Deciphering Acute Coronary Syndromes Pathobiology Through Proteomics
Gabriele Nieddu, Marilena Formato, Antonio Junior Lepedda

TL;DR
This paper reviews how proteomics has advanced our understanding of the biology behind acute coronary syndromes and identified potential biomarkers for diagnosis and treatment.
Contribution
The paper provides a critical overview of untargeted omics research in identifying biomarkers for acute coronary syndromes over the past two decades.
Findings
Proteomics has identified novel circulating and tissue biomarkers relevant to acute coronary syndromes.
Advancements in proteomic technologies have revealed pathways involved in atherosclerotic degeneration.
Multiple biological matrices have been studied to uncover markers for early diagnosis and therapeutic targets.
Abstract
Acute coronary syndrome (ACS) refers to a spectrum of conditions characterized by a sudden decrease in blood flow to the heart. This includes unstable angina, the mildest form, as well as non-ST- and ST-segment elevation myocardial infarction. The primary cause of ACS is typically the rupture or erosion of an atherosclerotic plaque in a coronary artery, resulting in the formation of a blood clot that can, partially or completely, block the blood flow to the heart muscle. The ongoing discovery and comprehension of emerging biomarkers for atherosclerosis could enhance our capacity to predict future events, particularly when integrated alongside traditional risk factors in assessing overall risk profiles. With advancements in proteomic technologies, large-scale approaches have been increasingly instrumental in unraveling pathways implicated in atherosclerotic degeneration and identifying…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
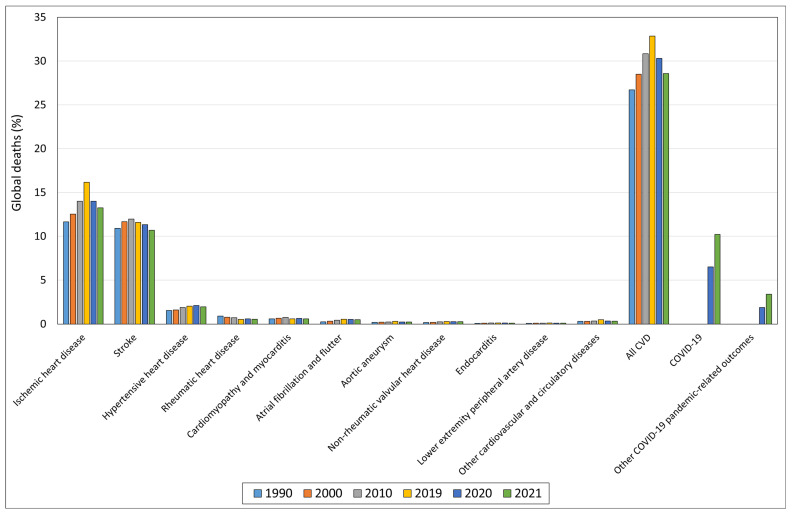 Figure 1
Figure 1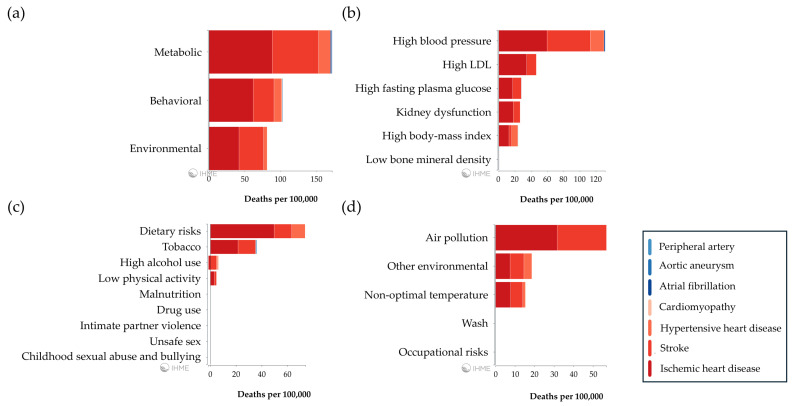 Figure 2
Figure 2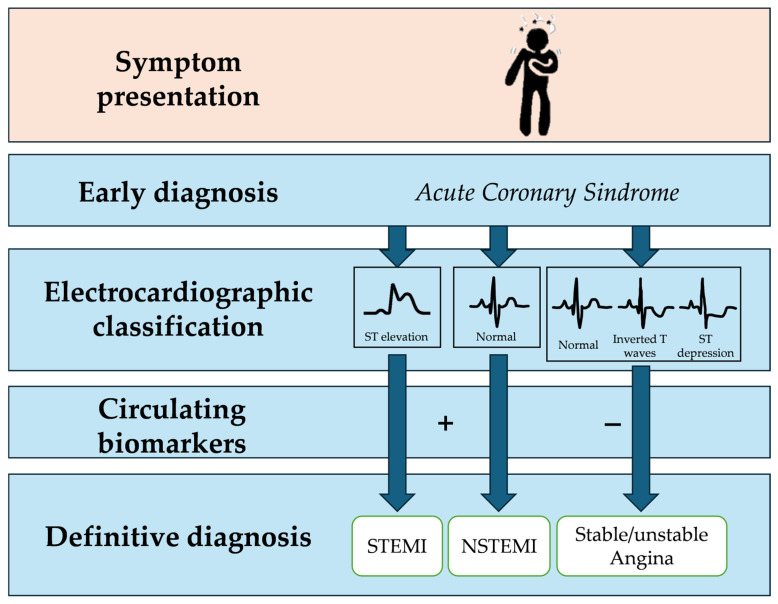 Figure 3
Figure 3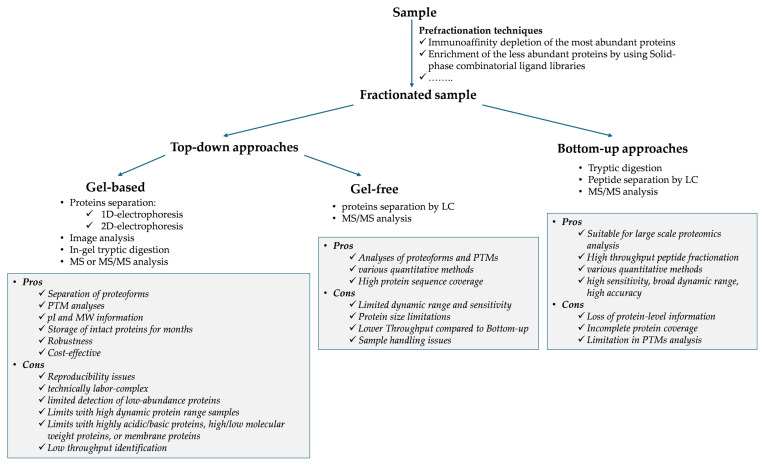 Figure 4
Figure 4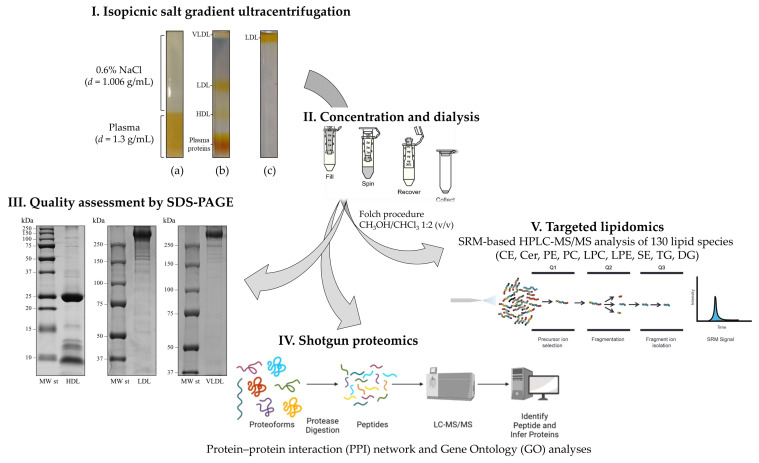 Figure 5
Figure 5 Figure 6
Figure 6- —Fondazione di Sardegna
- —European Union
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtherosclerosis and Cardiovascular Diseases · Advanced Proteomics Techniques and Applications · Protease and Inhibitor Mechanisms
1. Introduction
Despite significant advancements in diagnosis and treatment, cardiovascular disease (CVD) remains the leading cause of death and illness globally, with a higher prevalence observed in developed countries [1]. In 2019, CVD accounted for approximately 33% of global deaths, a figure that slightly decreased to 29% in 2021, representing ischemic heart disease and stroke as the main contributors. Particularly concerning is the upward trend observed over the last three decades (1990–2019), with only an apparent decline during the COVID-19 pandemic years, likely influenced in part by COVID-19 and COVID-19-related fatalities (Figure 1).
Several metabolic, behavioral, and environmental risk factors are known to contribute to overall CVD-related global deaths (Figure 2).
Currently, cardiovascular risk prediction, which still relies on traditional risk factors, can be unsatisfactory. In this scenario, identifying circulating biomarkers of subclinical atherosclerosis is of critical importance to improve cardiovascular risk prediction and early intervention with targeted therapies, potentially reversing/slowing disease progression as well as preventing major adverse cardiovascular events.
Acute coronary syndrome (ACS) refers to a spectrum of conditions characterized by a sudden decrease in blood flow to the heart. It includes unstable angina, the mildest form, as well as non-ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction (STEMI) [2]. ACS is primarily caused by the rupture or erosion of an atherosclerotic plaque within a coronary artery, resulting in the formation of a blood clot that can partially or completely block blood flow to the heart muscle. The presence of coronary plaques may cause chest pain or discomfort, known as angina, which can be classified as stable or unstable depending on its severity. Additional symptoms may include shortness of breath, sweating, nausea, lightheadedness, or fainting. Early recognition and timely treatment are critical to limit heart muscle damage, reduce complications, and improve patient outcomes.
ACS diagnosis relies on a combination of clinical evaluation, electrocardiography (ECG), and blood tests [3]. However, symptoms such as chest pain are atypical or absent in approximately one-third of patients with ACS, and ST-elevation may also be missing. These factors can contribute to delays in diagnosis and management (Figure 3).
An early diagnosis at admission is crucial for promptly identifying patients with symptoms suggestive of acute CVD. To achieve this, various specific circulating biomarkers, released into the plasma following acute cardiovascular events, are utilized, including brain natriuretic peptide [4,5], high-sensitivity C-reactive protein (hs-CRP) [6,7,8], heart-type fatty acid binding protein (H-FABP) [9,10], creatine kinase-MB (CK-MB) [11,12], and high-sensitivity cardiac troponin (hs-cTn) [13,14,15]. As current tests for diagnosing ACS are not definitive, coronary angiography is often performed, carrying inherent risks associated with this invasive procedure. Consequently, developing non-invasive, multi-marker-based strategies with improved specificity and sensitivity would be both clinically and economically beneficial [16]. Treatment focuses on restoring blood flow to the heart muscle and minimizing myocardial damage. This includes medications such as antiplatelet agents (e.g., aspirin, clopidogrel), anticoagulants (e.g., heparin, enoxaparin), nitroglycerin, beta-blockers, angiotensin-converting enzyme inhibitors, and statins. For patients with STEMI, revascularization procedures, including percutaneous coronary intervention or coronary artery bypass grafting, may be required to reestablish blood flow to the affected heart tissue [17].
Atherosclerosis is a chronic inflammatory condition characterized by the buildup of plaque in the arteries, driven by an interplay between genetic and environmental risk factors such as hypertension, diabetes, hyperlipidemia, high-fat diets, smoking, and physical inactivity [18].
The physiological coronary artery wall comprises three concentric layers: the tunica intima (facing the vessel lumen), the tunica media, and the tunica adventitia. The tunica intima consists of a continuous monolayer of endothelial cells anchored to a basement membrane, playing vital roles in vascular homeostasis, coagulation, inflammation, and tissue growth and repair. Endothelial dysfunction is an early event in atherosclerotic lesion development, marked by the overexpression of adhesion molecules and the secretion of pro-inflammatory and chemotactic cytokines [19,20]. Beneath the intima lies the tunica media, a thick, contractile layer of smooth muscle cells (SMCs) responsible for vessel structural integrity and blood flow and pressure regulation. SMCs contribute to atherogenesis through events such as migration, proliferation, and extracellular matrix (ECM) secretion. During plaque formation, SMCs migrate into the intima, where they proliferate and produce ECM proteins, thickening the arterial wall and narrowing the lumen, which reduces blood flow. Additionally, SMCs can internalize oxidized low-density lipoprotein (LDL), transforming themselves into foam cells that contribute to the formation of the necrotic core. SMCs may also adopt osteoblast-like or chondrocyte-like phenotypes, promoting vascular calcification [21]. The outermost layer, the tunica adventitia, contains a collagen-rich ECM that provides tensile strength to the vessel.
Among the well-established risk factors for atherosclerosis, elevated plasma levels of cholesterol-rich lipoproteins, particularly low-density lipoproteins (LDLs), are closely linked to the early stages of lesion formation [22]. LDL particles can become trapped in the subendothelial space of arteries through specific interactions with ECM components, leading to the formation of fatty streaks [23]. These fatty streaks represent the first visible sign of the atherosclerotic process and can progress toward the formation of plaque, which exhibits considerable variability between individuals in terms of growth rate and pathological characteristics [24]. The erosion or rupture of advanced plaques can trigger thrombosis, resulting in acute clinical events such as ACS, stroke, or peripheral artery occlusion [25,26].
Significant efforts have been dedicated to understanding the factors that contribute to plaque vulnerability and to identifying reliable and specific markers that predict a plaque’s susceptibility to ulceration to prevent adverse clinical events associated with thrombosis and arterial occlusion [27]. Evidence indicates that unstable plaques are characterized by heightened inflammation, increased proteolytic activity [28,29], and a pro-oxidant environment [30,31].
Over the past two decades, advancements in proteomic technologies have facilitated large-scale investigations into the pathways driving atherosclerotic degeneration. Through the comprehensive analysis of protein expression, modifications, and interactions, proteomics represents a powerful tool for discovering more sensitive and specific biomarkers, contributing to CVD management in clinical practice by enabling earlier diagnosis, personalized risk stratification, and more targeted therapy [32,33,34,35]. To address this challenge, various untargeted proteomics technologies have been employed, including one-dimensional and two-dimensional electrophoresis (1-DE and 2-DE) combined with mass spectrometry (MS) analyses, and gel-free MS-based proteomics (Figure 4). These methods have been applied to a wide range of human-derived matrices [36], such as vascular cells [37,38,39], arterial tissues [40], laser-capture microdissected samples [41], secretomes [42], plasma/serum [43], urine [44], and microparticles [45,46,47]. Platelets, key regulators of inflammation, immune responses [48,49], and targets for thrombotic event prevention, have also been studied using diverse omics approaches, including proteomics, lipidomics, metabolomics, transcriptomics, and translatomics [50]. Proteomics has been further applied to animal models, such as pigs, to deepen our understanding of coronary atherogenesis [51,52]. Emerging lipidomics studies of plasma and lipoproteins [53,54,55], as well as atherosclerotic tissues [56,57], have complemented proteomics, offering additional insights into atherosclerosis progression and plaque degeneration. Additionally, powerful targeted high-throughput proteomics platforms, including Olink and SomaScan, have been gaining traction recently, allowing for thousands of protein measurements simultaneously [58].
This chapter reviews and critically evaluates the major findings of the past 20 years, providing an overview of untargeted proteomics’ contribution to understanding the pathobiology of ACS.
2. Identification of ACS Circulating Biomarkers Through Untargeted MS-Based Technologies
Plasma is one of the most valuable matrices for discovering new biomarkers, as it contains both resident proteins, which make up the majority, and proteins released from vascular cells and tissues. However, plasma proteomics is challenged by both the presence of thousands of low-abundance proteins as well as the high dynamic range of protein concentrations [59]. Up to 99.9% of plasma proteins consist of the 21 most abundant ones, while the remaining 0.1% includes about 50,000 low-abundance proteins, often referred to as the “deep proteome”, where potential biomarkers may be found [60]. As a result, differential proteomics of unfractionated plasma provides limited insight. To increase analysis sensitivity, various precipitation methods [61] and commercially available depletion/enrichment strategies have been developed. These methods either remove the most abundant proteins or enrich plasma for low-abundant ones, mainly using antibodies, ion exchange, or affinity methods [62]. However, all these protocols may cause nonspecific co-depletion of less abundant proteins to some extent.
Several serological markers have been identified as correlating with coronary artery disease (CAD), covering a wide spectrum of pathophysiological processes such as cardiomyocyte injury, inflammation, oxidative stress, hemostasis, lipid metabolism, cell/cell interactions, and renal function. These biomarkers, relevant to ACS, are summarized in Table 1.
High-throughput unbiased quantitative plasma proteomics has also been applied to the identification of subclinical atherosclerosis biomarkers. In particular, Núñez et al. [76] performed an impressive study with a discovery phase on 444 subjects, well characterized by imaging of major arterial roots (carotids, infrarenal abdominal aorta, and iliofemoral arteries), cardiac computed tomography, clinical and blood parameters, and an external validation on 350 subjects. The identified panel of three proteins (Ig alpha-2 chain C region, apolipoprotein(a), and haptoglobin), assessed by standard assays on a cohort of 2999 subjects, was proven to be significantly associated with subclinical atherosclerosis.
In recent years, proteomics of secretory vesicles, intraluminal thrombus, urine, and purified lipoprotein fractions (i.e., lipoproteomics) has gained increasing attention as an alternative to whole plasma analysis in the search for new cardiovascular biomarkers.
2.1. Proteomics of Secretory Vesicles
Cells release various types of secretory vesicles, including microparticles, exosomes, and apoptotic bodies, found in all body fluids. These vesicles play relevant roles in intercellular communication by transferring proteins, nucleic acids, lipids, and metabolites to target cells via specific membrane receptors, and consequently, they differ in biogenesis, size, cargo, and biological functions. Understanding their roles in various pathophysiological processes can provide valuable insights into disease mechanisms and be key to developing novel therapeutic strategies for conditions such as cancer and cardiovascular disorders. Furthermore, the circulating levels of these vesicles could serve as biomarkers to assess disease severity and monitor treatment responses.
Secretory vesicles are of particular interest in the context of atherosclerosis, as they are released by multiple cell types involved in plaque progression, such as endothelial cells, smooth muscle cells, lymphocytes, monocytes, erythrocytes, and platelets, in response to pro-inflammatory signals and environmental stimuli like shear stress, hypoxia, and oxidative stress. These vesicles play a role in several pro-atherogenic events, including endothelial dysfunction, thrombosis, regulation of vascular tone, and the promotion of interactions between monocytes and endothelium, leukocytes and leukocytes, and leukocytes and endothelium. This has been consistently reviewed in the literature [47,77,78,79].
2.2. Proteomics of Intraluminal Thrombus
The formation of an intraluminal thrombus, triggered by a ruptured or eroded plaque, is considered the primary event leading to impaired blood flow in the coronary arteries during AMI. However, the exact mechanisms behind the sudden occlusion of coronary arteries in AMI remain unclear.
In a differential proteomics analysis, Distelmaier K et al. compared systemic plasma with plasma collected from the site of thrombus formation in AMI patients. Using two-dimensional gel electrophoresis followed by LC–MS/MS, they discovered, for the first time, an accumulation of the complement activator C-reactive protein, as well as the downstream complement effectors C3a and C5a, at the site of coronary thrombus formation during AMI. This localized event was shown to amplify the acute vascular occlusion process by enhancing neutrophil recruitment into the thrombus [80].
Alonso-Orgaz et al. conducted the first proteomic analysis of thrombus samples obtained from patients with STEMI through percutaneous intracoronary thrombectomy during primary angioplasty. By employing both gel-based and gel-free proteomic techniques, they identified 708 proteins in the thrombus, including a panel of five proteins—fermitin homolog 3, thrombospondin-1, myosin-9, beta parvin, and ras-related protein Rap-1b—that were positively correlated with the platelet marker CD41. These findings suggest the potential activation of a focal adhesion pathway in the platelets present within the thrombus. Additionally, the protein death-inducer obliterator 1 was found to be elevated in the plasma of STEMI patients, highlighting its potential as a systemic biomarker for thrombosis [81].
2.3. Urine Proteomics
Urine is an easily accessible and stable body fluid that remains resistant to proteolytic degradation even after extended storage, making it a valuable source of information. The protein and peptide composition of urine results from glomerular filtration and proximal tubular absorption of circulating proteins (about 30%) and from the urogenital tract (approximately 70%) [82]. Since urinary proteins can originate from all organs, reflecting both local and systemic pathophysiological conditions, urine has become one of the most promising biofluids in clinical proteomics, with applications across a wide range of medical fields. However, the urinary proteome is highly influenced by inter-individual and intra-individual variability, the latter being affected by factors such as physical activity, diet, medications, and caffeine consumption [83].
Although research on the urinary proteome in relation to CAD is still in its early stages, significant progress has been made in recent years [84]. Using capillary electrophoresis coupled with micro time-of-flight mass spectrometry, Delles et al. reported a panel of 238 CAD-specific polypeptides with high diagnostic potential [85,86,87]. This panel reverted to a physiological state following two years of antihypertensive treatment, suggesting its potential utility in patient monitoring. In a subsequent well-controlled prospective study, the same team identified a subset of markers predictive of CAD outcomes, including extracellular matrix components and proteins involved in hemostasis, erythropoiesis, inflammation, immune response, and signaling [88].
2.4. Lipoproteomics
Lipoproteomics is a specialized field of proteomics that focuses on the comprehensive analysis of apolipoproteins and lipoprotein-associated proteins, examining their structural and functional characteristics. It also aims to identify novel biomarkers that can be used for risk assessment, diagnosis, and treatment of various pathological conditions, particularly CVD.
Lipoproteins are supramolecular complexes that transport insoluble lipids from their sites of synthesis to tissues involved in their metabolism or storage. These complexes typically feature a hydrophobic core composed mainly of triacylglycerols and cholesteryl esters. Surrounding this core, there is a shell composed of amphipathic compounds, including phospholipids, unesterified cholesterol, and proteins, which are referred to as apolipoproteins (apo) and lipoprotein-associated proteins [89]. The various lipoprotein species found in circulation differ in their chemical composition, physical properties, and metabolic functions, and have been historically classified based on their densities: chylomicrons (<0.95 g/mL), very low-density lipoproteins (VLDL, <1.006 g/mL), low-density lipoproteins (LDL, 1.019–1.063 g/mL), intermediate-density lipoproteins (IDL, 1.006–1.030 g/mL), and high-density lipoproteins (HDL, 1.063–1.21 g/mL) [90]. Lipoprotein(a) or Lp(a) is another distinct class of lipoproteins, which consists of an LDL particle bound to a large, highly polymorphic glycoprotein called apo(a), connected to apo B100 by a single disulfide bond [91]. Smaller isoforms of apo(a), containing 11–22 Kringle IV repeats, have been strongly linked to high Lp(a) levels and an increased risk of coronary heart disease [92].
Lipoproteins, especially LDL and HDL, are crucial in the development of CVD. LDL is the primary transporter of cholesterol to peripheral tissues and a well-established major risk factor for atherosclerosis [22]. According to the “response-to-retention” hypothesis, LDL is retained in the subendothelial space of the arterial wall through interactions with ECM components, initiating the process of atherogenesis [93]. Conversely, HDL offers vascular protection by removing excess cholesterol from cells and facilitating its transport to the liver through reverse cholesterol transport [94]. Additionally, the pleiotropic HDL exhibits antioxidant, anti-inflammatory, and anti-thrombotic properties [95] and appears to play a role in innate immunity [96].
Recent studies have highlighted the critical role of lipoproteins’ protein and lipid components in influencing their functions in health and disease, particularly in CVD. Understanding the detailed composition and structure of the cargo within each lipoprotein class could provide valuable insights into their involvement in atherogenesis and the development of atherosclerotic plaques. In this context, the method used to isolate different lipoprotein particles is crucial, as it can significantly impact their protein content [97]. Ultracentrifugation in high-salt media represents a widely used method, established in the 1950s [98]. An issue of this approach is represented by the high ionic strength of the medium and the high centrifugal field forces that might cause either the dissociation of proteins or their exchange between different lipoprotein classes, potentially altering the pattern of associated exchangeable apolipoproteins. Additionally, some protocols have been set up in which salts were partially substituted by compounds, such as sucrose, iodixanol, or deuterium oxide. In this respect, Stahlman et al. suggested that deuterium oxide should be preferred over salts for isolating both LDL and HDL [99]. Alternatively, lipoproteins can be isolated through immunopurification methods that rely on specific antibodies for the dominant protein of each class. Although this procedure does not lead to the loss of weakly associated proteins, it may copurify non-specifically associated proteins, such as serum contaminants and/or other lipoprotein fractions carrying the same antibody target (e.g., apolipoprotein A-I is the main HDL apolipoprotein, but it is also present in both VLDL and LDL fractions). Other lipoprotein isolation methods that have been applied in lipoproteomic studies involve electrophoretic techniques, specifically free solution isotachophoresis [100], and chromatographic techniques, such as fast protein liquid chromatography [101], and size exclusion/affinity chromatography [102,103].
Furthermore, factors such as the choice of analytical method (instrumentation, quantification, and statistical approaches) and sample heterogeneity contribute to the discrepancies observed across studies, complicating the identification of widely accepted biomarkers (Figure 5) [104].
Notably, Davidson and colleagues have made significant contributions by curating a comprehensive list of proteins found in HDL and LDL, ranked by the frequency of their identification in mass spectrometry studies. This updated list is freely available to the scientific community through their website (www.DavidsonLab.com). The “HDL Proteome Watch Database” includes 285 proteins identified as “likely” HDL proteins, based on reports from at least three different laboratories out of a total of 1030 proteins identified across 51 studies. Gene ontology analyses of these proteins revealed their involvement in various biological processes, including lipid transport, hemostasis/protease inhibition, inflammation/acute phase response, immunity/anti-microbial functions, and cell/heparin binding [104]. Similarly, the database lists 60 proteins identified in four LDL proteomics studies up to 2015, with 22 of these proteins categorized as “likely” LDL proteins, because of independently identified by at least two studies. These include apolipoproteins A-I, A-II, A-IV, B, C-I, C-II, C-III, C-IV, D, E, F, J, L1, M, (a), serum amyloid A1, A2, A4, albumin, alpha-1-antitrypsin, cathelicidin antimicrobial peptide, dermcidin, and fibrinogen alpha chain.
Only a limited number of studies have focused on the VLDL proteome [99,107,108,109,110,111,112]. Among these, Dashty et al. identified 95 VLDL-associated and 51 LDL-associated proteins, of which 39 were common to both, and 56 and 12 were unique to VLDL and LDL, respectively. This set included all known apolipoproteins, lipid transport proteins, coagulation proteins, complement system proteins, and anti-microbial proteins [113].
Limited data are available on the Lp(a) proteome. Von Zychlinski et al. used two-dimensional liquid chromatography coupled with tandem mass spectrometry on highly purified Lp(a) particles that underwent tryptic digestion, identifying 35 proteins with high confidence. These proteins were involved in two key biological processes: lipid metabolism and response to wounding, the latter encompassing coagulation, complement activation, and inflammatory responses [114]. Bourgeois and colleagues conducted a discovery analysis on both Lp(a) and LDL, identifying 154 associated proteins. A differential analysis between Lp(a) and LDL proteomes revealed 15 proteins preferentially associated with Lp(a), which may be implicated in the acute inflammatory response, extracellular structure organization, and protease inhibition [115]. More recently, Mueller et al. developed a method for isolating Lp(a) from very small volume plasma samples (0.4 mL), enabling in-depth mass spectrometry analysis and providing a valuable tool for proteomics in case of limited sample availability [116].
Over the past two decades, numerous proteomic studies of purified HDL fractions have been conducted in relation to CAD, AMI, and ACS (Table 2).
While proteomics has advanced our understanding of the functions of different lipoprotein classes, particularly in relation to CVD, more information is needed to assess the residual risk of acute clinical events. The pleiotropic functions of lipoproteins, especially HDL, are influenced by both their protein and lipid components. Alterations in any of these elements can result in dysfunctional lipoproteins with pro-inflammatory and pro-atherogenic properties [129].
Recent years have seen a surge of interest in plasma lipidomics, driven by compelling evidence linking specific lipid species to the development of atherosclerosis [53,130,131,132,133,134,135,136], as well as to the onset of adverse clinical events [54,137,138,139,140,141]. However, only a limited number of studies have explored the relationship between biologically active lipids, their lipoprotein carriers, and CVD, as also recently reviewed by Ding and Rexrode [142].
Some studies have identified changes in the HDL phospho- and sphingolipidomes in connection with various pathological conditions strongly associated with CVD, such as type 1 and type 2 diabetes [143,144,145], obesity and metabolic syndrome [146,147], dyslipidemia [148,149], carotid atherosclerosis [106], and experimental atherosclerosis [150,151]. Furthermore, treatments such as statins [152] and dietary interventions with phytosterols and omega-3 fatty acids [153] have been shown to induce changes in the LDL lipidome, leading to a reduction in cardiovascular risk.
Lipidome profiles of both HDL and LDL have been explored in relation to CAD and ACS [154,155,156,157], revealing distinct differences when compared to healthy controls. Notably, the HDL phosphosphingolipidome exhibited unique signatures in individuals with hyperalphalipoproteinemia, a rare condition marked by elevated plasma HDL-cholesterol levels and an increased risk of early CAD [158,159].
To gain a more comprehensive understanding of lipoprotein metabolism in relation to CVD, Wang and colleagues recently developed a high-resolution method to analyze both the proteome and lipidome of lipoproteins and their interconnections [55]. Their findings demonstrated that the combined proteomic and lipidomic data provided better differentiation between ACS patients and healthy individuals than either proteomics or lipidomics alone.
3. Dissecting Atherosclerotic Plaque Through Proteomics
While tissue analysis can provide valuable insights, studying human atherosclerotic plaque specimens presents considerable challenges. Atherosclerotic plaques are complex tissues composed of various cell types within an environment marked by inflammatory, proteolytic [28,29], and oxidative processes [30,31]. These plaques reflect a systemic condition shaped by prolonged exposure to genetic and environmental risk factors. In addition to vascular smooth muscle cells (SMCs) and endothelial cells, plaques contain inflammatory cells, plasma proteins, newly synthesized ECM components, cell debris from apoptotic or necrotic events, and end-products of lipid and protein oxidation [18,24,160].
One potential solution to this issue is laser-captured microdissection (LCM), which allows for the isolation of specific cells or regions of the plaque under direct microscopic visualization. This technique has been minimally explored in proteomics but holds great promise. Another critical aspect of in situ analysis is selecting an appropriate control. To reduce tissue variability, it is ideal to use control samples from the same vascular region of the patient. Additionally, specimens obtained from surgical endarterectomy are preferred over post-mortem samples to avoid degradation of tissue before analysis. A key limitation, however, is the availability of human specimens. Given the heterogeneity of advanced lesions—such as variations in fibrous cap thickness, inflammatory and proteolytic components, calcifications, surface erosion, thrombosis, and intraplaque hemorrhage—a careful histochemical classification before biochemical analysis is essential [161,162].
In recent years, various proteomic technologies have been applied to diseased human tissues, providing deeper insights into the molecular mechanisms underlying advanced atherosclerotic plaque development. These studies have also enabled the identification of diagnostic features associated with plaque instability, which may serve as valuable therapeutic targets or biomarkers for patient monitoring. Research has primarily focused on both plaque extracts and secretomes, with the latter being derived by culturing different types of plaque segments. Additionally, animal models have been employed to further investigate the mechanisms involved in the early stages of lesion formation.
3.1. Proteomics of Coronary Plaque Extracts
Since the early 2000s, approximately twenty proteomics studies on human atherosclerotic plaques have been conducted, with a primary focus on either coronary (Table 3) or carotid atherosclerosis [163]. Both in-gel electrophoresis and shotgun proteomics have been employed to identify differentially expressed proteins. However, some limitations of these studies include the relatively small sample sizes and the challenges in selecting appropriate controls, which are often derived from unaffected vascular regions of the same patient or from different individuals. As a result, topological and inter-individual differences may be overlooked. Additionally, comprehensive validation using an independent cohort and complementary methodologies is often lacking.
The first large-scale protein profile of human atherosclerotic coronary arteries was provided by Bagnato et al., who identified 806 unique proteins with high confidence [165]. They utilized the direct tissue proteomic (DTP) approach, a technique developed by Hwang et al. for identifying candidate markers from formalin-fixed paraffin-embedded cancer specimens [169], to analyze paraffin and frozen tissue blocks from 35 coronary atherosclerotic lesions, which were classified histopathologically into early, intermediate, and advanced stages. The researchers laser-microdissected different plaque areas from both paraffin and frozen sections and subjected them to tryptic digestion followed by LC-MS/MS for area-specific proteomic analysis. Additionally, they homogenized the frozen sections, resolved the extracted proteins via SDS-PAGE, and analyzed them by LC-MS/MS. To quantify Stromal Cell-derived Factor 1 α and growth factors, which were not detected by the previous methods, they employed the AQUA (absolute quantification) methodology. This study demonstrated that laser capture microdissection (LCM) applied to plaque proteomics is an effective tool for comparing different plaque areas, such as the necrotic core and fibrous cap, providing valuable spatial insights.
LCM was also utilized by de la Cuesta et al. to isolate the intimal layers from human atherosclerotic coronary arteries, as well as from pre-atherosclerotic coronary and radial arteries, which were subsequently analyzed using 2D-DIGE coupled with MALDI-TOF/TOF MS for protein identification [166]. Their analysis revealed altered expression of 13 proteins involved in critical processes of plaque development, including vascular smooth muscle cell (VSMC) migration, ECM composition, coagulation, apoptosis, heat shock response, and intraplaque hemorrhage deposition.
In an effort to identify novel markers of plaque disruption, Lee et al. performed proteomic analysis on plaque debris obtained during coronary angioplasty using filterwire devices, identifying 423 proteins. The control group consisted of patients who underwent angiography without stenting [167]. They found that matrix metalloproteinase-9 (MMP-9) was significantly increased in lipid-rich plaques, as well as in the plasma of patients after plaque disruption by stenting. This novel method offers promising potential for discovering circulating biomarkers of plaque erosion, which is a key pathological mechanism behind major acute clinical events.
Although atherosclerosis often remains asymptomatic for many years, early lesions can manifest in children and young adults. Identifying arterial protein networks and their changes during the early stages of atherosclerosis holds great promise for diagnostics and therapy, with potential implications for preventing acute clinical events. In this context, Herrington et al. conducted a study to explore features of early atherosclerosis by examining 200 coronary and aortic autopsy samples from young adults. This approach led to the identification of 1925 proteins, as well as several networks and pathways associated with early atherosclerosis. Based on these findings, they selected a set of 13 plasma proteins, which were later shown to be effective in predicting the onset of CAD in an independent clinical cohort [33].
3.2. Proteomics of Plaque Secretomes
The plaque secretome may serve as another valuable source of biomarkers with potential clinical applications. It encompasses the full spectrum of proteins released or secreted into a serum-free medium by the plaque during culture. As such, the secretome is expected to reflect tissue-specific metabolic functions and changes in both healthy and diseased states. In comparison to tissue extracts and plasma samples, the secretome typically contains fewer protein species and exhibits a more limited range of protein concentrations.
Proteomics applied to the study of the cultured plaque secretome was initially pioneered by the teams of Vivanco and Egido, and this approach has since been successfully adopted in several studies [163]. The method developed by Duran et al. enabled the analysis of secretomes from different regions of the same carotid specimens obtained through endarterectomy (including normal segments, non-complicated plaques, and plaques complicated by thrombus). This approach helped mitigate intra- and inter-individual variability in control specimens by using 2D electrophoresis coupled with mass spectrometry [170]. Martin–Ventura and colleagues applied this technique to analyze protein secretion profiles from both femoral and carotid plaques, identifying Heat Shock Protein 27 as a potential circulating marker for atherosclerosis [171]. Notably, this method also proved valuable in assessing the effects of pharmacological treatments on plaque. In fact, the same team found that incubating plaque specimens with atorvastatin caused the expression of 66% of the proteins to revert to their baseline control levels [172].
De la Cuesta et al. conducted LC-MS/MS analysis on secretomes from human atherosclerotic coronary arteries, pre-atherosclerotic coronary arteries, and mammary arteries, identifying 64 proteins, 15 of which had not been previously reported in plasma. Due to the reduced dynamic range of protein concentrations in the secretome, they were able to identify low-abundance proteins such as laminin A/C, GELS, and vinculin, which are known to be involved in inflammation, cell adhesion, and arterial aging. These proteins were found to be significantly dysregulated in the coronary plaque secretome compared to the mammary artery secretome, suggesting potential therapeutic implications [173].
Secretome proteomics has also been applied to study coronary plaques in pigs fed a standard or high-cholesterol diet. This model, which closely mimics human pathology, offers valuable insights into the molecular mechanisms driving early atherogenesis, a stage that is challenging to study in human clinical settings. The early stages of plaque development are particularly difficult to examine in humans, but using a systems biology approach that integrates secretome data with histopathological features and circulating factors, Pelosi et al. demonstrated that systemic inflammation was locally associated with macrophage/phagocytosis-related protein expression in arteries, influencing atherosclerosis severity [51].
Rocchiccioli et al. mapped 224 proteins secreted by coronary plaques cultured from the same pig model used by Pelosi, finding a strong correlation between VSMC activation/migration and lesion progression [52]. Among the differentially expressed proteins associated with various stages of atherosclerosis (from type I to type V, according to Stary’s classification), chitinase 3-like protein 1 was identified, and its expression was validated through immunohistochemistry. This protein was proposed as a potential diagnostic marker for atherosclerosis.
4. Conclusions
The continuous discovery and understanding of new biomarkers for atherosclerosis hold the potential to significantly improve our ability to predict future cardiovascular risks, particularly when emerging biomarkers are integrated with traditional risk factors to assess overall risk profiles.
In recent years, proteomics has become a powerful tool in identifying novel cardiovascular biomarkers with diagnostic and prognostic significance. This approach offers an unparalleled opportunity to deepen our understanding of the various stages of atherogenesis and plaque development, bridging the gap between fundamental research and clinical applications. Plasma and plasma-derived fractions, as well as atherosclerotic tissues—especially plaque extracts and secretomes—are invaluable sources of information about both the early stages of atherogenesis and potential predictors of acute clinical events.
Despite its promise, advancing proteomics toward clinical practice faces several challenges. These include the intrinsic complexity of biological matrices, issues with sample availability, and the selection of appropriate controls, all of which can hinder results interpretation. Large-scale studies across different populations are needed to validate the clinical relevance of newly identified biomarkers, as well as the development of cost-effective standardized assays. While many databases exist that collect findings from genome-wide association studies and gene expression profiling, there is currently no proteomics-specific dataset dedicated to atherosclerosis. Therefore, future efforts must focus on thoroughly analyzing the wealth of data generated by proteomics studies to create comprehensive, shared datasets that include all identified biomarkers. These datasets should be integrated with data from other omics technologies, such as genomics, transcriptomics, and metabolomics. In this regard, artificial intelligence could play a crucial role in data analysis and interpretation, enabling fast, iterative processing of large volumes of information derived from these technologies. As technology advances and bioinformatics tools mature, proteomics is expected to play an increasingly pivotal role in precision cardiovascular medicine.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Roth G.A. Mensah G.A. Johnson C.O. Addolorato G. Ammirati E. Baddour L.M. Barengo N.C. Beaton A.Z. Benjamin E.J. Benziger C.P. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study J. Am. Coll. Cardiol.2020762982302110.1016/j.jacc.2020.11.01033309175 PMC 7755038 · doi ↗ · pubmed ↗
- 2Fahed A.C. Jang I.-K. Plaque Erosion and Acute Coronary Syndromes: Phenotype, Molecular Characteristics and Future Directions Nat. Rev. Cardiol.20211872473410.1038/s 41569-021-00542-333953381 · doi ↗ · pubmed ↗
- 3Byrne R.A. Rossello X. Coughlan J.J. Barbato E. Berry C. Chieffo A. Claeys M.J. Dan G.-A. Dweck M.R. Galbraith M. 2023 ESC Guidelines for the Management of Acute Coronary Syndromes Eur. Heart J. Acute Cardiovasc. Care 2024135516110.1093/ehjacc/zuad 10737740496 · doi ↗ · pubmed ↗
- 4Almeida I. Chin J. Santos H. Miranda H. Santos M. SáC. Almeida S. Sousa C. Almeida L. National Cardiology Data Collection Center, P.S. of C.C.P.N.R. of A.C.S.I. Prognostic Value of Brain Natriuretic Peptide in ST-Elevation Myocardial Infarction Patients: A Portuguese Registry Rev. Port. Cardiol.202241879510.1016/j.repc.2020.12.01636062710 · doi ↗ · pubmed ↗
- 5Ikeda S. Shinohara K. Enzan N. Matsushima S. Tohyama T. Funakoshi K. Kishimoto J. Itoh H. Komuro I. Tsutsui H. Serial Measurement of B-Type Natriuretic Peptide and Future Cardiovascular Events in Patients with Type 2 Diabetes Mellitus without Known Cardiovascular Disease Int. J. Cardiol.20223569810410.1016/j.ijcard.2022.03.04935354080 · doi ↗ · pubmed ↗
- 6Kamath D.Y. Xavier D. Sigamani A. Pais P. High Sensitivity C-Reactive Protein (Hs CRP) & Cardiovascular Disease: An Indian Perspective Indian J. Med. Res.201514226126810.4103/0971-5916.16658226458341 PMC 4669860 · doi ↗ · pubmed ↗
- 7Polyakova E.A. Mikhaylov E.N. The Prognostic Role of High-Sensitivity C-Reactive Protein in Patients with Acute Myocardial Infarction J. Geriatr. Cardiol.20201737938310.11909/j.issn.1671-5411.2020.07.00732863819 PMC 7416062 · doi ↗ · pubmed ↗
- 8Lee H.S. Lee J.-H. Early Elevation of High-Sensitivity C-Reactive Protein as a Predictor for Cardiovascular Disease Incidence and All-Cause Mortality: A Landmark Analysis Sci. Rep.2023131411810.1038/s 41598-023-41081-w 37644061 PMC 10465521 · doi ↗ · pubmed ↗