referenced earlier either advise against performing UFE in patients with submucosal leiomyomas, present findings based on a small sample size, or fail to specifically distinguish between patients with submucosal leiomyomas and those with other types of fibroids. Consequently, there is a lack of comprehensive and detailed research that directly explores the outcomes and efficacy of UFE in the context of submucosal leiomyomas.
This study involved a larger sample size compared to those previously mentioned, encompassing 155 patients diagnosed specifically with submucosal leiomyomas out of a total of 724 patients who underwent UFE during the study period. Each patient’s leiomyomas were classified according to the FIGO classification system to ensure precise categorization. Both pre- and post-UFE evaluations were conducted using MRI, which offers superior accuracy compared to transvaginal ultrasound scanning [22].
This cohort demonstrated that UFE is a safe and effective treatment for patients with submucosal leiomyomas. The occurrence of pelvic infections was relatively low at 6.5%, with only five patients requiring additional surgical interventions such as TCRF or TAH.
The main limitation of the current study is the retrospective design. However, the patient cohort is drawn from the local catchment area, and all patient medical records are maintained in the hospital’s electronic Cerner system. Another limitation is that data collection focused on the volume of the dominant submucosal leiomyoma. Patients had between 1 and 10 submucosal leiomyomas, with a median of 2. Despite these limitations, the positive clinical outcomes observed in most patients suggest that the study has captured the most relevant findings.
In conclusion, this study demonstrates that UFE is a safe and effective treatment option for patients with symptomatic submucosal leiomyomas and is associated with high clinical success. Implementing clear pathways and adopting a multidisciplinary team approach is critical in managing these patients to ensure the best treatment options are presented.