Segmental Vitiligo: Rapid Spread From a Halo Nevus
Monica Z Trevino, Jodie Shao, Elene Valladares, Dale Quest

TL;DR
This paper reports a rare case of segmental vitiligo developing from a halo nevus in a teenager, highlighting its distinct unilateral pattern and lack of autoimmune comorbidities.
Contribution
The paper presents a rare clinical case linking a halo nevus to segmental vitiligo, emphasizing its unique characteristics and implications for diagnosis.
Findings
The depigmentation followed Blaschko’s lines and halted at the midline, typical of segmental vitiligo.
The patient showed no autoimmune comorbidities, aligning with the segmental vitiligo pattern.
Recent guidelines suggest topical calcineurin or JAK/STAT inhibitors as first-line treatments.
Abstract
Vitiligo, a skin condition characterized by depigmentation, is classified into segmental and non-segmental forms based on onset and distribution. While halo nevi typically accompany non-segmental vitiligo, this report documents a rare case where a halo nevus transitioned into segmental vitiligo in an adolescent male. The depigmentation exhibited a distinct unilateral pattern, halting at the midline, which is characteristic of segmental vitiligo. Unlike non-segmental vitiligo, segmental vitiligo is less commonly associated with autoimmune diseases, and this patient's lack of autoimmune comorbidity aligns with that pattern. The depigmentation followed Blaschko’s lines, which typically do not cross the midline. Based on the consultation at the time, no immediate treatment was recommended. Recent guidelines suggest first-line use of topical calcineurin inhibitors like tacrolimus or JAK/STAT…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
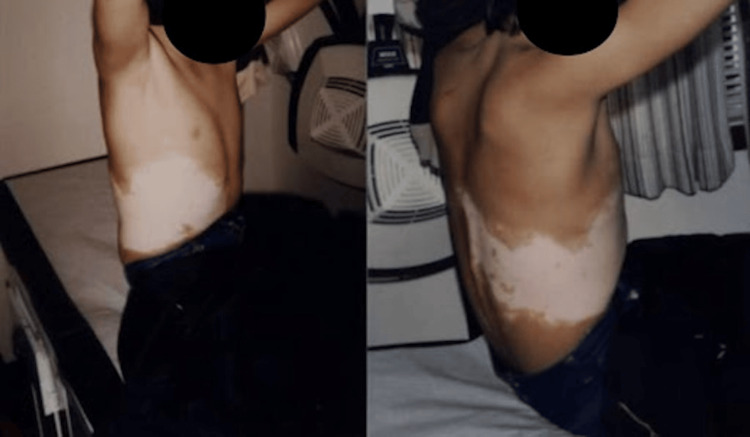 Figure 1
Figure 1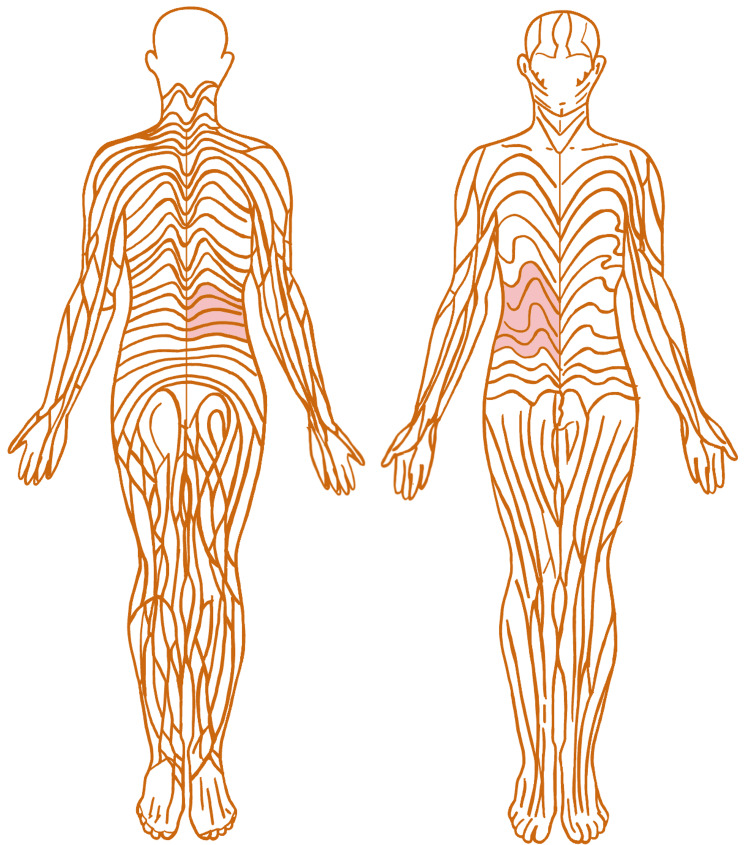 Figure 2
Figure 2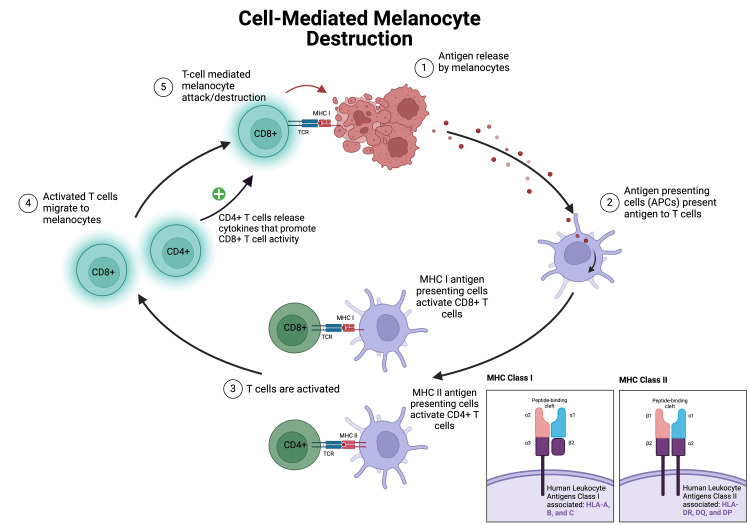 Figure 3
Figure 3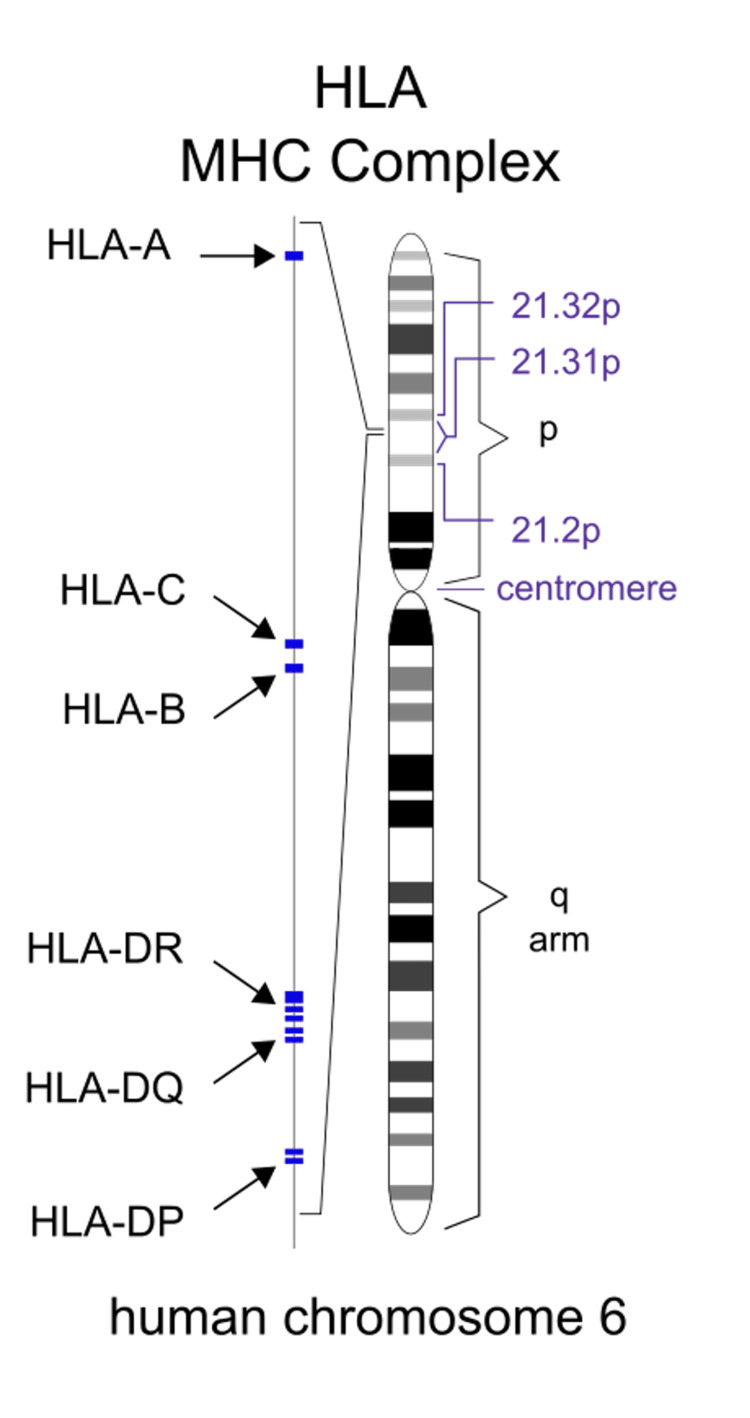 Figure 4
Figure 4| Segmental Vitiligo | Nonsegmental Vitiligo | Case Presentation: Segmental Vitiligo From a Halo Nevus | |
| Onset | Childhood or adolescence [ | Bimodal [ | Adolescent |
| Koebner’s phenomenon | Rarely observed [ | Commonly observed [ | Not observed |
| Presence of halo nevi | Uncommon [ | Common [ | Observed |
| Distribution | Unilateral with a sharp demarcation around the midline [ | Symmetrical well-defined macules crossing midline [ | Unilateral, halted at the midline |
| Depigmentation progression | Rapid progression, stabilizes without further spread [ | Variable, can continue spreading throughout life [ | Rapid spread in segmental pattern, then quiescent |
| Autoimmune disease linkages | Less correlation [ | Linked with allergies and other immunological diseases like canities (premature hair graying) or atopy [ | No known autoimmune diseases |
| Treatment | Topical therapies, targeted phototherapy, and surgical therapy [ | Topical therapies, targeted phototherapy, and surgical therapy [ | No FDA-approved treatment for pediatric vitiligo [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
Topicsmelanin and skin pigmentation · Mast cells and histamine · RNA regulation and disease
Introduction
This report presents a case of segmental vitiligo evolving from a halo nevus in an adolescent. A halo nevus is a mole with a surrounding halo of depigmented skin caused by the immune system attacking melanocytes, the cells that give skin its pigment. Melanocyte destruction is correlated with interferon-gamma (IFN-γ) release, therefore activating CXCR3+ CD8+ T cells, triggering melanocyte apoptosis. The nevus will gradually decrease in size and disappear spontaneously, leaving only depigmented skin [1]. This is thought to be a potential signal for the onset of vitiligo. Sometimes, the area will re-pigment outwardly from spared melanocytes in the hair follicle over months or years. Koebner’s phenomenon, observed as a trigger for conditions including vitiligo or psoriasis, manifests in areas where the skin has been injured or irritated [2,3]. As such, sunburns can act as a physical trigger for Koebner's phenomenon, leading to the progression of trauma-induced depigmentation in susceptible individuals [3].
This case was previously presented at the 2nd Annual El Paso Pediatric Colloquium as a clinical conundrum on June 6, 2015.
Case presentation
A male adolescent of Athapaskan descent (Dene) initially presented with a single halo nevus at the right fourth intercostal level along the anterior axillary line. The initial and only halo nevus present was a dark mahogany color approximately 2.5 mm in diameter. The depigmented skin around the nevus was around 1.5 cm, displaying a symmetrical, pink-cream hue. After the initial consultation with a senior dermatologist, it was assumed that the depigmented patch would halt and remain quiescent. However, the depigmented patch rapidly evolved over one week across the right chest up to the midline and then remained quiescent, as seen at the time of follow-up from the initial visit (Figure 1). This pattern of spreading is typical for segmental vitiligo but unusual in its association with a halo nevus.
Segmental pattern Spread of segmental depigmentation across the right side of the chest, halting at the midline.
In addition to segmental vitiligo, the patient’s symmetrical pityriasis alba on the cheeks presented as non-defined, hypopigmented patches with slight scaling. The patient's skin condition did not extend beyond the described areas, and there were no other significant dermatological findings. The diagnosis was confirmed visually, as standard diagnostic tools were unavailable in the rural setting of the visit.
The examination revealed no other associated symptoms or signs of systemic illness. The patient was not being treated for any conditions, with no known history or family history of autoimmune diseases, which is a consideration in cases of nonsegmental vitiligo. This case was seen during a locum tenens, and labs were not performed at the time.
Discussion
Segmental vitiligo spreading from a halo nevus, as seen in our case, is rare and typically follows Blaschko’s lines, not crossing the midline [4-6]. Misattribution is not surprising for this pattern; due to its dermatomal pattern, some suggest it should be termed zosteriform rather than Blaschoid [7]. Blaschko's lines have an arc-like arrangement, as seen in Figure 2, and result from cutaneous mosaicism. Table 1 provides a concise comparison of segmental and non-segmental vitiligo with our case.
Blashcko's linesThe highlighted segments of the figure represent areas of depigmented skin identified on the adolescent male presented in our case.This image is adapted from: Blaschko A. (1901) Die Nervenverteilung in der Haut in ihrer Beziehung zu den Erkrankungen der Haut. Retrieved from public domain [11].
Manifestation
Cutaneous mosaicism refers to the presence of multiple genetic cell populations, some mutated and some not, within the same skin area. Variations in human leukocyte antigen (HLA) genes potentially influence the development of vitiligo by affecting self-antigen presentation to T cells, leading to healthy melanocyte destruction [12]. As illustrated in Figure 3, CD8+ T cells infiltrate the skin and release cytotoxic molecules like granzyme B and perforin, leading to the apoptosis of melanocytes. Interferon-gamma (IFN-γ) is secreted by activated CD8+ T cells, promoting an inflammatory environment through pathways like JAK-STAT and other cytokines, while also inducing the expression of chemokine (C-X-C motif) ligands 9 and 10 to attract more C-X-C chemokine receptors like CXCR3+ T cells to the site of inflammation [10]. CXCR3+ is suggested to have a role in the generation of effector and memory T cells amplifying immune response and trafficking of T cells against melanocytes [10,13].
Cell-mediated melanocyte destructionThis figure shows the process in which antigen-presenting cells (APCs) identify antigens from melanocytes as foreign material in vitiligo. Diagrams of both major histocompatibility complexes (MHCs) I and II include which human leukocyte antigens (HLA) they are respectively associated with. Adapted from a BioRender template titled "Antigen Presentation in Cancer" [14].
HLA genes, part of major histocompatibility complexes (MHCs), are crucial in distinguishing self from foreign material in the immune system, as seen in Figure 4.
HLA MHC complex on chromosome 6The human leukocyte antigen (HLA) genes, responsible for encoding major histocompatibility complex (MHC) proteins, are located on chromosome 6. MHC I is associated with the HLA A, B, and C genes. MHC II is associated with the HLA DR, DQ, and DP genes.Sourced from Wikimedia Commons [15].
Follow-up with audiologists and ophthalmologists is recommended due to potential melanocyte destruction in the inner ear and iris, causing sensorineural hearing loss or uveitis [16]. Specific HLA genetic expressions, such as HLA-DR4, correlate with different vitiligo manifestations [17]. Patients with segmental vitiligo linked to halo nevi likely possess HLA genes, reducing their risk of developing other autoimmune diseases, explaining the lower incidence of autoimmune diseases in segmental vitiligo compared to non-segmental forms [12].
Treatment
At the time of the visit, there were no immediate treatment recommendations. The spread of the depigmented patch after the first visit was unpredictable. According to the guidelines, the first-line use of topical calcineurin inhibitors in pediatric vitiligo, like tacrolimus, has shown effectiveness for depigmentation on the head and neck with intermediate response on the trunk and extremities [10]. JAK/STAT inhibitors like ruxolitinib in patients 12 years and older have been FDA-approved since 2022 for vitiligo affecting less than 10% of the body surface area [10]. Ruxolitinib is a JAK/STAT inhibitor and therefore prevents CD8+ T cell recruitment for melanocyte destruction. Narrow-band ultraviolet B (NB-UVB) phototherapy is used for larger affected areas or can be used in combination with topical calcineurin inhibitors [18].
Conclusions
This case of an adolescent developing segmental vitiligo from an initial halo nevus is noteworthy. Typically, segmental vitiligo is not linked to the presence of a halo nevus as much as it is associated with nonsegmental vitiligo. Recognizing diverse manifestations of vitiligo may promote earlier treatment interventions. Increasing awareness of atypical presentations might lead to improved management strategies and outcomes for patients with vitiligo.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vitiligo: a review Dermatology Bergqvist C Ezzedine K 57159223620203215562910.1159/000506103 · doi ↗ · pubmed ↗
- 2Hot spots for clinical signs of disease activity in vitiligo Exp Dermatol Delbaere L van Causenbroeck J Duponselle J Van Goethem C Speeckaert R van Geel N 033202410.1111/exd.1497537975576 · doi ↗ · pubmed ↗
- 3Pediatric to adult shift in vitiligo onset suggests altered environmental triggering J Invest Dermatol Jin Y Santorico SA Spritz RA 24124314020203126067110.1016/j.jid.2019.06.131 · doi ↗ · pubmed ↗
- 4Comparison of childhood vitiligo presenting with or without associated halo nevi Pediatr Dermatol Cohen BE Mu EW Orlow SJ 44483320162657309310.1111/pde.12717 · doi ↗ · pubmed ↗
- 5Clinical practice. Vitiligo N Engl J Med Taïeb A Picardo M 16016936020091912952910.1056/NEJ Mcp 0804388 · doi ↗ · pubmed ↗
- 6Autoimmunity in segmental vitiligo Front Immunol Speeckaert R Lambert J Bulat V Belpaire A Speeckaert M van Geel N 5684471120203319334210.3389/fimmu.2020.568447 PMC 7655129 · doi ↗ · pubmed ↗
- 7Different phenotypes of segmental vitiligo based on a clinical observational study J Eur Acad Dermatol Venereol van Geel N De Lille S Vandenhaute S Gauthier Y Mollet I Brochez L Lambert J 6736782520112084034310.1111/j.1468-3083.2010.03847.x · doi ↗ · pubmed ↗
- 8Clinical and epidemiological characteristics of childhood vitiligo: a study of 701 patients from Brazil Int J Dermatol Martins CP Hertz A Luzio P Paludo P Azulay-Abulafia L 2362445920203154423810.1111/ijd.14645 · doi ↗ · pubmed ↗