Valve type and post-dilation impact on transprosthetic gradients in patients undergoing transcatheter aortic valve-in-valve procedure
Manuela Muratori, Laura Fusini, Gloria Tamborini, Paola Gripari, Sarah Ghulam Ali, Valentina Mantegazza, Anna Garlaschè, Francesco Doni, Andrea Baggiano, Francesco Cannata, Alberico Del Torto, Fabio Fazzari, Antonio Frappampina, Daniele Junod, Riccardo Maragna, Saima Mushtaq

TL;DR
This study examines how different valve types and balloon post-dilation affect heart valve replacement outcomes in patients with degenerated aortic valves.
Contribution
The study identifies that self-expandable valves with balloon post-dilation result in lower transprosthetic gradients after valve-in-valve procedures.
Findings
Self-expandable valves with balloon post-dilation had the lowest mean transprosthetic gradients at discharge.
All groups showed improved hemodynamics over time, with no significant difference in 5-year mortality.
Balloon post-dilation significantly reduced gradients compared to valves without post-dilation.
Abstract
Valve-in-Valve transcatheter aortic valve replacement (ViV-TAVR) is an appealing treatment option for patients with degenerated aortic bioprosthetic valves. However, higher post-procedural transprosthetic gradients are more common after ViV-TAVR than after TAVR for native aortic valve stenosis. We sought to evaluate the impact of type of implanted valve and balloon post-dilation on echocardiographic results and mortality in ViV-TAVR patients. One hundred and eleven consecutive patients were enrolled. A balloon-expandable valve, a self-expandable valve without balloon post-dilation, and a self-expandable valve with balloon post-dilation were performed in 35 (Group 1), 39 (Group 2), and 37 (Group 3) patients, respectively. All patients underwent comprehensive transthoracic echocardiography at baseline, discharge, and 6–12 months follow-up. Successful ViV-TAVR was performed in 110…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
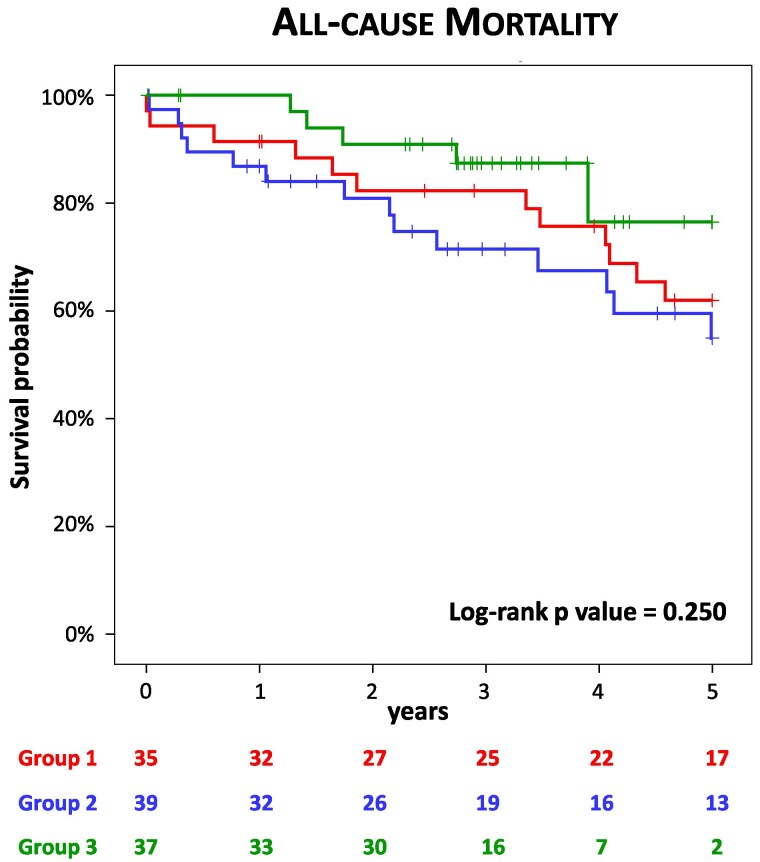 Figure 1
Figure 1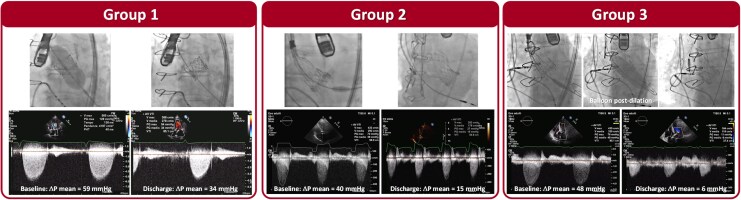 Figure 2
Figure 2| All ( | Group 1 ( | Group 2 ( | Group 3 ( |
| |
|---|---|---|---|---|---|
|
| |||||
| Age, years | 78 ± 8 | 77 ± 11 | 78 ± 7 | 79 ± 5 | 0.409 |
| Female | 57 (51%) | 17 (49%) | 19 (49%) | 21 (56%) | 0.723 |
| Body Surface Area, kg/m2 | 1.76 ± 0.19 | 1.76 ± 0.19 | 1.75 ± 0.20 | 1.77 ± 0.20 | 0.938 |
| Hypertension | 90 (81%) | 27 (77%) | 31 (79%) | 32 (86%) | 0.570 |
| Diabetes mellitus | 27 (24%) | 10 (29%) | 11 (28%) | 6 (16%) | 0.371 |
| Dyslipidaemia | 71 (64%) | 23 (66%) | 20 (51%) | 28 (76%) | 0.083 |
| Angina | 16 (14%) | 7 (20%) | 6 (15%) | 3 (8%) | 0.349 |
| Dyspnoea | 110 (99%) | 34 (97%) | 39 (100%) | 37 (100%) | 0.334 |
| Syncope | 2 (2%) | 2 (6%) | 0 (0%) | 0 (0%) | 0.110 |
| Chronic obstructive pulmonary disease | 29 (26%) | 12 (35%) | 11 (28%) | 6 (16%) | 0.180 |
| eGFR < 60 mL/min/1.73 m2 | 68 (61%) | 20 (57%) | 26 (67%) | 22 (59%) | 0.677 |
| NYHA functional classes III–IV | 86 (77%) | 28 (80%) | 33 (85%) | 25 (68%) | 0.187 |
| Peripheral vascular disease | 30 (27%) | 10 (29%) | 10 (25%) | 10 (27%) | 0.961 |
| Coronary artery disease | 40 (36%) | 13 (37%) | 15 (38%) | 12 (32%) | 0.849 |
| Prior myocardial infarction | 10 (9%) | 4 (11%) | 4 (10%) | 2 (5%) | 0.634 |
| Prior percutaneous coronary intervention | 21 (19%) | 4 (11%) | 9 (23%) | 8 (22%) | 0.388 |
| Prior coronary artery bypass graft | 27 (24%) | 8 (23%) | 10 (26%) | 9 (24%) | 0.962 |
| Atrial flutter/fibrillation | 24 (22%) | 8 (23%) | 9 (23%) | 7 (19%) | 0.887 |
|
| |||||
| LVEDV index, mL/m2 | 78 ± 30 | 78 ± 31 | 79 ± 29 | 78 ± 32 | 0.989 |
| LVESV index, mL/m2 | 36 ± 22 | 36 ± 21 | 38 ± 22 | 34 ± 22 | 0.750 |
| LVEF, % | 56 ± 11 | 56 ± 11 | 54 ± 13 | 60 ± 10 | 0.082 |
| LV mass index, g/m2 | 146 ± 44 | 151 ± 37 | 146 ± 47 | 142 ± 46 | 0.824 |
| LA volume index, mL/m2 | 59 ± 22 | 67 ± 32 | 55 ± 14 | 55 ± 16 | 0.054 |
| AVA, cm2 | 0.99 ± 0.47 | 0.89 ± 0.3 | 1.07 ± 0.53 | 1.01 ± 0.52 | 0.282 |
| AVA index, cm2/m2 | 0.56 ± 0.26 | 0.51 ± 0.18 | 0.61 ± 0.31 | 0.56 ± 0.27 | 0.241 |
| Mean pressure gradient, mmHg | 38 ± 16 | 41 ± 15 | 36 ± 16 | 37 ± 17 | 0.373 |
| Peak pressure gradient, mmHg | 63 ± 24 | 67 ± 22 | 60 ± 23 | 63 ± 26 | 0.393 |
| PASP, mmHg | 45 ± 13 | 45 ± 12 | 45 ± 13 | 46 ± 13 | 0.895 |
| Mitral regurgitation ≥2 | 59 (53%) | 20 (57%) | 14 (36%) | 22 (59%) | 0.051 |
| Tricuspid regurgitation ≥2 | 34 (31%) | 15 (43%) | 7 (18%) | 12 (32%) | 0.065 |
| Mechanism of failure | 0.697 | ||||
| Stenosis | 45 (41%) | 14 (40%) | 18 (46%) | 13 (35%) | |
| Regurgitation | 41 (37%) | 11 (31%) | 14 (36%) | 16 (43%) | |
| Combined | 25 (22%) | 10 (29%) | 7 (18%) | 8 (22%) |
| Variables | Baseline | Discharge | 6–12 Months |
|
|---|---|---|---|---|
|
| ||||
| LVEDV index, mL/m2 | 78 ± 30 | 70 ± 26 | 62 ± 21 | 0.002 |
| LVESV index, mL/m2 | 37 ± 22 | 34 ± 20 | 26 ± 14 | <0.001 |
| LVEF, % | 56 ± 11 | 54 ± 10 | 61 ± 9 | <0.001 |
| LV mass index, g/m2 | 155 ± 39 | 135 ± 44 | 132 ± 50 | <0.001 |
| LA volume index, mL/m2 | 65 ± 28 | 56 ± 14 | 52 ± 15 | 0.053 |
| AVA, cm2 | 0.87 ± 0.30 | 1.42 ± 0.40 | 1.37 ± 0.31 | <0.001 |
| AVA index, cm2/m2 | 0.49 ± 0.18 | 0.8 ± 0.21 | 0.76 ± 0.17 | <0.001 |
| Mean pressure gradient, mmHg | 41 ± 16 | 20 ± 9 | 23 ± 10 | <0.001 |
| Peak pressure gradient, mmHg | 67 ± 24 | 34 ± 15 | 39 ± 16 | <0.001 |
| PASP, mmHg | 42 ± 8 | 36 ± 7 | 36 ± 9 | <0.001 |
| Aortic valve regurgitation ≥2 | 21 (60%) | 2 (7%) | 2 (7%) | <0.001 |
| Mitral regurgitation ≥2 | 18 (60%) | 11 (37%) | 8 (27%) | 0.008 |
| Tricuspid regurgitation ≥2 | 12 (40%) | 6 (20%) | 2 (7%) | 0.003 |
|
| ||||
| LVEDV index, mL/m2 | 75 ± 27 | 66 ± 27 | 60 ± 21 | <0.001 |
| LVESV index, mL/m2 | 36 ± 22 | 31 ± 21 | 26 ± 17 | 0.001 |
| LVEF, % | 55 ± 13 | 56 ± 11 | 58 ± 11 | 0.132 |
| LV mass index, g/m2 | 144 ± 47 | 128 ± 39 | 122 ± 29 | 0.014 |
| LA volume index, mL/m2 | 54 ± 15 | 53 ± 16 | 53 ± 14 | 0.856 |
| AVA, cm2 | 1.00 ± 0.53 | 1.62 ± 0.54 | 1.59 ± 0.46 | <0.001 |
| AVA index, cm2/m2 | 0.58 ± 0.31 | 0.92 ± 0.29 | 0.9 ± 0.24 | <0.001 |
| Mean pressure gradient, mmHg | 38 ± 16 | 18 ± 9 | 18 ± 11 | <0.001 |
| Peak pressure gradient, mmHg | 63 ± 23 | 32 ± 16 | 32 ± 17 | <0.001 |
| PASP, mmHg | 44 ± 12 | 34 ± 9 | 37 ± 10 | <0.001 |
| Aortic valve regurgitation ≥2 | 21 (53%) | 4 (13%) | 4 (13%) | <0.001 |
| Mitral regurgitation ≥2 | 11 (36%) | 5 (16%) | 5 (16%) | 0.038 |
| Tricuspid regurgitation ≥2 | 5 (16%) | 2 (7%) | 4 (13%) | 0.247 |
|
| ||||
| LVEDV index, mL/m2 | 79 ± 33 | 63 ± 27 | 61 ± 23 | <0.001 |
| LVESV index, mL/m2 | 34 ± 23 | 30 ± 21 | 26 ± 17 | <0.001 |
| LVEF, % | 60 ± 10 | 56 ± 10 | 59 ± 9 | 0.011 |
| LV mass index, g/m2 | 148 ± 48 | 124 ± 35 | 116 ± 33 | <0.001 |
| LA volume index, mL/m2 | 56 ± 18 | 49 ± 17 | 48 ± 18 | 0.043 |
| AVA, cm2 | 0.98 ± 0.49 | 1.71 ± 0.43 | 1.55 ± 0.48 | <0.001 |
| AVA index, cm2/m2 | 0.54 ± 0.24 | 0.97 ± 0.25 | 0.89 ± 0.28 | <0.001 |
| Mean pressure gradient, mmHg | 36 ± 16 | 12 ± 6 | 13 ± 7 | <0.001 |
| Peak pressure gradient, mmHg | 62 ± 24 | 21 ± 10 | 24 ± 11 | <0.001 |
| PASP, mmHg | 46 ± 13 | 36 ± 9 | 39 ± 9 | <0.001 |
| Aortic valve regurgitation ≥2 | 24 (64%) | 2 (6%) | 2 (6%) | <0.001 |
| Mitral regurgitation ≥2 | 23 (68%) | 16 (47%) | 9 (27%) | <0.001 |
| Tricuspid regurgitation ≥2 | 12 (35%) | 10 (29%) | 7 (21%) | 0.150 |
| Group 1 ( | Group 2 ( | Group 3 ( |
| |
|---|---|---|---|---|
| 1-year | 3 (9%) | 5 (13%) | 0 (0%) | 0.090 |
| 3-year | 6 (17%) | 10 (26%) | 4 (11%) | 0.240 |
| 5-year | 12 (34%) | 14 (36%) | 5 (14%) | 0.056 |
- —Italian Ministry of Health-Ricerca Corrente
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
Introduction
Biological valves are increasingly implanted in patients requiring aortic valve replacement, rather than mechanical valves.^1^ Bioprosthetic valves do not require anticoagulant therapy and have excellent haemodynamic properties. However, their durability is limited because of structural valve degeneration (SVD). Over time, SVD results in prosthesis failure and haemodynamic dysfunction manifested as stenosis, regurgitation, or a combination of both requiring the need for intervention in most cases.^2,3^ The conventional treatment for dysfunctional valve prosthesis has been redo surgery for many years. However, patients with SVD are often elderly and have several comorbidities, which frequently makes them unsuitable candidates for reoperation.^4,5^ Valve-in-Valve transcatheter aortic valve replacement (ViV-TAVR) has been identified as a feasible, less-invasive treatment option for patients with degenerated surgically implanted bioprostheses. Currently, European and US guidelines recommend this approach in high-risk patients with aortic SVD.^6,7^ In these patients, ViV-TAVR has been associated with a high rate (95%) of procedural success and a mean 30-day mortality of 8%. Nevertheless, the Valve-in-Valve International Data (VIVID) Registry has identified several major concerns with this technique: coronary obstruction, valve malposition, and elevated residual gradients.^8,9^ Moreover, it is still unclear whether the elevated residual gradients after ViV procedures are comparable with those reported after redo surgical aortic valve replacement.^10,11^ Regarding post-procedural gradients, the type of transcatheter heart valve selected, as well as the implantation technique, are relevant factors, but they have not been investigated yet.^12,13^ Specifically, balloon post-dilation is a widely embraced strategy used to optimize transcatheter valve expansion, thereby positively affecting paravalvular leaks and mean gradients.
In this study, we aimed to analyse haemodynamic and clinical outcomes after ViV-TAVR and to compare the results according to the use of a balloon-expandable vs. self-expandable valve, with or without balloon post-dilation.
Methods
Study population
Between April 2008 and December 2020, 111 consecutive patients with symptomatic severe bioprosthetic SVD underwent ViV-TAVR at the Centro Cardiologico Monzino IRCCS in Milan, Italy. The decision to perform ViV-TAVR was made by a heart team based on established criteria.^6,7^ Patients with a predominant prosthetic-patient mismatch, thrombosis, endocarditis, or paravalvular regurgitation were excluded. We collected information about the size of the surgical prosthesis and the reason of valve failure. All ViV-TAVR procedures were performed under fluoroscopic guidance. In the majority of patients, transoesophageal echocardiography was used as an adjunct to fluoroscopy to provide an accurate evaluation of valve position and function, with careful assessment of the presence and severity of aortic regurgitation (AR). Patients were stratified according to percutaneous valve type and balloon post-dilation (balloon-expandable vs. self-expandable with and without post-dilation).
A comprehensive transthoracic echocardiography using commercially available equipment (iE33 or EPIQ, Philips Medical System, Andover, Massachusetts; Vivid-7, E9, or E95 GE Healthcare, Horten, Norway) was performed for all patients at baseline, discharge, and 6–12-months follow-up. All echocardiographic examinations were acquired by experienced echocardiographers. The transthoracic echocardiography was performed in multiple cross-sectional and off-axis views with careful attention to assessing the morphology and mobility of prosthetic valve leaflets, evaluating the integrity of the cusps, and detecting the presence of calcification. Left ventricular (LV) end-diastolic and end-systolic volumes and maximal left atrial volume were measured using the biplane Simpson’s method, and LV ejection fraction was derived. Doppler-derived parameters including peak velocity, mean pressure gradient, and velocity-time integral of the jet were assessed from the apical, right parasternal, right supraclavicular, and suprasternal positions. Prosthetic aortic valve area was derived from the continuity equation according to current guidelines.^14,15^ To avoid underestimation, the diameter of the LV outflow tract was measured in the mid-systole from the parasternal long-axis view using a zoomed mode, measuring inner-edge to inner-edge of the prosthetic valve. The LV outflow tract velocity-time integral was obtained using pulsed-wave Doppler by positioning the sample volume 5 mm below the prosthetic aortic leaflets. All echocardiographic measurements were obtained by averaging the values collected over three consecutive cardiac cycles in patients with sinus rhythm, and over five cardiac cycles for those with atrial fibrillation. In the presence of atrial fibrillation, care was taken to obtain measurements during less irregular heart rate, trying to match temporally similar beats for preventing unrepresentative results. To evaluate the presence and severity of prosthetic AR, a combination of the qualitative and semi-quantitative parameters was used according to current guidelines and to VARC-3 document.^14–16^
Clinical events were evaluated according to the Valve Academic Research Consortiun-3 criteria.^16^ The follow-up period was defined as the time between the procedure and the last documented contact with the patient alive or the time of documented death. All-cause mortality rate was reported during the 5-year follow-up period.
The Institutional Review Board and the Ethical Committee of our institution approved the study (CCM–PR182). For retrospective analysis of clinically acquired data anonymously handled, the Ethical Committee waived the need of patient written informed consent.
Statistical analysis
Continuous data are presented as mean ± SD and categorical variables as numbers (percentages), as appropriate. Continuous variables were compared using the one-way analysis of variance test (for normally distributed variables) or the Kruskal–Wallis test (for non-normally distributed variables). Bonferroni post hoc analysis was performed to assess between-group differences in case of a significant difference in the overall 3-group comparison. Categorical variables were compared using the Pearson χ^2^ test or Fischer-exact test (if the expected cell count was <5) for categorical variables. ANOVA for repeated measures was used to evaluate changes in echocardiographic variables over time for the three groups. Mortality rates are presented as Kaplan–Meier curves, and the log-rank test was used for comparisons among groups. All P values <0.05 were considered statistically significant. Data analyses were conducted using SPSS version 27 (IBM SPSS Statistics, IBM Corporation, New York) and R version 4.1.2.
Results
Successful ViV-TAVR was performed in 110 (99%) patients. Intraoperative mortality occurred in 1 patient who received a balloon-expandable valve due to rupture of the aortic valve annulus. The mechanism of valve failure was stenosis in 27 patients, regurgitation in 54 patients, and combined stenosis with regurgitation in 29 patients.
The balloon-expandable Edwards SAPIEN valve (Edwards Lifesciences, Irvine, California, USA) was used in 35 (32%, Group 1) patients, while a self-expandable valve (CoreValve, Medtronic, Minneapolis, Minnesota, USA and Portico, Abbott, Lake Bluff, Illinois, USA) was used in 76 cases. Among these cases, 39 (35%, Group 2) did not undergo balloon post-dilation, while 37 (33%, Group 3) did undergo balloon post-dilation.
Clinical and echocardiographic baseline characteristics of the entire population are presented in Table 1. The distribution of valve failure modes did not differ among the groups: Group 1 [stenosis, n = 14 (40%); regurgitation, n = 11 (41%); combined, n = 10 (29%)], Group 2 [stenosis, n = 18 (46%); regurgitation, n = 14 (36%); combined, n = 7 (18%)] and Group 3 [stenosis, n = 13 (35%); regurgitation, n = 16 (43%); combined, n = 8 (22%)]. There was no significant difference between the self-expandable and balloon-expandable valves in the rate of ViV-TAVR performed in small prosthesis [surgical valve size ≤21 mm: Group 1, 17 (51%); Group 2, 19 (53%); Group 3, 20 (57%); P = 0.886).
Baseline peak and mean transprosthetic gradients, LV volumes, ejection fraction, and pulmonary artery systolic pressure were similar among groups. A significant improvement in all echocardiographic parameters was observed in all patients over time. Specifically, a significant reduction in post-procedural transprosthetic gradients was observed at discharge and 6–12 months follow-up compared with baseline in all groups (Table 2). The gradient reduction remained consistent over time, even in patients with small surgical valves. Immediately after ViV-TAVR procedure, the lowest mean transprosthetic gradient was observed in Group 3 (12 ± 7 mmHg) compared with Group 1 and Group 2 (20 ± 9 mmHg and 17 ± 8 mmHg, respectively, P < 0.001). This result proved to be reproducible even when considering small surgical valve in all three groups, despite having higher mean transprosthetic gradients compared with larger surgical valves. Furthermore, this result was confirmed at 6–12 months follow-up (P < 0.001; Table 2).
No significant difference was found in paravalvular regurgitation rate among different SVD modes [stenosis, 2 (5%); regurgitation, 5 (14%); combined, 1 (5%); P = 0.325) at 6–12 months.
Kaplan–Meier analysis demonstrated similar outcomes up to 5 years regardless of the transcatheter valve type with or without balloon post-dilation and regardless of the mechanism of degeneration of the surgical valve (Figure 1, Table 3). No difference in mortality rate was found between small and large surgical degenerated valves (P = 0.520).
Kaplan–Meyer analysis. Kaplan–Meier curves demonstrating the event-free survival for all-cause mortality according to transcatheter valve type with or without balloon post-dilation (left panel) and mechanism of degeneration of the surgical valve (right panel).
- shows representative cases of fluoroscopy and transprosthetic gradients in Group 1, Group 2, and Group 3, respectively.
Representative cases. Fluoroscopy and continuous-wave Doppler tracings showing mean pressure gradient at baseline and discharge in a patient from Group 1 (Left Panel), Group 2 (Central Panel), and Group 3 (Right Panel).
Discussion
Until a few years ago, the best treatment of choice for prosthetic valve dysfunction has been redo surgery.^6,7^ However, patients with prosthetic aortic valve degeneration are increasingly older and have multiple comorbidities. As a result, they are not ideal candidates for redo surgery. Although ViV-TAVR may be an effective and less-invasive strategy for patients with failed surgical bioprostheses, suboptimal haemodynamic results might be a limitation of this procedure.^8–13^
This study includes a cohort of consecutive patients undergoing ViV-TAVR who were stratified into three groups: Group 1 receiving a balloon-expandable prosthesis, Group 2 receiving a self-expandable prosthesis without balloon post-dilation, and Group 3 receiving a self-expandable prosthesis with post-balloon dilatation. The main results of the study are: (i) significant improvement in all echocardiographic parameters in all groups both acutely and at follow-up; (ii) the lowest values of mean transprosthetic gradients immediately after implantation and at 6–12 months follow-up were obtained with the self-expandable prosthesis with balloon post-dilation; (iii) transcatheter valve type with or without balloon post-dilation and degeneration mode of the surgical valve were not associated with worse early and long-term all-cause mortality. However, there is a trend toward better outcomes in patients receiving a self-expandable prosthesis with balloon post-dilation.
The ViV-TAVR approach includes a highly heterogeneous group of procedures, applicable to various surgical valves with different degeneration modes.^17^ Accurate candidate assessment is crucial for optimal results, primarily based on knowledge of the failed bioprosthetic valve (model, size, structure, leaflet position, and failure mode). Another key factor is understanding the structural features and implantation techniques of transcatheter valves in relation to patient anatomy and type of surgical valve.^8,9^ Unlike previous studies,^9,18^ we observed a significant reduction in post-procedural gradients in all patients, regardless of prosthesis type. This may be influenced by improved knowledge of transcatheter valves features and implantation technique. Self-expandable valves with a supra-annular design minimize interference with the surgical valve annulus reducing transvalvular gradients, though deep deployment may lead to suboptimal haemodynamics. On the other hand, balloon-expandable valves, which are intra-annular devices, may be implanted in a higher position trying to be as ‘supra-annular’ as possible to achieve better haemodynamic.^19–21^ The significant reduction of post-procedural gradients observed in our study may have been due to the exclusion of cases with prevalent patient–prosthesis mismatch without severe bioprosthetic degeneration. Excluding patients with high transprosthetic gradients due to an effective orifice area of the surgical valve being too small in relation to body size in the absence of SVD (calcification/hypomobility of the leaflets or pannus) is essential for good haemodynamic results with ViV-TAVR. While prosthesis–patient mismatch can predispose to SVD,^22,23^ our findings suggest proper patient selection, ensuring that prosthesis–patient mismatch was not the primary dysfunction mechanism.
The absence of significant prosthetic regurgitation after ViV-TAVR is another relevant data of our study. The global registry of ViV-TAVR reported significant regurgitation in ≈5% of patients,^8^ primarily due to transcatheter valve malposition with paravalvular leak, sometimes mistaken as intravalvular regurgitation. The low rate of significant paravalvular regurgitation supports the good selection of our population, mainly due to the use of transaesophageal echocardiography during preoperative evaluation. This allowed for the exclusion of patients with both SVD and significant paravalvular leak, a condition that cannot be corrected with ViV-TAVR.
Despite the haemodynamic benefits of ViV-TAVR, some studies have shown that when small surgical valves are treated with this procedure, transvalvular gradients remain significantly increased during follow-up, even after an initial adequate reduction.^9,24^ In fact, in the PARTNER-2 study, surgical bioprosthetic valves <21 mm were exclued.^25^ Our study confirms sustained long-term gradient reduction, supporting the efficacy of the ViV-TAVR procedure regardless of the mechanism of SVD or surgical valve size, provided proper patient selection excludes prevalent patient–prosthesis mismatch. In addition, late valve thrombosis reported in ∼7% of cases may contribute to gradient elevation, though often asymptomatic.^26^ In this study, the lowest values of mean transprosthetic gradient were obtained with self-expandable prosthesis after balloon post-dilation, consistent with ex vivo bench test showing improved expansion after valve ballooning and improved residual gradients.^27^ However, high-pressure balloon inflation after ViV-TAVR may cause structural damage to the self-expanding valve frame or leaflets, resulting in severe acute regurgitation, or early and accelerated SVD. It is reassuring that we did not observe severe prosthesis regurgitation or early prosthesis degeneration up to 6–12 months follow-up in Group 3. Of course, operator experience and careful attention to balloon size and position might have played a key role in reducing the risk of these complications.
Another key finding of our study is the overall good survival across all three groups, with a trend toward better outcomes in patients receiving a self-expandable valve with balloon post-dilation, which correlates with lower transprosthetic gradients. As shown in previous studies,^18,19,28,29^ short-term survival in our cohort of patients with different transcatheter heart valves and procedure techniques was similar. In the PARTNER-2 registry,^30^ 3-year all-cause mortality was 32%, while in the CoreValve US Expanded Use Study it was 15%.^31^ Our data show an estimated mortality of 17% at 3 years, regardless of the prosthesis implanted and/or the implantation technique, which is in line with the literature. Furthermore, no differences in mortality were documented according to the underlying mechanism of dysfunction (stenosis, regurgitation, or combined). A recent study by Bleiziffer et al.^29^ reported lower survival rates in patients with failed bioprostheses having small diameters compared to those with large diameters. Indeed, a small surgical bioprostheses represents an important risk factor for mortality after ViV-TAVR. In our study, the proportion of patients with a labelled size of the surgical valve ≤21 mm was comparable among the three groups, and we found similar mortality rate in small and large degenerated surgical valves.
Limitations
Several limitations should be acknowledged. First, this is a single-centre study analysing a limited number of patients, with the inherent structural bias of the study design. Second, VIV-TAVR is performed in a heterogeneous group of patients in terms of types and sizes of surgical and transcatheter valves. Third, the choice of transcatheter valve type (balloon-expandable vs. self-expandable valve) as well as the decision to perform post-dilation were determined by operator preference.
Conclusions
In conclusion, when comparing the data from this study with the currently available literature, it is evident that the clinical and haemodynamic results of ViV-TAVR are satisfactory, and the procedure is safe and effective. Self-expandable valves with balloon post-dilation demonstrate lower post-procedural gradients, and thus this phenomenon is worthy of further investigation in a randomized controlled trial.
Several adverse events (elevated post-procedural gradients, persistent regurgitation, and thrombosis) have been described after ViV-TAVR, but they may be prevented with appropriate procedural planning, optimal prosthesis selection, increased operator experience, and novel transcatheter techniques such as ring fracture of the surgical bioprosthetic valve.
Consent
For retrospective analysis of clinically acquired data anonymously handled, the Ethical Committee waived the need of patient written informed consent.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brown JM, O'Brien SM, Wu C, Sikora JA, Griffith BP, Gammie JS. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the society of thoracic surgeons national database. J Thorac Cardiovasc Surg 2009;137:82–90.19154908 10.1016/j.jtcvs.2008.08.015 · doi ↗ · pubmed ↗
- 2Dvir D, Bourguignon T, Otto CM, Hahn RT, Rosenhek R, Webb JG et al Standardized definition of structural valve degeneration for surgical and transcatheter bioprosthetic aortic valves. Circulation 2018;137:388–99.29358344 10.1161/CIRCULATIONAHA.117.030729 · doi ↗ · pubmed ↗
- 3Kostyunin AE, Yuzhalin AE, Rezvova MA, Ovcharenko EA, Glushkova TV, Kutikhin AG. Degeneration of bioprosthetic heart valves: update 2020. J Am Heart Assoc 2020;9:e 018506.32954917 10.1161/JAHA.120.018506 PMC 7792365 · doi ↗ · pubmed ↗
- 4Christiansen S, Schmid M, Autschbach R. Perioperative risk of redo aortic valve replacement. Ann Thorac Cardiovasc Surg 2009;15:105–10.19471224 · pubmed ↗
- 5Maganti M, Rao V, Armstrong S, Feindel CM, Scully HE, David TE. Redo valvular surgery in elderly patients. Ann Thorac Surg 2009;87:521–5.19161771 10.1016/j.athoracsur.2008.09.030 · doi ↗ · pubmed ↗
- 6Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F et al 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation 2021;143:e 72–227.33332150 10.1161/CIR.0000000000000923 · doi ↗ · pubmed ↗
- 7Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J et al 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561–632.34453165 10.1093/eurheartj/ehab 395 · doi ↗ · pubmed ↗
- 8Dvir D, Webb J, Brecker S, Bleiziffer S, Hildick-Smith D, Colombo A et al Transcatheter aortic valve replacement for degenerative bioprosthetic surgical valves: results from the global valve-in-valve registry. Circulation 2012;126:2335–44.23052028 10.1161/CIRCULATIONAHA.112.104505 · doi ↗ · pubmed ↗