Mitral Valve Aneurysm With Severe Mitral Regurgitation and Pseudoaneurysm Formation: A Rare Complication of Infective Endocarditis
Kesar Prajapati, FNU Samaksh, Poornima Jaiswal Charpuria, Nisarg Desai, Ankit V Shah

TL;DR
A rare case of infective endocarditis leading to a mitral valve aneurysm and severe heart failure is reported, highlighting the need for early diagnosis and treatment.
Contribution
This paper presents a rare clinical case of mitral valve aneurysm as a complication of infective endocarditis with fatal outcomes due to delayed diagnosis.
Findings
A 34-year-old female with infective endocarditis developed a mitral valve aneurysm and pseudoaneurysm, leading to severe heart failure.
Delayed diagnosis and advanced presentation resulted in refractory heart failure and electrical storm, causing a fatal outcome.
The case emphasizes the importance of early recognition and timely surgical intervention for improved prognosis.
Abstract
Infective endocarditis (IE) is a life-threatening condition caused by infection of the heart’s endocardial surface, often involving native or prosthetic valves. It presents with diverse symptoms, ranging from isolated fever and heart failure to more severe manifestations such as ischemic stroke from septic or thrombus embolization. A rare but serious complication of IE is mitral valve aneurysm (MVA), a localized outpouching of the mitral valve, often leading to mitral regurgitation (MR), heart failure, and, in severe cases, rupture. This report highlights a case of delayed diagnosis of IE in a 34-year-old female who presented with prolonged fever, progressive dyspnea, and signs of heart failure. Echocardiography revealed severe MR, anterior mitral valve leaflet perforation, and a large pseudoaneurysm, suggesting MVA. Because of the advanced presentation, the patient developed refractory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
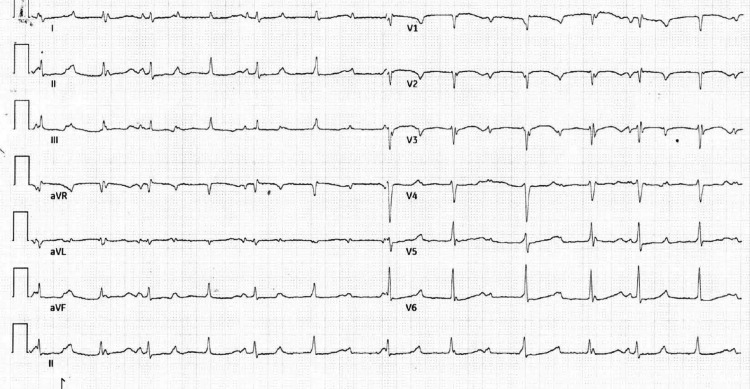 Figure 1
Figure 1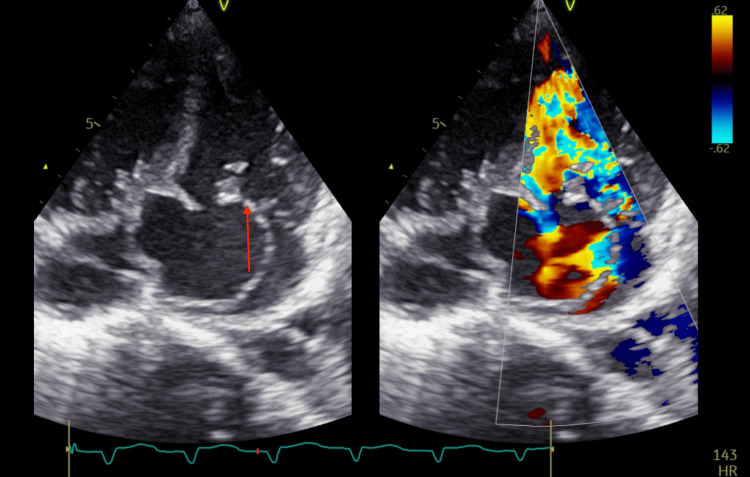 Figure 2
Figure 2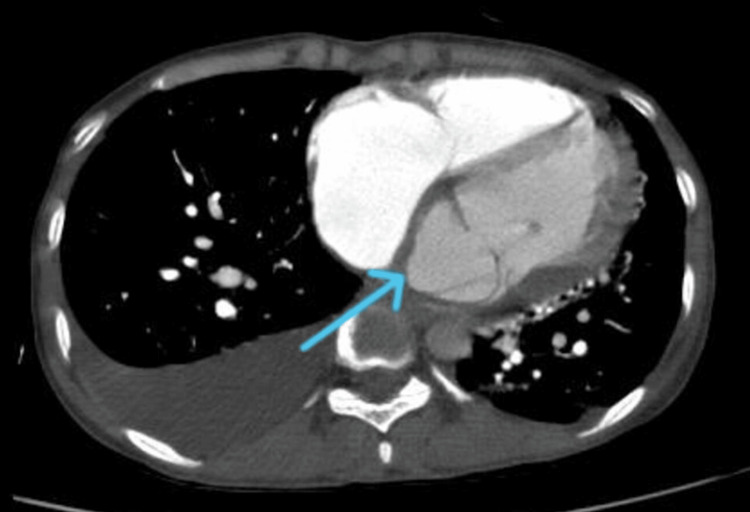 Figure 3
Figure 3 Figure 4
Figure 4| Laboratory parameters | Patient value | Reference range |
| WBC | 20,000/mm3 | 4.30-11.0 mm3 |
| Neutrophil | 80% | 50-65% |
| Lymphocytes | 18% | 25-40% |
| Hemoglobin | 8.5 g/dL | 14-18 g/dL |
| MCV | 86.2 fL | 80-94 fL |
| MCH | 27.3 pg | 26-33 pg |
| MCHC | 31.6 g/dL | 31-36 g/dL |
| BUN | 25 mg/dL | 6-20 mg/dL |
| Creatinine | 1.2 mg/dL | 0.7-1.2 mg/dL |
| Sodium | 135 mEq/L | 136-145 mEq/L |
| Potassium | 4.5 mEq/L | 3.5-5.1 mEq/L |
| Magnesium | 2.2 mg/dL | 1.6-2.6 mg/dL |
| Phosphorus | 3.3 mg/dL | 2.5-4.5 mg/dL |
| Troponin | 13 ng/L | 0-22 ng/L |
| Pro-BNP | 1200 pg/mL | 1-125 pg/mL |
| Procalcitonin | 100.2 ng/mL | 0.02-0.08 ng/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Structural Anomalies and Repair · Cardiac Valve Diseases and Treatments
Introduction
Infective endocarditis (IE) is an infection of the heart's endocardial surface, affecting both native valves and prosthetic materials like artificial valves, pacemakers, and catheters. Despite diagnostic and therapeutic advances, IE remains a life-threatening disease with diverse presentation, varying from patients presenting with isolated fevers and decompensated heart failure to patients presenting with hemorrhagic or ischemic stroke resulting from either septic or thrombus embolization [1]. Complications of valvular IE include abscesses, fistulas, thromboembolism, septic embolization, and congestive heart failure from conduction system involvement and valve destruction [2]. Mitral valve aneurysm (MVA) formation was described as early as 1729 by Morand [3]. Transesophageal echocardiography (TEE) is particularly effective in identifying these aneurysms, which appear as saccular outpouchings of the mitral valve leaflets [4]. The integration of echocardiography and CT in the diagnostic workflow enhances the detection and management of IE complications, including MVA formation and rupture, thereby improving patient outcomes [5,6]. Aneurysm rupture in a longstanding MVA can lead to communication with the left atrium (LA), causing mitral regurgitation (MR), and the acute volume overload on the left ventricle (LV) and LA results in pulmonary edema and cardiogenic shock, which can be life-threatening [6,7]. Beyond MR, the rupture can also cause systemic embolization if thrombi are present within the aneurysm, further complicating the clinical picture [4]. Early diagnosis and treatment of IE are crucial to prevent severe complications [8]. We report a case of delayed recognition of IE that resulted in a rare but severe complication of ruptured MVA, causing MR, which resulted in the death of our patient.
Case presentation
A 34-year-old female patient was admitted to our hospital for prolonged high-grade intermittent fever for three months and worsening breathlessness gradually for two months, from New York Heart Association (NYHA) class II to class IV, along with constitutional symptoms like anorexia, weight loss, and fatigue. No significant past medical history was present, including major cardiovascular conditions. No major risk factors for IE were noted, like IV drug use, cardiac surgery, or congenital heart conditions. Multiple prescriptions of amoxicillin-clavulanic, levofloxacin, and sulfamethoxazole-trimethoprim were given for fever, but the patient never completed the treatment, as per the history. On presentation, her vital signs were as follows: blood pressure (BP) of 100/60 mmHg, heart rate (HR) of 50/minute, respiratory rate (RR) of 18/minute, and oxygen saturation of 95% on room air. Physical examination revealed anemia and mild splenomegaly. Cardiac examination showed a gallop rhythm, a wide split-second heart sound (S2), and a grade III/VI pansystolic murmur at the apex, suggesting severe MR.
A 12-lead electrocardiogram (ECG) revealed a junctional rhythm with intermittent complete heart block (CHB) (Figure 1). Inflammatory markers were elevated, with a total leukocyte count of 20,000/mm³ (80% neutrophils, 18% lymphocytes), an erythrocyte sedimentation rate (ESR) of 80 mm/hour, and a C-reactive protein (CRP) level of 200 mg/L. Additional laboratory values on admission included: hemoglobin 8.5 g/dL, troponin 13 ng/L, pro-BNP 1200 pg/mL, procalcitonin 50 ng/mL, blood urea nitrogen (BUN) 25 mg/dL, creatinine 1.2 mg/dL, sodium 135 mEq/L, potassium 4.5 mEq/L, magnesium 2.2 mg/dL, and phosphorus 3.3 mg/dL (Table 1). Blood cultures were performed but remained negative, likely due to prior antibiotic use before admission. This may have also contributed to the absence of visible vegetation on imaging. A 2D transthoracic echocardiogram (TTE) suggested anterior mitral valve leaflet perforation with severe MR. Additionally, a large subaortic aneurysm arose from the LV and prolapsed into the LA (Figure 2, Video 1). However, there was no evidence of intracardiac vegetation. Cardiac computed tomography revealed a large 40 × 29 mm pseudo-aneurysm arising from the basal segments of LV (Figure 3), involving the aorto-mitral region and projecting into the interatrial septum (IAS) and posterior atrioventricular groove the detailed anatomical information provided by cardiac CT is invaluable for planning the surgical intervention, ensuring that all infected and compromised tissues are addressed, and minimizing the risk of complications during and after surgery. As per the cardiothoracic surgery team, these CT findings may cause significant challenges for surgical planning, as they increase the risk of fistula formation and extensive tissue destruction.
12-lead electrocardiogram (ECG) with junctional rhythm with intermittent complete heart block (CHB)
Transthoracic echocardiography showing anterior mitral leaflet perforation (red arrow) with severe mitral regurgitation demonstrated on color Doppler
Transthoracic echocardiogram demonstrating anterior mitral leaflet perforation with severe mitral regurgitation on color Doppler
Axial contrast-enhanced cardiac CT image of the chest showing a large 40 × 29 mm pseudo-aneurysm (blue arrow) arising from the basal segments of the left ventricle
Treatment
Considering a clinical suspicion of IE, she was treated with intravenous antibiotics, along with a diuretic and non-invasive ventilation. She was scheduled for early mitral valve replacement (MVR) with pseudoaneurysm repair. However, during the hospital stay, she developed an electrical storm (Figure 4) with multiple episodes of ventricular tachycardia, which was managed with electrical cardioversion, intravenous amiodarone infusion, and overdrive pacing. However, the episodes were only partially responsive, likely due to the underlying severe structural and hemodynamic compromise. Temporary pacing was also attempted to stabilize the HR, but the patient’s condition remained unstable. A multidisciplinary team aimed to stabilize her for definitive surgical intervention. However, she had refractory heart failure precipitated by the electrical storm and succumbed before she could undergo surgical intervention.
Electrocardiogram showing an electrical storm with recurrent episodes of polymorphic ventricular tachycardia
Discussion
MVA is a rare but potentially life-threatening condition that involves the formation of a localized bulge or outpouching in the mitral valve leaflet, with the anterior valve leaflet more commonly involved than the posterior leaflet [9]. The mechanism behind MVA formation is believed to be related to inflammatory processes, causing the valve tissue to weaken and leading to the ballooning of the valve leaflet. This may be induced by endocarditis, rheumatic disease, and other connective tissue diseases like mitral valve prolapse, osteogenesis imperfecta, Marfan syndrome, and pseudoxanthoma elasticum [10]. MVAs present with symptoms of severe MR, including heart failure, dyspnea, and fatigue, similar to the presentation in this case. Auscultatory findings, such as a pansystolic murmur, are typical and reflect the regurgitant flow due to valve dysfunction [11]. The condition often leads to complications such as valvular perforation, rupture, or formation of a pseudoaneurysm, which can severely impair cardiac function and worsen heart failure [12]. Echocardiography is the primary diagnostic tool, revealing the aneurysmal bulge in the mitral leaflet and often showing associated MR [13].
MVAs present significant complications, including the risk of rupture and valvular perforation. While a conservative approach with serial follow-up is often recommended for uncomplicated MVA, when complications such as rupture or severe regurgitation arise, especially in large unruptured aneurysms, surgical intervention becomes necessary [14]. The 2020 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines outline medical and surgical approaches for managing MVAs [6]. Medical management includes antibiotic therapy for MVAs associated with IE to treat the underlying infection and prevent complications. Surgical options depend on the aneurysm's size and valve anatomy. Mitral valve repair is preferred for small aneurysms with favorable anatomy, while MVR is recommended for large unruptured aneurysms, particularly in cases of rupture, severe regurgitation, or when repair durability is uncertain. The guidelines emphasize surgical intervention for symptomatic patients with severe primary MR, irrespective of left ventricular systolic function, and favor MVR in complex cases to ensure durable outcomes. Recent studies support these recommendations, highlighting the importance of surgical management in severe mitral valve pathology [14,15].
In this case, the patient presented with high-grade fever, progressive dyspnea, and signs of heart failure (NYHA classes II to IV), which are typical of severe MR and IE. The echocardiogram showed anterior mitral valve leaflet perforation with severe MR, which is suggestive of an MVA or severe valvular damage. Moreover, the presence of a large pseudoaneurysm arising from the basal segments of the LV further supports the diagnosis of a complex MVA with associated complications, such as pseudoaneurysm formation [14]. The patient's refractory heart failure, despite medical management and antibiotic therapy, is a common outcome in cases of MVA with IE. Surgical intervention, such as MVR and aneurysm repair, is often required, but the presence of an electrical storm and ventricular tachycardia in this patient complicated the clinical course, preventing surgery and leading to a fatal outcome.
Conclusions
MVAs are a rare but serious complication, often associated with IE, present like MR clinically, and may occur as an isolated pathology. Early diagnosis through echocardiography is crucial. Surgical replacement remains the treatment of choice for patients with severe MR and aneurysm, but the presence of electrical storm and arrhythmias complicates management, as demonstrated in this case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study Arch Intern Med Murdoch DR Corey GR Hoen B 46347316920091927377610.1001/archinternmed.2008.603PMC 3625651 · doi ↗ · pubmed ↗
- 2Native-valve infective endocarditis N Engl J Med Chambers HF Bayer AS 56757638320203275752510.1056/NEJ Mcp 2000400 · doi ↗ · pubmed ↗
- 3A perforated mitral valve aneurysm: a rare but serious complication of aortic valve endocarditis resulting from a regurgitant jet lesion Cureus Werner ME Riezebos RK Kuipers RS 012202010.7759/cureus.11644 PMC 775566333376655 · doi ↗ · pubmed ↗
- 4Infective endocarditis complicated by mitral valve aneurysm: pathologic and echocardiographic correlations Echocardiography Seratnahaei A Bailey AL Hensley PJ O'Connor W Smith MD 141714223220152593097010.1111/echo.12958 · doi ↗ · pubmed ↗
- 5The role of echocardiography and cardiac computed tomography in the diagnosis of infective endocarditis J Clin Med Petkovic A Menkovic N Petrovic O 1212202310.3390/jcm 12175482 PMC 1048886537685577 · doi ↗ · pubmed ↗
- 62020 ACC/AHA guideline for the management of patients with valvular heart disease: Executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation Otto CM Nishimura RA Bonow RO 071143202110.1161/CIR.000000000000093233332149 · doi ↗ · pubmed ↗
- 7Ruptured mitral valve aneurysm: an uncommon cause of acute dyspnoea Echocardiography Tewari S Moorthy N Sinha N 02127201010.1111/j.1540-8175.2010.01185.x 20545989 · doi ↗ · pubmed ↗
- 8Infective endocarditis in the Netherlands: current epidemiological profile and mortality: an analysis based on partial ESC EORP collected data Neth Heart J El Kadi S van den Buijs DM Meijers T 5265362820203250434010.1007/s 12471-020-01431-z PMC 7494701 · doi ↗ · pubmed ↗