Diagnostic Value of Peripheral Blood Smear Tests in Identifying Candida Infections in a Tertiary Care Setting: A Case Series
Malvika Gaur, Tushar Sehgal, Ginni Bharti, Hemapriya J Babu, Immaculata Xess

TL;DR
This case series explores how peripheral blood smear tests can help detect Candida infections quickly and inexpensively, especially in hospitals with limited resources.
Contribution
The study highlights the diagnostic potential of peripheral blood film tests as a rapid and cost-effective screening method for Candida infections.
Findings
Budding yeasts were identified in peripheral blood films of three out of four patients with Candida infections.
Peripheral blood film tests provided rapid preliminary insights, aiding early antifungal therapy initiation.
Blood culture remains the gold standard, but PBF tests are a valuable initial screening tool in resource-limited settings.
Abstract
Invasive fungal infections (IFIs) are a significant cause of morbidity and mortality in hospitalized patients, particularly among neonates and immunocompromised individuals. Candida species are one of the most commonly associated pathogens associated with IFIs. We present a case series of four patients with IFIs. All cases underwent peripheral blood film (PBF) examination, blood culture, and serum galactomannan testing. Budding yeasts were found in the PBF of three out of four cases. The findings were confirmed by culture. While blood culture remains the gold standard for diagnosing IFIs, the PBF test demonstrated its value as a rapid and cost-effective initial screening tool, especially in resource-limited settings. PBF tests can offer valuable preliminary insights, facilitating further diagnostic evaluation and early initiation of antifungal therapy. These findings underscore the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
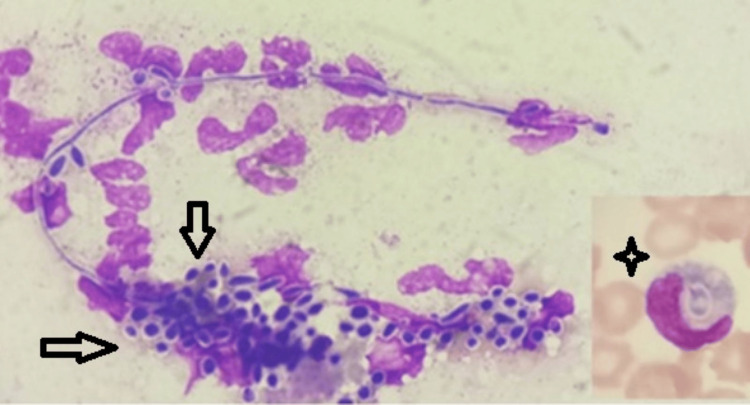 Figure 1
Figure 1| Case | Age | Gender | Predisposing condition | Outcome |
| 1 | 10 days | Male | Preterm, low birth weight, post-surgical intestinal atresia | Died |
| 2 | 40 years | Female | Post-surgery for adenocarcinoma of the colon | Responded to antifungal treatment |
| 3 | 49 years | Male | Hepatitis C, recurrent ascites | Died |
| 4 | 16 days | Male | Low birth weight | Died |
| Case | Age | Gender | Hemoglobin (g/dL) | Normal reference range of hemoglobin (g/dL) | WBC (10^9/L) | Normal reference range of WBC (10^9/L) | Platelet (10^9/L) | Normal reference range of Platelet (10^9/L) | Yeast form in PBF | Blood/swab Culture | Serum galactomannan |
| 1 | 10 days | Male | 9.5 | 11-17.3 | 15.5 | 3.1-21.6 | 21 | 152-472 | Detected | Positive for | Positive |
| 2 | 40 years | Female | 10.5 | 12-15 | 19.9 | 4-11 | 80 | 150-450 | Detected | Positive for | Positive |
| 3 | 49 years | Male | 8.9 | 13-17 | 11 | 4-11 | 155 | 150-450 | Detected | Positive for | Positive |
| 4 | 16 days | Male | 12.5 | 11-17.3 | 18.9 | 3.1-21.6 | 44 | 152-472 | Detected | Positive for | Positive |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Bacterial Identification and Susceptibility Testing
Introduction
Invasive fungal infections (IFIs) are a significant contributor to morbidity and mortality among hospitalized patients, particularly those with compromised immune function. Globally, the incidence of IFIs is rising, estimated at approximately six cases per 100,000 individuals annually [1]. *Candida *species are one of the most frequently implicated pathogens, especially among critically ill patients in intensive care units (ICUs), neonates, trauma patients, and the immunocompromised [2, 3]. An Indian study identified *Candida *species as the leading cause of bloodstream infections in ICUs, with Candida tropicalis, Candida parapsilosis, Candida auris, Candida albicans, and Candida glabrata being the most commonly isolated strains [4].
Invasive candidiasis (IC) accounts for roughly 9% of hospital-acquired bloodstream infections in the United States, ranking among the most common pathogens in medical, surgical, and ICU environments [5]. Likewise, Indian data have revealed a growing prevalence of non-albicans *Candida *species, such as Candida tropicalis, Candida parapsilosis, Candida auris, and Candida glabrata, particularly in ICU settings, possibly driven by widespread fluconazole use [6]. In a multicentric observational study conducted at 27 Indian ICUs, among 1,400 ICU-acquired candidemia cases, 65.2 % were adult. The important finding of the study was the vast spectrum of agents (31 *Candida *species) causing candidemia and a high rate of isolation of Candida tropicalis (41.6 %). Azole and multidrug resistance were seen in 11.8% and 1.9% of isolates. Public sector hospitals reported a significantly higher presence of the relatively resistant Candida auris and Candida rugosa. The 30-day crude and attributable mortality rates of candidemia patients were 44.7% and 19.6 %, respectively. The various significant independent predictors of mortality included admission to a public sector hospital, APACHE II score (short for Acute Physiology and Chronic Health Evaluation II) at admission, underlying renal failure, central venous catheterization, and steroid therapy [7].
Although blood culture remains the gold standard for diagnosing IFIs, peripheral blood film (PBF) examination is an often underutilized yet potentially valuable screening method. Identifying intracytoplasmic budding yeast cells within neutrophils or monocytes during PBF examination can indicate fungal infection early [1, 8-11]. While PBF examination is less sensitive than blood cultures, it may offer more rapid preliminary evidence, especially in severely ill patients who require immediate intervention [12]. However, interpreting PBF test results can be challenging in cases of low fungal load, emphasizing the need for meticulous examination and clinical awareness [13].
Case presentation
Table 1 shows the clinical details of all the cases.
Table 2 shows the results of all laboratory investigations.
A representative figure (Figure 1) shows the PBF examination with pseudohyphae and intracellular and extracellular round-to-oval budding yeast cells engulfed by a monocyte.
Peripheral blood film (PBF) examination shows pseudohyphae and intracellular and extracellular round-to-oval budding yeast cells (multiple arrows) engulfed by a monocyte (four-point star; Leishman and Giemsa stain, x1000)
Case 1: a preterm neonate with intestinal atresia
A preterm, low-birth-weight 10-day-old male neonate was diagnosed with intestinal atresia and admitted to the neonatal intensive care unit (NICU) for further management. He required abdominal surgery for the correction of the intestinal obstruction. Initially, a complete blood count (CBC) and PBF examination showed normal results. However, thrombocytopenia was noted by day 5 of admission, prompting further investigation. On day 20, CBC revealed a white blood cell (WBC) count of 15.5 x 10^9/L (normal range, 3.1-21.6 x 10^9/L), hemoglobin of 9.5 g/dL (normal range, 11-17.3 g/dL), and a platelet count of 21 x 10^9/L (normal range, 152-472 x 10^9/L). On PBF examination, intracellular and extracellular round-to-oval budding yeast cells were observed, engulfed by both monocytes and neutrophils. A distinct zone of clearing was noted around the budding yeast cells, and pseudohyphae were also present. The neutrophils were increased, and toxic granules were demonstrated, accompanied by monocytosis. The findings suggest disseminated invasive fungal infection; a fungal culture was advised. Blood samples from the peripheral and central line catheters were sent for culture, and intravenous antifungal therapy was initiated the same day. Despite these interventions, blood culture results were negative. Follow-up blood samples collected on day 21 and day 22 showed a similar PBF picture, with persistent fungal forms engulfed by neutrophils and monocytes. However, by day 23, the fungal spores were no longer visible in the PBF examination, though thrombocytopenia persisted. A pharyngeal swab culture identified Candida albicans, and direct potassium hydroxide (KOH) preparation confirmed the presence of fungal elements. Additionally, the urine routine test revealed budding yeast forms (3+) (normal range, no yeast forms).
Case 2: an adult female with adenocarcinoma of the colon
A 40-year-old female patient with a medical history significant for adenocarcinoma of the colon was admitted to the ICU following multiple surgeries, including tumor resection and lymph node dissection. The patient required a colostomy bag and a central venous catheter for administering antibiotics and steroids as part of her postoperative management. On day 15 of hospitalization, the patient developed signs of systemic infection. Laboratory investigations revealed hemoglobin of 10.5 g/dL (normal range, 12-15 g/dL), WBC of 19.9 × 10^9/L (normal range, 4-11 × 10^9/L), and a platelet count of 80 × 10^9/L (normal range, 150-450 × 10^9/L). PBF examination showed fungal blastospores and pseudohyphae, indicating the presence of an invasive fungal infection. Additionally, neutrophilic leukocytosis and monocytosis were noted. The serum galactomannan test was positive. Blood samples were sent for culture, and empirical antifungal therapy with amphotericin B was promptly initiated. Subsequent blood culture results confirmed the presence of Candida albicans. Alongside the fungal infection, blood cultures isolated Klebsiella pneumoniae, a carbapenem-resistant gram-negative bacterium. Antibiotic susceptibility testing using the VITEK 2 system (bioMérieux Inc., Durham, NC, USA) revealed that the Klebsiella pneumoniae strain was sensitive only to colistin, necessitating the use of colistin. By the third day of antifungal therapy, a repeat PBF examination showed no fungal elements, indicating a successful initial response to treatment. A periodic acid-Schiff (PAS) stain performed on the initial blood smear further validated the diagnosis of invasive fungal infection by highlighting fungal structures. Despite the complexity of managing dual infections involving Candida albicans and multidrug-resistant Klebsiella pneumoniae, the patient’s condition improved with the combined antifungal and antibiotic therapy.
Case 3: an adult male with hepatitis C and recurrent ascites
A 49-year-old male patient with a longstanding history of hepatitis C virus infection was admitted to the hospital for the evaluation and management of recurrent ascites and jaundice. During his stay, the patient developed clinical features suggestive of systemic infection. PBF examination revealed intracellular budding fungi, raising the suspicion of IC. Further diagnostic workup included fungal culture, which confirmed the presence of Candida glabrata. The serum galactomannan test was also positive, indicating fungal involvement. CBC revealed hemoglobin of 8.9 g/dL (normal range, 13-17 g/dL), WBC of 11 × 10^9/L (normal range, 4-11 × 10^9/L), and a platelet count of 155 × 10^9/L (normal range, 150-450 × 10^9/L). The patient's pleural fluid culture also grew *Klebsiella *species, further complicating the clinical picture. C-reactive protein (CRP) levels were elevated at 87.5 mg/L (normal range, <3 mg/L), corroborating the presence of a significant inflammatory or infectious process. The patient's condition deteriorated rapidly despite initiating antifungal therapy and addressing the bacterial infection. The invasive fungal infection, combined with his underlying hepatitis C and bacterial co-infection, led to worsening clinical status. Unfortunately, the patient passed away shortly after the diagnosis of disseminated invasive fungal infection was made, highlighting the critical nature of fungal infections in immunocompromised individuals.
Case 4: a neonate with sepsis and low birth weight
A 16-day-old male neonate with low birth weight was brought to the hospital with clinical signs of sepsis. Initial investigations included a CBC and PBF examination. CBC revealed hemoglobin of 12.5 g/dL (normal range, 11-17.3 g/dL), WBC of 18.9 × 10^9/L (normal range, 3.1-21.6 × 10^9/L), and platelet count of 44 × 10^9/L (normal range, 152-472 × 10^9/L) during hospitalization. PBF examination revealed intracellular budding fungi, prompting further investigation for a suspected fungal infection. The blood culture identified Candida albicans, and the serum galactomannan test confirmed the diagnosis of IC. A urine culture also showed similar findings. Despite the initiation of aggressive antifungal therapy, the neonate’s condition continued to decline. The combined effects of invasive fungal infection and sepsis overwhelmed the neonate’s fragile physiology. Unfortunately, the neonate succumbed to sepsis shortly after the fungal infection was diagnosed, underscoring the critical importance of early detection and intervention in cases of neonatal fungal infections.
Discussion
Our study emphasizes the potential role of PBF examination in diagnosing IC, a finding consistent with national and international studies. In our case series, intracellular budding yeast cells were detected on PBF examination, correlating with positive blood culture results and underscoring the value of PBF examinations for early identification. This observation aligns with previous Indian studies that successfully employed PBF examinations to diagnose *Candida *infections, particularly in ICU patients and neonates [4,10].
Hirai et al. [14] analyzed 36 cases in which the PBF examination showed candidemia. The most frequently isolated species was Candida parapsilosis (35.1 %), followed by Candida albicans (29.7 %). The overall mortality rate was 53.6 %. The time from the discovery of yeast-like pathogens using PBF to death ranged from a few hours to 93 days (median 19 days) [14]. Similarly, Kim et al. [15] observed that budding yeast cells within neutrophils on PBF could be an early indicator of candidemia. In our findings, Candida albicans was the most frequently identified species in both PBF and blood culture, consistent with prior Indian studies reporting Candida albicans as the predominant pathogen in hospitalized patients [6].
Timely diagnosis and initiation of antifungal therapy are critical, particularly for neonates and critically ill individuals. Despite treatment, IC is associated with high mortality rates; some studies report mortality of up to 55% in adults and 80% in neonates with Candida infections [16, 17]. Early detection is essential, and PBF examination can be a valuable adjunct to other diagnostic approaches in improving patient outcomes.
Although PBF examination has limitations, such as lower sensitivity and dependence on the fungal load, it remains a rapid, non-invasive screening tool. When combined with clinical judgment, blood cultures, and fungal antigen tests, careful examination of PBF can significantly contribute to effectively managing IFIs.
Conclusions
PBF examinations can be a valuable tool for the early detection of IFIs, especially Candida, particularly in neonates and critically ill adults. Although its sensitivity is lower than that of blood cultures, PBF examinations can offer important diagnostic insights when used alongside other methods, such as blood cultures and fungal antigen testing. More extensive studies are needed to further validate the effectiveness of PBF examinations in diagnosing and managing IFIs, especially in high-risk patient groups.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sensitivity of peripheral blood smear review for the diagnosis of Candida fungemia Arch Pathol Lab Med Branda JA Ferraro MJ Kratz A 9710113120071722713010.5858/2007-131-97-SOPBSR · doi ↗ · pubmed ↗
- 2An undual presentation of candidaemia primarily detected on peripheral blood smear Bombay Hosp J Vartak UC Vartak S Taklikar S Baradkar VP Bhatt NK Patel H 8889502008 https://www.semanticscholar.org/paper/An-Unusual-Presentation-of-Candidaemia-Primarily-on-Chakravarty-Vartak-Vartak/0009 dcc 8efeb 723827 f 377d 5c 34f 87be 886880 bb
- 3Budding yeast cells in peripheral blood smear: clue to candidemia Infect Chemother Cho SY Chae H Kim M Lee DG Kim HJ 3423434820162803248710.3947/ic.2016.48.4.342PMC 5204016 · doi ↗ · pubmed ↗
- 4The incidence, aetiology and antimicrobial susceptibility of central line-associated bloodstream infections in intensive care unit patients at a private tertiary care hospital in Mumbai, India Indian J Med Microbiol Singhal T Shah S Thakkar P Naik R 5215263720193243687410.4103/ijmm.IJMM_20_3 · doi ↗ · pubmed ↗
- 5Bench-to-bedside review: Candida infections in the intensive care unit Crit Care Méan M Marchetti O Calandra T 2041220081827953210.1186/cc 6212 PMC 2374590 · doi ↗ · pubmed ↗
- 6Epidemiology and antifungal susceptibility of Candida species in a tertiary care hospital, Kolkata, India Curr Med Mycol Bhattacharjee P 20272201610.18869/acadpub.cmm.2.2.5PMC 549030128681016 · doi ↗ · pubmed ↗
- 7Incidence, characteristics and outcome of ICU-acquired candidemia in India Intensive Care Med Chakrabarti A Sood P Rudramurthy SM 2852954120152551030110.1007/s 00134-014-3603-2 · doi ↗ · pubmed ↗
- 8Intracellular yeasts in a peripheral blood film leads to a diagnosis of Candida parapsilosis fungaemia Br J Haematol Fenomanana J Harzallah I Lohmann C Gharbi R Debliquis A Drénou B 31819120203274380710.1111/bjh.17020 · doi ↗ · pubmed ↗