SPNing our wheels—Pancreatic solid pseudopapillary neoplasm as an extraluminal etiology of persistent duodenal ulceration
Kanak V. Kennedy, Jibraan A. Fawad, Y. Dana Neugut, Doris Valenzuela‐Araujo, Alexander Coe, Tricia R. Bhatti, Michael Acord, Michael D. Manfredi, Petar Mamula, Kathleen M. Loomes, Jefferson N. Brownell

TL;DR
A rare pancreatic tumor was found to cause persistent duodenal ulcers in a child, highlighting the need to consider extraluminal causes in such cases.
Contribution
This case report identifies a pancreatic solid pseudopapillary neoplasm as a rare extrinsic cause of duodenal ulceration in a pediatric patient.
Findings
A pancreatic head solid pseudopapillary neoplasm presented with duodenal ulceration and recurrent upper GI bleeding.
Extraluminal etiologies should be considered when duodenal ulcers recur or progress without other known causes.
Abstract
Pediatric upper gastrointestinal (GI) bleeding secondary to duodenal ulceration is a potentially serious and life‐threatening condition with a broad differential diagnosis. We present a pediatric case of a pancreatic head solid pseudopapillary neoplasm (SPN) presenting with duodenal ulceration and recurrent upper GI bleeding. This case highlights pancreatic SPNs as a rare extrinsic cause of duodenal ulceration. Recurrence and progression in size and extent of a duodenal ulceration in the absence of other inciting factors should raise suspicion for an extraluminal etiology.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
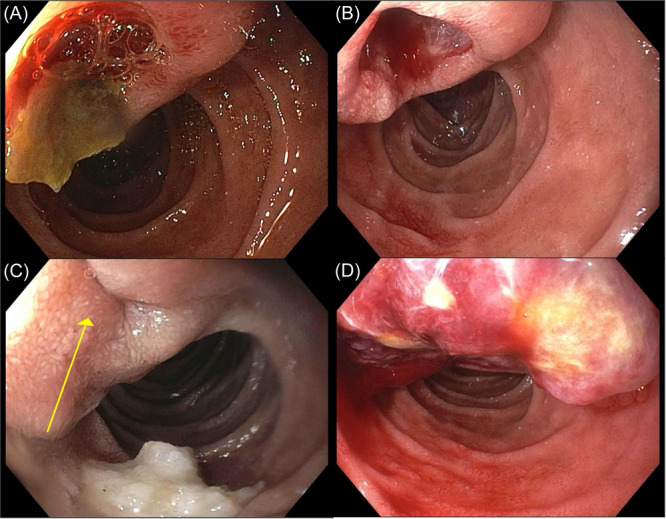 Figure 1
Figure 1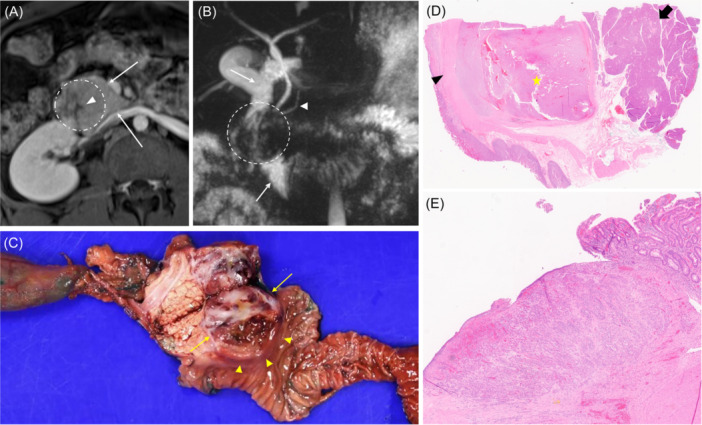 Figure 2
Figure 2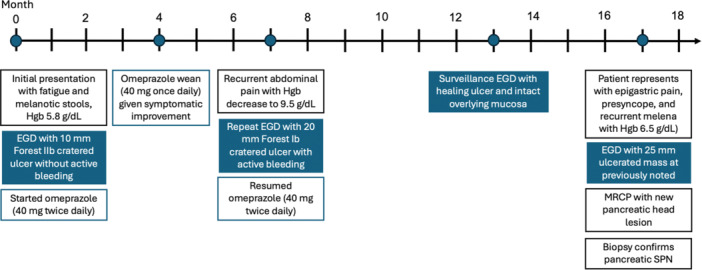 Figure 3
Figure 3- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gastrointestinal disorders and treatments · Pancreatitis Pathology and Treatment
INTRODUCTION
1
Pediatric upper gastrointestinal (GI) bleeding is a potentially serious and life‐threatening condition, with mortality rates as high as 5%–21% depending on the underlying etiology.1 Effective identification and management of the underlying condition is crucial to reducing morbidity and mortality. Here, we present a case of an adolescent female who presented with recurrent upper GI bleeding secondary to persistent duodenal ulceration.
CASE REPORT
2
A 14‐year‐old female presented to our tertiary care center emergency department with a 5‐day history of progressive fatigue and dizziness, and was found to have significant normocytic anemia (hemoglobin 5.8 g/dL, normal 12.0–16.0 g/dL; hematocrit 19.8%, normal 36.0%–46.0%; mean corpuscular volume 78 fL, normal 78.0–102.0 fL). She denied any associated syncopal episodes, focal weakness, or vision changes, but on further questioning reported intermittent melenic stools. She denied upper GI tract symptoms, including nausea, vomiting, dysphagia, abdominal pain, or hematemesis. She had no associated weight loss. Her past medical history was notable for sacrococcygeal teratoma in infancy, diagnosed in utero and treated with chemotherapy and surgical resection. She had no family history of inflammatory GI disease or bleeding/clotting disorders. She denied any prior nonsteroidal anti‐inflammatory drug (NSAID) use and was not on any scheduled or as needed medications before admission.
Further evaluation revealed positive fecal occult blood, significant iron deficiency (ferritin 2.1 ng/mL, normal 10.0–67.4 ng/mL; transferrin 377 mg/dL, normal 180–370 mg/dL; transferrin saturation 2.0%, normal 6%–40%), normal prothrombin time, partial thromboplastin time, and international normalized ratio, negative Helicobacter pylori stool antigen, normal fecal calprotectin, and negative infectious stool studies. Bowel ultrasound showed no bowel wall thickening or hyperemia and a magnetic resonance (MR) abdomen/pelvis without intravenous contrast showed no tumor recurrence. Esophagogastroduodenoscopy (EGD) was performed and demonstrated a 10‐mm Forrest IIb cratered ulcer with an adherent clot in the second portion of the duodenum adjacent to the major papilla (Figure 1A). Biopsies obtained adjacent to the ulcer demonstrated no pathologic diagnosis, including no evidence of H. pylori infection. Colonoscopy was visually and histologically normal. She was started on high‐dose acid suppression with omeprazole (40 mg twice daily) and discharged with plan for close outpatient follow‐up.
Endoscopic evolution of patient's duodenal ulceration appearance. Duodenal ulcer images at time of (A) initial presentation, (B) subsequent episode of recurrent anemia and abdominal pain, (C) surveillance endoscopy during asymptomatic period, and (D) at time of SPN diagnosis. SPN, solid pseudopapillary neoplasm.
Given symptomatic improvement without recurrence of melena, omeprazole was weaned after 4 months to 40 mg once daily. After 3 months, the patient's hemoglobin decreased from 12.0 to 9.5 g/dL (normal 12.0–16.0 g/dL). This prompted repeat endoscopic evaluation, which demonstrated a larger 20 mm Forrest Ib cratered duodenal ulcer with active bleeding (Figure 1B). Using a duodenoscope, the ulcer was treated with epinephrine and argon plasma coagulation (APC). She resumed high‐dose omeprazole (40 mg twice daily) following endoscopy. Additional evaluation at this time was notable for normal serum gastrin while on omeprazole therapy (83 pg/mL, normal 0–100 pg/mL). Surveillance EGD performed 6 months later demonstrated a healing ulcer with intact overlying mucosa (Figure 1C). Hemoglobin was stable at 13.0 g/dL (normal 12.0–16.0 g/dL) at the time of endoscopy.
The patient presented again 4 months later with 2 weeks of worsening epigastric pain, presyncope, and recurrent melena. Admission laboratory studies demonstrated recurrent severe anemia (Hgb 6.5 g/dL, normal 12.0–16.0 g/dL). She underwent urgent endoscopy, which now showed a new ulcerated mass 25 mm in diameter, protruding into the lumen and distorting the papilla at the previously noted ulcer site (Figure 1D). After epinephrine injection, the bleeding vessel was desiccated with APC, and the mass was biopsied with standard forceps. An MR cholangiopancreatography (MRCP) was obtained while awaiting histopathology analysis, which demonstrated a heterogeneous enhancing lesion in the pancreatic head measuring 4.8 × 4.0 × 3.6 cm^3^ (Figure 2A,B). Biopsy results subsequently confirmed a diagnosis of a pancreatic solid pseudopapillary neoplasm (SPN).
Radiographic imaging and histopathology confirming pancreatic solid pseudopapillary neoplasm. (A) Axial T1 fat‐saturated post‐contrast MR image demonstrates an enhancing mass (dashed circle) within the head of the pancreas (thin arrows). Central ulceration is shown as an area of hypoattenuation (arrowhead). (B) Coronal T2 SPACE MRCP shows a hypointense mass (dashed circle) protruding into the lumen of the duodenum (thin arrows). There was no biliary or pancreatic (arrowhead) duct dilation. (C) Gross images of resected tumor (thin arrows) and adjacent bowel (arrowheads) post‐pylorus‐preserving pancreaticoduodenectomy. (D) Histology of resected tumor (star) located between muscularis propria of the duodenum (black arrowhead) and adjacent, nonneoplastic pancreas (black arrow). Tumor consists of a partially encapsulated proliferation of cytologically bland tumor cells with areas of discohesion and pseudopapillae formation (hematoxylin and eosin stain, 15× original magnification). (E) Higher power view of ulcerated duodenal mucosa overlying tumor (hematoxylin and eosin stain, 200× original magnification). MR, magnetic resonance; MRCP, magnetic resonance cholangiopancreatography.
Primary resection of the tumor with a pylorus‐preserving pancreaticoduodenectomy was performed without complication (Figure 2C). Eight months after resection, the patient has had no further episodes of upper GI bleeding or symptomatic anemia, and surveillance imaging has shown no signs of recurrence.
DISCUSSION
3
We report a rare presentation of pancreatic head SPN in a pediatric patient presenting with duodenal ulceration and upper GI bleeding. Pancreatic SPNs represent only 2%–3% of all primary pancreatic tumors, most frequently affecting young females.2, 3 They typically occur in the pancreatic tail, although pancreatic head lesions can occur more often in adolescents. Clinical symptoms associated with SPNs are often nonspecific, including abdominal pain, nausea, bloating, early satiety, and vomiting. They are slow‐growing and have relatively low malignant potential, with a reported 5‐year survival rate of 98%.2, 4 Up to 10%–15% of cases demonstrate locally aggressive behavior,3, 4, 5, 6 such as invasion of adjacent structures as was seen in our patient. Risk factors for invasive tumor behavior of malignant SPNs include larger tumor size, increased Ki‐67 index, and lymphovascular invasion.3
The differential diagnosis for persistent duodenal ulcers includes drug‐induced injury secondary to NSAIDs and corticosteroid use, H. pylori infection, acid hypersecretory states including Zollinger–Ellison syndrome, inflammatory diseases (Crohn's disease and eosinophilic GI disease), vascular insufficiency, malignancy, foreign bodies, obstruction, and postoperative anastomotic ulceration. In this case, endoscopic biopsies of the mucosa surrounding the patient's ulcer site were obtained on several occasions, with histopathology reassuring against underlying infection and inflammatory diseases. Further, she had no history of NSAID or corticosteroid exposure, and serum gastrin levels were within normal limits on acid suppression.
Of note, our patient was evaluated with cross‐sectional imaging with MR abdomen/pelvis without intravenous contrast at the time of her initial presentation, months before her definitive diagnosis (Figure 3). While the imaging was tailored to evaluate for recurrent germ cell tumors given the patient's past medical history, retrospective comparison of that study to her subsequent MRCP at diagnosis showed a small enhancing mass in the head of the pancreas measuring 3 × 2.2 × 2 cm^3^ (anteroposterior × transverse × craniocaudal) that was not appreciated at the time of the original study. The evolving imaging findings during our patient's 2‐year clinical course are consistent with the natural history of locally aggressive pancreatic SPNs described in the literature.7
Timeline of patient's clinical course from initial presentation to SPN diagnosis. EGD, esophagogastroduodenoscopy; Hgb, hemoglobin; mg, milligram; MRCP, magnetic resonance cholangiopancreatography; SPN, solid pseudopapillary neoplasm.
This case highlights pancreatic SPNs as a rare extrinsic cause of duodenal ulceration. Recurrence and progression in size and extent of a duodenal ulceration in the absence of other inciting factors should raise suspicion for an extraluminal etiology.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sur LM , Armat I , Sur G , et al. Practical aspects of upper gastrointestinal bleeding in children. J Clin Med. 2023;12:2921. 10.3390/jcm 12082921 37109257 PMC 10145382 · doi ↗ · pubmed ↗
- 2Sun G , Fang K , Fu X , et al. Solid pseudopapillary neoplasm of the pancreas: a multi‐institution study of 118 cases. Pancreas. 2023;52:e 121‐e 126.37523603 10.1097/MPA.0000000000002219 · doi ↗ · pubmed ↗
- 3Lu X , Chen H , Zhang T . Solid pseudopapillary neoplasm (SPN) of the pancreas: current understanding on its malignant potential and management. Discov Oncol. 2024;15:77.38498246 10.1007/s 12672-024-00905-5PMC 10948659 · doi ↗ · pubmed ↗
- 4Mylonas KS , Doulamis IP , Tsilimigras DI , et al. Solid pseudopapillary and malignant pancreatic tumors in childhood: a systematic review and evidence quality assessment. Pediatr Blood Cancer. 2018;65:e 27114.29697193 10.1002/pbc.27114 · doi ↗ · pubmed ↗
- 5Hao EIU , Hwang HK , Yoon D‐S , Lee WJ , Kang CM . Aggressiveness of solid pseudopapillary neoplasm of the pancreas: a literature review and meta‐analysis. Medicine. 2018;97:e 13147.30544374 10.1097/MD.0000000000013147 PMC 6310540 · doi ↗ · pubmed ↗
- 6Silva RJ , Oliveira INF , Ribeiro TCR , Chebli LA , Chebli JMF . A rare presentation of a solid pseudopapillary neoplasm of the pancreas. GE Port J Gastroenterol. 2022;29:135‐138.35497660 10.1159/000514783 PMC 8995665 · doi ↗ · pubmed ↗
- 7Wang X , Zhu D , Bao W , Li M , Wang S , Shen R . Prognostic enigma of pancreatic solid pseudopapillary neoplasm: a single‐center experience of 63 patients. Front Surg. 2021;8:771587.34881287 10.3389/fsurg.2021.771587 PMC 8645639 · doi ↗ · pubmed ↗