Pleomorphic adenoma of the lip: a case report and literature review
Rawa M Ali, Rebaz M Ali, Aras J Qaradakhy, Dilan S Hiwa, Ari M Abdullah, Diyar A Omar, Shko H Hassan, Abdullah A Qadir, Abdulwahid M Salih, Fahmi H Kakamad

TL;DR
This paper reports a rare case of a pleomorphic adenoma in the upper lip of a young man and emphasizes the importance of complete surgical removal to prevent recurrence.
Contribution
The novelty lies in presenting a rare case of upper lip pleomorphic adenoma in a young adult and reinforcing diagnostic and treatment considerations.
Findings
A 29-year-old male presented with a painless, slow-growing upper lip swelling confirmed as pleomorphic adenoma.
Complete surgical excision with clear margins prevented recurrence at the 7-month follow-up.
Pleomorphic adenoma should be considered in the differential diagnosis of upper lip swellings.
Abstract
Pleomorphic adenoma (PA) most commonly affects the major salivary glands but can also involve the minor salivary glands, particularly those of the hard and soft palate. However, the current study aims to present a case of upper lip PA. A 29-year-old male presented with a painless, firm, slow-growing swelling (1.5 × 1.5 cm) on the left upper lip. Ultrasonography showed a solid, hypoechoic nodule with irregular margins and mild peripheral vascularity. The encapsulated tumor was excised, and histopathology confirmed PA. At the 7-month follow-up, no evidence of recurrence was observed. Though typically seen in adults aged 40–70, PA can affect younger patients. Complete excision with clear margins is essential due to the risk of recurrence or malignant transformation. PA should be considered in the differential diagnosis of upper lip swellings.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
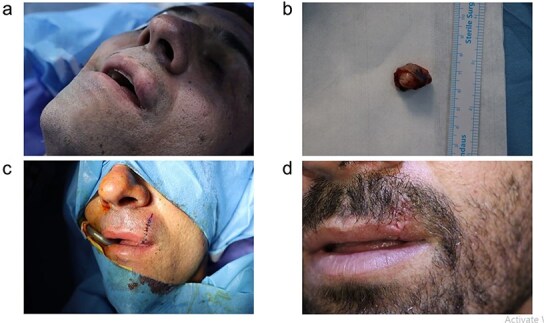 Figure 1
Figure 1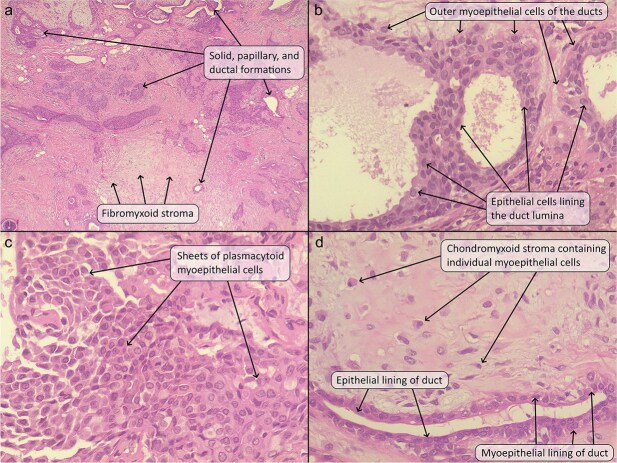 Figure 2
Figure 2|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mamat | 1 | Malaysia | 4 | Male | Painless lump for 3 years. | Central | 15 × 10 | Partially encapsulated pleomorphic adenoma with variable epithelial and stromal components. | Surgical excision | 6 | No | |
| Kazikdas | 1 | Cyprus | 20 | Male | Gradually enlarging painless mass for 2 years. | Right | 40 × 30 | Well-circumscribed submucosal lobular tumor consisting of ductal tubules lined by cuboidal cells, with adjacent areas of chondroid and myxoid stroma and proliferation of clusters of epithelial cells. | Surgical excision with abdominal fat harvested through a 15-mm inferior umbilical incision and inserted into the excision site as a volume filler. | 12 | No | |
| Gelidan | 1 | Saudi Arabia | 46 | Male | No | 2-year history of painless, progressive upper lip external swelling. | Left | 15 × 10 | Circumscribed benign minor salivary gland neoplasm that shows epithelial (ductal) component forming the inner layer of cyst and tubules and myoepithelial cells present as the outer layer of cysts and tubules and scattered within the myxoid stroma. | Surgical excision | 12 | No |
| Suka | 1 | Japan | 54 | Female | No | Painless slow-growing mass for 5 years. | Right | 10 × 10 | The tumor tissue consisted of densely proliferating stromal and epithelial cells forming ductal structures. The stroma exhibited myxomatous and hyalinizing degeneration, with some fibrous tissues present, but no cartilaginous tissue was observed. | Surgical excision | 24 | No |
| Qureshi | 1 | Pakistan | 39 | Male | No | Painless gradually progressive swelling for 2 years. | Right | 15 | Circumscribed, encapsulated, biphasic neoplasm composed of stromal and epithelial components. | Surgical excision | ||
| Chiboub | 1 | Tunisia | 24 | Male | Thyroglossal duct cyst | Painless swelling on the lip for 5 years duration. | Left | Polygonal and spindle-shaped myoepithelial cells in a variable background stroma containing mucoid and myxoid areas. | Surgical excision | 28 | No | |
| Alrehaili | 1 | Saudi Arabia | 24 | Female | No | Painless lump and progressive swelling of the lip for 18 months. | Right | 5 × 4 × 3 | An island and sheets of plasmacytoid cells arranged in duct-like structures, with irregular tubules and patterned strands of benign neoplastic cells surrounded by chondromyxoid stroma. Some cystic areas are identified, with variable stroma exhibiting fibrous, chondroid, and myxoid appearance. | Surgical excision | 12 | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Ear and Head Tumors · Cancer and Skin Lesions
Introduction
Salivary glands are divided into major (parotid, sublingual, submandibular) and minor glands, with the latter located in areas like the oral cavity, nasal passages, and oropharynx [1, 2]. Salivary gland tumors represent 3% of head and neck tumors, with pleomorphic adenoma (PA) being the most common benign neoplasm [1, 3]. Minor salivary gland PAs typically affect the soft and hard palates, reflecting the higher embryological distribution of minor salivary glands in these areas compared to the lips, making upper lip involvement a rare occurrence [2, 4–6]. This study reports a case of a 29-year-old male with upper lip PA. Only peer-reviewed papers were included, and the study was written according to CaReL guidelines [7, 8].
Case presentation
Patient information
A 29-year-old male presented with a left anterior upper lip swelling. He had right-sided weakness and spasticity, along with intellectual disability, attributed to an ischemic insult sustained during birth. Family and surgical histories were negative.
Clinical finding
On physical examination, the mass measured approximately 1.5 × 1.5 cm, and it was well-defined, sessile, and firm. The mass had expanded outwards towards the skin rather than inwards towards the oral mucosa. The skin over the mass appeared stretched and had turned pink. No noticeable changes were present in the surrounding area, and there was no regional lymph node enlargement (Fig. 1). The patient also had multiple skin lesions and skin tags.
(a) Preoperative appearance of the mass located in the upper lip. (b) The excised mass. (c, d) The postoperative appearance of the patient.
Diagnostic approach
Ultrasonography revealed a solid, hypoechoic nodule in the left upper lip, measuring 12 × 10 × 9 mm, with irregular margins, mild peripheral vascularity (having a high resistive index of ~1), and full-thickness involvement, features that were highly suspicious. A biopsy was taken, and the histologic findings were suggestive of a pleomorphic adenoma.
Therapeutic intervention
Under general anesthesia and through a longitudinal incision, the fully encapsulated tumor was wholly excised with ease. A layered repair was carried out, involving the closure of the deep dermal and epidermal layers to ensure proper alignment and achieve satisfactory cosmetic outcomes. Gross examination showed a well-defined, white nodule near the vermilion border measuring 1.9 cm in greatest dimension (Fig. 1). Histopathologic examination showed a relatively well-defined nodule under the skin that was composed of variably sized ductal formations showing cystic change, papillary growths, and solid formations, composed of cells that had a small amount of lightly eosinophilic cytoplasm and oval nuclei with fine chromatin and inconspicuous nucleoli. Some of the ducts showed squamous metaplasia, and some contained an eosinophilic secretion. These formations lay within a fibrous and chondromyxoid stroma containing clusters and individual cells with a plasmacytoid, spindled, and stellate configuration, having oval nuclei and fine chromatin. There was a giant cell reaction around the tumor. There was no significant mitotic activity, pleomorphism, or necrosis (Fig. 2).
(a) The tumor comprised of solid clusters and ductal structures (some of which showed intraluminal papillary formations) lying within a fibrous and chondromyxoid stroma. (b) The ductal structures were lined by a luminal layer of epithelial cells and an abluminal layer of myoepithelial cells. (c) Some areas showed sheets of plasmacytoid myoepithelial cells with bland nuclei. (d) The chondromyxoid stroma contained individual plasmacytoid myoepithelial cells and ductal structures. Hematoxylin and eosin stain; original magnification 40× (a), 400× (b–d).
Follow-up and outcome
The patient had no intraoperative complications and had an uneventful postoperative period. At the 7-month follow-up, no evidence of recurrence was observed.
Discussion
The parotid gland is the most common site for PA, comprising 80% of cases, followed by the submandibular gland (10%) [1]. PA can also arise in minor salivary glands, including the palate, buccal mucosa, nasal cavity, and tongue, but lip involvement is rare. The upper lip is six times more frequently affected than the lower lip, and it has been postulated that the disparity in the incidence of PA between the upper and lower lips can be attributed to embryological development. Specifically, the upper lip arises from the fusion of three facial protuberances, while the lower lip forms from the fusion of only two. This more complex fusion process in the upper lip increases the likelihood of ectopic embryonic cells becoming entrapped, thereby raising the risk of tumorigenesis in that region. Furthermore, the upper lip contains a greater number of well-developed labial salivary glands, in contrast to the lower lip, which harbors only a limited number of smaller glands. This anatomical difference may further account for the higher prevalence of PA in the upper lip [4, 9]. While PA’s pathogenesis remains unclear, the presence of chromosomal translocations with breakpoints at 8q12 and 12q13-15 is well recognized. These rearrangements lead to gene fusions involving key transcription factor genes, most notably PLAG1 and HMGA2. It has been revealed that HMGA2 acts as an upstream regulator of PLAG1, and that it modulates IGF2 expression through this transcription factor. This discovery offers a novel mechanistic insight into the aforementioned chromosomal abnormalities observed in PA, highlighting IGF2 as a key oncogenic driver and a potential therapeutic target [10]. Although Chiboub et al. reported a female predominance, recent studies show male cases are also frequent, with no clear sex predilection established (Table 1) [1, 2, 4, 11–14].
PA typically presents in individuals aged 40–70, but cases in children, such as a 4-year-old male reported by Mamat et al., highlight its occurrence across all ages [11, 14]. Though histologically benign, PA can mimic malignancy due to features like capsule invasion, necrosis, increased cellularity, and cytologic atypia, complicating diagnosis [4]. Its slow-growing, painless nature often leads to delayed presentation, with patients typically seeking medical care more than two years after first noticing the mass. This underscores the need to consider PA in the differential diagnosis of lip swellings in both pediatric and adult patients [4, 11, 14].
As PA grows, surgery becomes more challenging, and recurrence risk rises. Surgical excision with clear margins is the standard treatment. Kazikdas et al. used abdominal fat grafting to restore lip contour postexcision [1, 4, 14]. Malignant transformation occurs in 2%–23% of cases, requiring wider margins (1–2 cm) when suspected [1, 4]. Despite being benign, PA demands close follow-up due to the risk of recurrence from capsular rupture during surgery [14]. Although no recurrences were noted in the reviewed cases with one-year follow-up, longer monitoring is necessary to rule out late recurrence. In conclusion, this rare presentation highlights that the differential diagnosis for upper lip swellings should include PA. Complete surgical excision may result in a good outcome, but close follow-up is recommended to monitor for any signs of recurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kazikdas KC, Yalcinozan ET, Dirik MA. Pleomorphic adenoma of the upper lip. Natl J Maxillofac Surg 2020;11:110–2. 10.4103/njms.NJMS_55_1733041587 PMC 7518476 · doi ↗ · pubmed ↗
- 2Gelidan AG, Arab K. Rare upper lip pleomorphic adenoma presents as cutaneous skin lesion: case report. Int J Surg Case Rep 2021;85:106142. 10.1016/j.ijscr.2021.10614234265588 PMC 8281655 · doi ↗ · pubmed ↗
- 3Salih AM, Kakamad FH, Ali SM, et al. Giant pleomorphic adenoma of the parotid gland extending to the parapharyngeal space: a rare case report. Int J Case Rep Images 2018;9:100914 Z 01AS 2018. 10.5348/100914 Z 01AS 2018 CR · doi ↗
- 4Alrehaili J . A unique pleomorphic adenoma in the minor salivary glands of the upper lip: a case report. Pathol Lab Med Int 2023;15:37–41. 10.2147/PLMI.S 415283 · doi ↗
- 5Abdullah AS, Ahmed AG, Mohammed SN, et al. Benign tumor publication in one year (2022): a cross-sectional study. Barw Med J 2023;1:20–5.
- 6Taiwo AO, Akinshipo A, Braimah RO, et al. Pleomorphic adenoma of the upper lip: a case report. Saudi J Med Med Sci 2018;6:32–5. 10.4103/sjmms.sjmms_109_1630787814 PMC 6196673 · doi ↗ · pubmed ↗
- 7Abdullah HO, Abdalla BA, Kakamad FH, et al. Predatory publishing lists: a review on the ongoing battle against fraudulent actions. Barw Med J 2024;2:26–30.
- 8Prasad S, Nassar M, Azzam AY, et al. Ca Re L guidelines: a consensus-based guideline on case reports and literature review (Ca Re L). Barw Med J 2024;2:13–9.