Adult-Onset Immunoglobulin A Vasculitis (IgAV) Presenting in a Middle-Aged Indian Male Patient
Abdalla Khalil, Naomi Oldham, Saju Beepaul, Elvin Chang

TL;DR
A middle-aged Indian man was diagnosed with adult-onset IgA vasculitis after showing symptoms like chest pain, abdominal pain, and rash.
Contribution
This case highlights IgAV in an adult male, which is less commonly reported than in children.
Findings
The patient showed elevated IgA levels and IgA deposition confirmed by skin biopsy.
He responded well to oral steroids with reduced inflammation.
The case demonstrates gastrointestinal and skin involvement typical of IgAV.
Abstract
Immunoglobulin A vasculitis (IgAV) is a small vessel vasculitis that mainly affects the skin, gastrointestinal tract, and kidneys. We present a case of a middle-aged male patient who presented to the emergency department with lower chest pain, colicky abdominal pain, and painful petechial rash. His inflammatory markers and IgA were raised with mild proteinuria. Abdominal CT and endoscopy revealed gastrointestinal involvement, and immunofluorescence skin biopsy confirmed IgA deposition in the dermal vessels. He responded clinically to oral steroids, and his inflammatory markers trended down. After six days, he was discharged.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1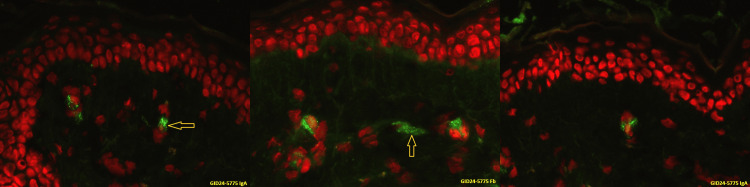 Figure 2
Figure 2 Figure 3
Figure 3| Test | Result on admission | Normal level |
| White blood count | 14.9 X10 ^9/L | 3.6 - 11 X10^9/L |
| Hemoglobin | 122 g/L | 130 – 180 X10^9/L |
| Platelet count | 542 X10^9/L | 140 - 400 X10^9/L |
| Neutrophils | 11.5 x10^9/L | 1.8 - 7.5 X10^9/L |
| Sodium | 136 mmo/L | 135 – 145 mmol/L |
| Potassium | 4.7 mmol/L | 3.5 – 5.1 mmol/L |
| Creatinine | 73 umol/L | 66 – 110 umol/L |
| ALT | 90 IU/L | 5-40 IU/L |
| ALP | 195 IU/L | 30 -120 mg/dl |
| Bilirubin | 14 umol/L | 3-20 umol/L |
| Albumin | 42 g/L | 35-55 g/L |
| CRP | 203 mg/dl | 0 – 5 mg/dl |
| ESR | 116 mm/hr | 0-20 mm/hr |
| IgA | 4.29 g/L | 0.8 -3.0 g/L |
| Complement C3 | 1.63 g/L | 0.75 – 1.75 g/L |
| Complement C4 | 0.36 g/L | 0.20 - 0.4 g/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Coagulation, Bradykinin, Polyphosphates, and Angioedema · Platelet Disorders and Treatments
Introduction
Immunoglobulin A vasculitis (IgAV), formerly known as Hench-Schonlein purpura, is a small vessel vasculitis characterized by the deposition of the dominant IgA1 immune complexes in the vessels of the target organs (predominantly capillaries, venules, and arterioles) [1].
Common clinical presentations include palpable purpura and petechiae (with a normal platelet count), arthralgia/arthritis, and gastrointestinal and renal involvement [2].
IgA vasculitis is the most common childhood primary vasculitis, but it is rare in adulthood [3]. The most common reported clinical presentation at onset in adults was non-thrombocytopenic purpura (97%), and the second most common presentation in adults was renal involvement (78%). Joint involvement was the third most common presentation (59%), followed by gastrointestinal involvement (39%) [3].
Many patients report infections preceding the onset of the symptoms of vasculitis (Streptococcus, parainfluenza, and human parvovirus B19), which are thought to trigger the disease. However, the full pathophysiology is not understood [4].
Case presentation
A 57-year-old Indian male patient programmer with a past medical history of mild ankylosing spondylitis and suspected Raynaud’s disease presented to the Accident and Emergency (A&E) with a four-day history of sudden onset, sharp pleuritic left lower chest/subcostal pain.
He was found to be tachycardic at 121 beats/minute, with an ECG showing normal sinus rhythm and no ST changes. The rest of the blood tests were normal.
He was referred to an ambulatory clinic via the pulmonary embolism pathway, where CT Pulmonary angiography demonstrated no pulmonary embolism and normal lung parenchyma.
Three days later, he presented to A&E complaining of diffuse cramping abdominal pain, ongoing chest pain, and progressive painful and itchy bilateral rash on both legs, which started on his buttocks and spread over his legs and up to mid-back.
The patient did not report any recent fever, respiratory symptoms, cough, cold, or previous rashes. He has not traveled abroad recently and has had no contact with ill individuals.
On examination, his heart rate was 110 beats/min, blood pressure was 126/70 mm Hg, temperature was 37 °C, respiratory rate was 20/min, and oxygen saturation was 97%. He had a widespread, tender, itchy petechial rash over the upper arms, back, abdomen, flanks, buttocks, and inner thighs (Figure 1).
Rash type and distribution Widespread petechial rash at the arm, cubital area, buttock, flank, and back of the patient.
His chest was clear on auscultation, and his heart examination was normal. Abdominal examination revealed generalized tenderness without guarding or rebound and normal bowel sounds. He had bilateral ankle mild pitting edema.
Blood tests on admission revealed high WBC, neutrophils, ESR, and CRP. Immunoglobulin A was raised too (Table 1).
An autoimmune screen was sent, including antineutrophil cytoplasmic antibodies (ANCA), antinuclear antibody (ANA), anti-double-stranded DNA (dsDNA), anti-RO, anti-Sm, complements, immunoglobulins, and rheumatoid factor, which were all negative apart from IgA.
His blood and urine cultures were negative, and his viral screen for COVID-19, flu, Epstein-Barr virus (EBV), cytomegalovirus (CMV), hepatitis B virus (HBV), hepatitis C virus (HCV), and HIV were all negative. His urine microscopy was normal, but the urine albumin creatinine ratio was mildly raised to 4.9 mg/mmol (<3 mg/mmol).
He was commenced on IV piperacillin/tazobactam to cover a possible abdominal infection. Following dermatology consultation, a provisional diagnosis of IgA vasculitis was made, and he was also commenced on oral prednisolone 30 mg once daily with a weaning course of 5 mg every five days.
His abdominal and chest pain improved, and his infection markers decreased. His ECG demonstrated normal sinus rhythm and no ST changes. A bedside ECHO demonstrated no pericardial effusion, normal systolic and diastolic function, and normal valves and pulmonary artery pressure.
A skin biopsy (from a recent rash on the back of the patient) was performed before his discharge, and immunofluorescence imaging showed IgA deposition in the subdermal vessels (Figure 2).
Immunofluorescence image of the skin biopsy. The IgA and fibrinogen are the granular fluorescent green colour in the dermal vessels (Yellow arrows)
Oesophago-gastro duodenoscopy revealed erosive gastritis and duodenitis, which was felt likely secondary to vasculitis.
CT abdomen and pelvis with intravenous contrast demonstrated a short segment of enteritis involving the proximal jejunum with a further focal area of fat stranding and a small volume of free fluid surrounding the cecum, suggestive of cecum inflammation. Multifocal areas of inflammation involving the small and large bowel were felt secondary to the recent diagnosis of vasculitis (Figure 3).
CT Abdomen and Pelvis with IV Contrast. Axial and Coronal view showing short segment of enteritis involving the proximal jejunum (left horizontal arrow). The focal area of fat stranding and small volume of free fluid surrounding the cecum suggests cecum inflammation/caecitis (right lower vertical arrow). Those areas of bowel inflammation may be secondary to the recent diagnosis of vasculitis.
His abdominal and chest pain resolved, and his inflammatory markers were down-trending. He was discharged after six days with an outpatient follow-up with rheumatology, gastroenterology, and renal clinic.
Discussion
The annual incidence of adult IgAV vasculitis varies among countries. It was reported at 6.21-20.4/100,000 in the UK, 6.1/100,000 in the Netherlands, 17.55/100,000 in southern Sweden, 12.9/100,000 in Taiwan, and 55.9/100,000 in Korea [3,5,6].
The disease is mostly mild and self-limiting when presenting in childhood, but it is more likely to follow a remission and relapsing course in adult IgA vasculitis [7,8].
In a French multicenter retrospective study of 260 adult patients with IgAV, 53% had gastrointestinal involvement. The most common initial presentation was abdominal pain 99%, intestinal bleeding was 31%, diarrhea was 26%, and surgical abdomen was 4%, and the most common finding at abdominal imaging was intestinal wall thickening 63%. The endoscopic abnormalities were 87%, mostly mucosal ulceration [9].
The European League Against Rheumatism/Pediatric Rheumatology International Trials Organization/Pediatric Rheumatology European Society (EULAR/PRINTO/PRES) published the classification criteria of IgA vasculitis in 2010. This was more sensitive and specific in the adult population than the old American College of Rheumatology criteria published in 1990. EULAR/PRINTO/PRES criteria for diagnosis of IgAV include purpura or petechiae and one of the following four criteria (abdominal pain, arthritis/arthralgia, renal involvement, and leukocytoclastic vasculitis with predominant IgA deposits or proliferative glomerulonephritis with predominant IgA deposits) [10].
In a recent retrospective study in Sweden of adults with IgAV from 2000 through 2019, the most common clinical presentation at onset was non-thrombocytopenic purpura (97%), renal involvement (78%), primarily mild, consisting of microscopic haematuria and non-nephrotic proteinuria. IgAV in adults frequently affects the kidneys and causes chronic kidney disease, but has a favorable outcome than other vasculitides affecting the kidneys [11].
Our patient presented with palpable petechial rash, abdominal pain, and gastrointestinal and renal involvement. His inflammatory markers and serum IgA were raised. His abdominal CT showed enteritis of the proximal part of the jejunum and inflammation of the caecum. His immunofluorescent image of the skin biopsy confirmed IgA deposition in the subdermal venules.
Rarely, a patient with ankylosing spondylitis can develop leucocytoclastic vasculitis, which is another small vessel vasculitis, but no other organ is involved as in our patient.
Conclusions
IgAV is a relatively rare disease in adults compared to children. Abdominal pain is one of the common presentations of IgAV which requires medical imaging and endoscopy to exclude other differential diagnoses and to assess the gastrointestinal involvement. Mild proteinuria may be the early renal involvement. Predominant IgA deposition in the dermal vessels is also a confirmatory finding.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pathogenesis of Ig A vasculitis: an up-to-date review Front Immunol Song Y Huang X Yu G Qiao J Cheng J Wu J Chen J 7716191220213485842910.3389/fimmu.2021.771619 PMC 8630619 · doi ↗ · pubmed ↗
- 2Overview of the 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides Clin Exp Nephrol Jennette JC 6036061720132407241610.1007/s 10157-013-0869-6PMC 4029362 · doi ↗ · pubmed ↗
- 3Epidemiology of primary systemic vasculitis in children: a population-based study from southern Sweden Scand J Rheumatol Mossberg M Segelmark M Kahn R Englund M Mohammad AJ 2953024720182940937310.1080/03009742.2017.1412497 · doi ↗ · pubmed ↗
- 4Viral infections may be associated with Henoch-Schönlein purpura J Clin Med Nikolaishvili M Pazhava A Di Lernia V 12202310.3390/jcm 12020697 PMC 986200936675626 · doi ↗ · pubmed ↗
- 5A nationwide survey on epidemiological characteristics of childhood Henoch-Schönlein purpura in Taiwan Rheumatology (Oxford) Yang YH Hung CF Hsu CR Wang LC Chuang YH Lin YT Chiang BL 6186224420051567105010.1093/rheumatology/keh 544 · doi ↗ · pubmed ↗
- 6Epidemiology of immunoglobulin A vasculitis (Henoch-Schönlein): current state of knowledge Curr Opin Rheumatol Piram M Mahr A 1711782520132331873510.1097/BOR.0b 013e 32835 d 8e 2a · doi ↗ · pubmed ↗
- 7Henoch-Schönlein purpura in children and adults: clinical differences in a defined population Semin Arthritis Rheum García-Porrúa C Calviño MC Llorca J Couselo JM González-Gay MA 1491563220021252807910.1053/sarh.2002.33980 · doi ↗ · pubmed ↗
- 8Differences in clinical manifestations and outcomes between adult and child patients with Henoch-Schönlein purpura J Korean Med Sci Kang Y Park JS Ha YJ 1982032920142455064510.3346/jkms.2014.29.2.198PMC 3923997 · doi ↗ · pubmed ↗