Rapid chronic kidney disease progression in younger, First Nations patients in the Northern Territory
Winnie Chen, Oyelola Adegboye, Gillian Gorham, Asanga Abeyaratne, Sandawana William Majoni, Sean Taylor, Samuel Heard, Harshana Munasinghe, Matthew J. L. Hare, Alan Cass

TL;DR
Younger First Nations patients in Australia's Northern Territory experience faster chronic kidney disease progression, highlighting the need for early interventions.
Contribution
Identifies younger First Nations patients as a high-risk group for rapid CKD progression in a remote Australian setting.
Findings
Younger patients under 50 had higher risk of progressing to kidney replacement therapy or death.
CKD progression is more rapid in younger First Nations individuals in the Northern Territory.
Early intervention is critical for younger patients to prevent severe outcomes.
Abstract
This 6‐year retrospective cohort study investigated the progression of chronic kidney disease (CKD) among Australian First Nations patients in remote Northern Territory. We found that younger patients (age less than 50 years) were at a higher risk of progression to kidney replacement therapy or death compared to older adults. The results indicate a need to target early CKD intervention efforts to younger patients at risk of rapid progression.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
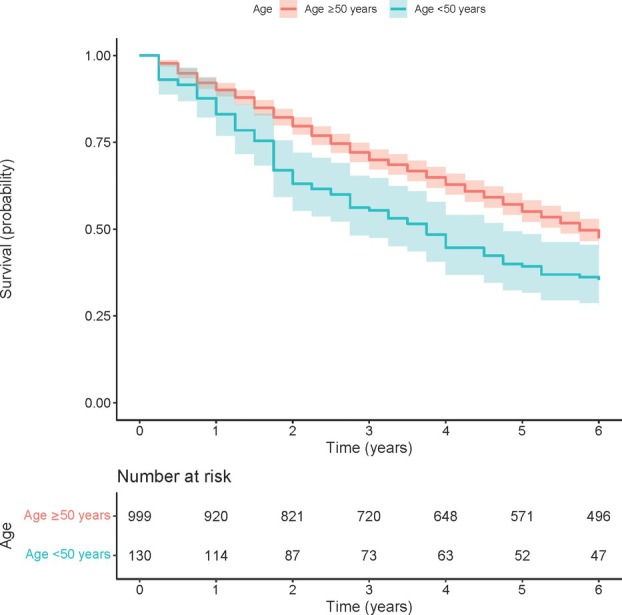 Figure 1
Figure 1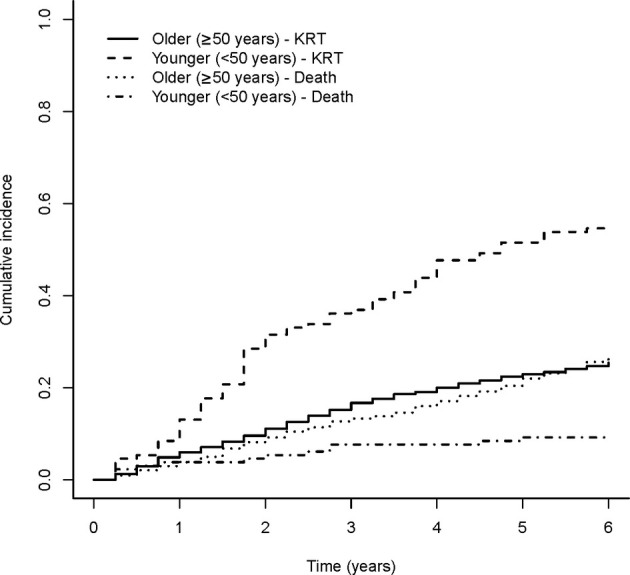 Figure 2
Figure 2- —Ian Potter Foundation 10.13039/501100001047
- —National Health and Medical Research Council 10.13039/501100000925
- —Medical Research Future Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Kidney Disease and Diabetes · Dialysis and Renal Disease Management · Healthcare cost, quality, practices
Remote Northern Territory (NT) communities in Australia are a hotspot for chronic kidney disease (CKD).1 Australian First Nations people in the NT have over 30% prevalence of CKD compared to approximately 10% in non‐First Nations people, with a much higher prevalence of end‐stage kidney disease (ESKD).2, 3 As with other First Nations populations globally, the heavy burden of CKD in remote NT is associated with social disadvantage.4 The Australian and New Zealand Dialysis and Transplant (ANZDATA) registry data reports the median age of dialysis initiation in the NT to be 51 years – more than a decade younger than the median age (63 years) across all dialysis centres in Australia and New Zealand.5 Despite recognition that First Nations patients commencing dialysis are younger, there remains limited understanding regarding differences in CKD progression by age. In this study, we aimed to examine the differences in CKD progression by age among First Nations people in the remote NT.
This was a retrospective cohort study using data from the Territory Kidney Care database, covering a 6‐year follow‐up period from 2017 to 2023, with longitudinal data available in 3‐monthly intervals. The database contains individual‐level electronic health record (EHR) data from all NT public hospitals (n = 6), all NT Health remote primary health clinics (n = 56) and the majority of Aboriginal Community Controlled Health Organisations (ACCHOs) in the NT (n = 11).6, 7 In remote NT, NT Health and ACCHO clinics are the sole primary healthcare providers, serving predominantly First Nations patients. Clinical information extracted included demographic details, coded diagnoses, and laboratory results. The presence of CKD and related chronic conditions is determined using previously validated EHR‐based algorithms.8 The inclusion criteria for this study were First Nations patients currently attending a participating remote primary health clinic, older than 16 years of age, with CKD stage 3a to CKD stage 5. CKD patients already on kidney replacement therapy (KRT) at baseline were excluded from the study.
Medians and interquartile ranges (IQRs) were reported for continuous variables, while categorical variables were presented as counts with percentages. The primary outcome of interest was time to a combined endpoint of KRT or death, with a focus on describing differences in outcomes between those who are younger (<50 years) and older (≥50 years). This age cut‐off was based on the median age of dialysis initiation in the NT (51 years).5 Secondary outcomes included time to KRT and time to death. Unadjusted and adjusted Cox proportional hazards (PH) were used to describe the association between age categories and the primary outcome. As KRT and death are competing risks, an additional competing risk analysis was performed. Cumulative incidence function for KRT and death according to age category, and results of the Fine‐Gray model were reported. Statistical analyses were conducted in R (version 4.2.3)9 and Python (version 3.9.12).10 Ethics approval was granted by NT Health and Menzies School of Health Research Human Research Ethics Committee (NTHREC 2021‐4102) and was approved by the NT Health Research Governance Office.
The study cohort consisted of 1129 First Nations patients with baseline CKD stages of 3a to 5 (eGFR <60 mL/min per 1.73 m^2^) (Table 1). At baseline, the median age was 60 years, with 36% males. Common comorbidities included hypertension (prevalence 88%), diabetes (78%) and coronary artery disease (37%). Comorbidities were more common in patients with more severe stages of CKD.
Figure 1 presents Kaplan–Meier survival curves of time to KRT or death, comparing younger (<50 years) versus older (≥50 years) age categories. The Kaplan–Meier curves show that median survival to the combined endpoint of KRT or death for younger patients was approximately 3.6 years, compared with 5.6 years in older patients. At the end of the 6‐year follow‐up period, a higher proportion of younger patients progressed to KRT or death (65%) compared to the older group (43%) – see also Table S2. In the unadjusted Cox PH model, younger patients <50 years were at higher risk of progressing to KRT or death compared to older patients ≥50 years (unadjusted HR 1.52, 95% CI 1.21–1.92). When adjusted for gender and comorbidities (diabetes, cardiovascular disease, hypertension), the effect of age category on risk of progression to KRT or death was strengthened (adjusted HR 2.17, 95% CI 1.71–2.75) (Table 2). Figure 2 presents cumulative incidence functions for competing risks of KRT and death by age category. Fine‐Gray's test showed that, when accounting for these two competing risks, the cumulative incidence of KRT remains significantly higher in the younger age category. Full results are available in Appendix S1.
Discussion
While it is well established that First Nations Australians start KRT earlier than non‐First Nations Australians, our study is a first in investigating age‐related differences in CKD progression among a high‐risk group of First Nations patients. We found that within 4 years, over half of younger First Nations patients (<50 years) with CKD in this NT cohort progressed to KRT or had died. We demonstrated that younger patients were at significantly higher risk of progression to KRT compared to older patients, even when the competing risk of death is taken into account. Additional analyses confirmed that age‐related differences remained present when patients were further stratified by baseline CKD stages.
The accelerated progression highlights an urgent need to optimise early management of CKD and target resources towards this higher‐risk cohort. Preventing rapid progression to KRT requires multifaceted approaches, including addressing upstream factors and underlying inequities within healthcare provision, access to culturally safe, high‐quality care for CKD and related chronic conditions in primary healthcare, timely diagnosis and timely access to specialist‐supported care.4
A previous prospective cohort study of First Nations people across northern and central Australia did not show age to be a significant risk factor for CKD progression in terms of eGFR decline or progression to a combined renal endpoint.11 However, few patients in that study (n = 85, 15.5% of the study cohort) had eGFR <60 mL/min per 1.73 m^2^, whereas all 1129 patients in our cohort were CKD patients with eGFR <60 mL/min per 1.73 m^2^ (inclusion criteria stages 3a or higher). Similar to our study, a population‐wide Tasmanian study of patients with CKD stage 4 and above (eGFR <30 mL/min per 1.73 m^2^) showed the risk of death to increase with age, with the risk of KRT decreasing with advanced age.12 However, the Tasmanian study did not access primary care data and was conducted in a much older cohort (median age 81 years, vs median age 60 years in our study).
A strength of this study is that it used linked data from the Territory Kidney Care database, which included longitudinal EHR data from all NT public hospitals and the majority of remote NT Health and ACCHO clinics. This allowed for accurate categorisation of CKD staging, comorbidities and study endpoints (KRT and death). Nevertheless, this was a retrospective study that relied on secondary use of existing EHR data, which had inherent limitations in terms of data accuracy and completeness.13, 14, 15 For example, CKD aetiology could not be accurately ascertained from the current dataset. Future research could consider a more detailed and nuanced analysis of CKD progression, including CKD progression in terms of declines in eGFR over time.11, 16 Using data from across all CKD stages over a longer follow‐up period would facilitate a deeper understanding of how age, gender, comorbidities and access to evidence‐based prevention influence kidney health outcomes.
Supporting information
Appendix S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kidney Health Australia . State of the Nation: 2016 Kidney Health Week – Chronic Kidney Disease Hot Spots. Melbourne: KHA; 2016 (cited 2024 September). Available from URL: https://kidney.org.au/uploads/resources/state-of-the-nation-kidney-health-week-2016-chronic-kidney-disease-hot-spots.pdf
- 2ANZDATA Registry . ANZDATA 46th Annual Report. Adelaide: Australia and New Zealand Dialysis and Transplant Registry; 2023 (cited 2024 September). Available from URL: https://www.anzdata.org.au/report/anzdata-46th-annual-report-2023-data-to-2022/
- 3Li L , Guthridge S , Li SQ , Zhao Y , Lawton P , Cass A . Estimating the total prevalence and incidence of end‐stage kidney disease among Aboriginal and non‐Aboriginal populations in the Northern Territory of Australia, using multiple data sources. BMC Nephrol 2018; 19: 15.29334912 10.1186/s 12882-017-0791-3PMC 5769509 · doi ↗ · pubmed ↗
- 4Tunnicliffe DJ , Bateman S , Arnold‐Chamney M , Dwyer KM , Howell M , Jesudason S et al. Recommendations for Culturally Safe and Clinical Kidney Care for First Nations Australians. Sydney: CARI Guidelines; 2022.10.5694/mja 2.52114 PMC 1095249037838977 · doi ↗ · pubmed ↗
- 5Ethier I , Campbell SB , Cho Y , Hawley CM , Isbel NM , Krishnasamy R et al. Dialysis initiation in older persons across centres and over time in Australia and New Zealand. Nephrology (Carlton) 2021; 26: 613–622.33715269 10.1111/nep.13873 · doi ↗ · pubmed ↗
- 6Gorham G , Abeyaratne A , Heard S , Moore L , George P , Kamler P et al. Developing an integrated clinical decision support system for the early identification and management of kidney disease—building cross‐sectoral partnerships. BMC Med Inform Decis Mak 2024; 24: 69.38459531 10.1186/s 12911-024-02471-w PMC 10924414 · doi ↗ · pubmed ↗
- 7Chen W , Howard K , Gorham G , Abeyaratne A , Zhao Y , Adegboye O et al. Costs and healthcare use of patients with chronic kidney disease in the Northern Territory, Australia. BMC Health Serv Res 2024; 24: 791.38982437 10.1186/s 12913-024-11258-8PMC 11234693 · doi ↗ · pubmed ↗
- 8Chen W , Abeyaratne A , Gorham G , George P , Karepalli V , Tran D et al. Development and validation of algorithms to identify patients with chronic kidney disease and related chronic diseases across the Northern Territory, Australia. BMC Nephrol 2022; 23: 320.36151531 10.1186/s 12882-022-02947-9PMC 9502610 · doi ↗ · pubmed ↗