Benefit of splenectomy in distal pancreatectomy for neuroendocrine tumours: multicentre retrospective study
Elise Clément, Pietro Addeo, Alain Sauvanet, Célia Turco, Ugo Marchese, Safi Dokmak, Christophe Laurent, Ahmet Ayav, Olivier Turrini, Laurent Sulpice, Régis Souche, Julie Perinel, David J Birnbaum, Olivier Facy, Johan Gagnière, Lilian Schwarz, Guillaume Piessen, Nicolas Regenet

TL;DR
A study compared surgical approaches for removing pancreatic neuroendocrine tumors and found that removing the spleen during surgery does not improve outcomes.
Contribution
The study challenges the routine use of splenectomy in distal pancreatectomy for neuroendocrine tumors by showing no benefit in lymph node dissection or survival.
Findings
Splenectomy during distal pancreatectomy did not improve lymph node dissection or survival rates.
Spleen-preserving approaches had comparable safety and oncological outcomes to splenectomy.
Tumor grade and node analysis varied significantly between surgical techniques.
Abstract
Distal pancreatectomy is frequently indicated for left-sided pancreatic neuroendocrine tumour (NET). When combined lymphadenectomy is warranted, distal pancreatectomy with splenectomy (DPS) is generally advocated to optimize lymph node dissection. The spleen-preserving distal pancreatectomy (SPDP) may represent an alternative approach. This study aimed to evaluate postoperative and oncological results of distal pancreatectomy with and without splenectomy for pancreatic NET. This multicentre retrospective study included all distal pancreatectomy for pancreatic NET performed between 2014 and 2018. Patients with functional NET or multiple endocrine neoplasia type 1 were excluded. Indications and results were compared between DPS, distal pancreatectomy according to Kimura (K-SPDP) and distal pancreatectomy according to Warshaw (W-SPDP), before and after propensity score matching (PSM).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
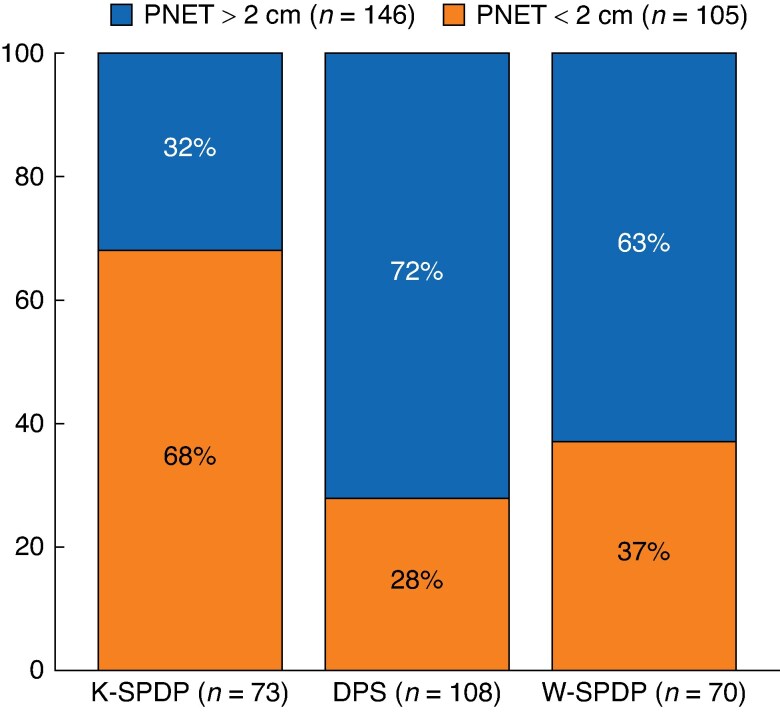 Fig. 1
Fig. 1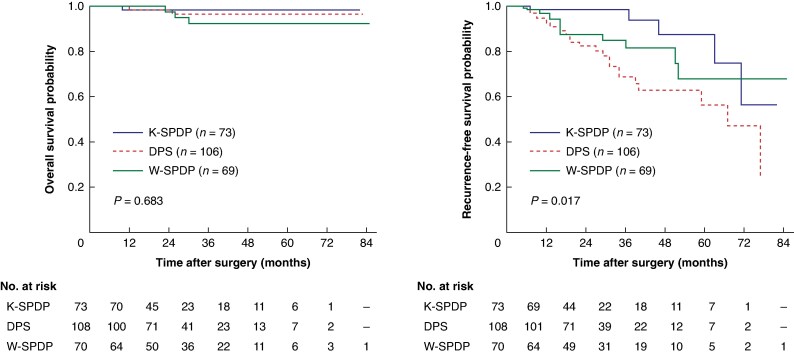 Fig. 2
Fig. 2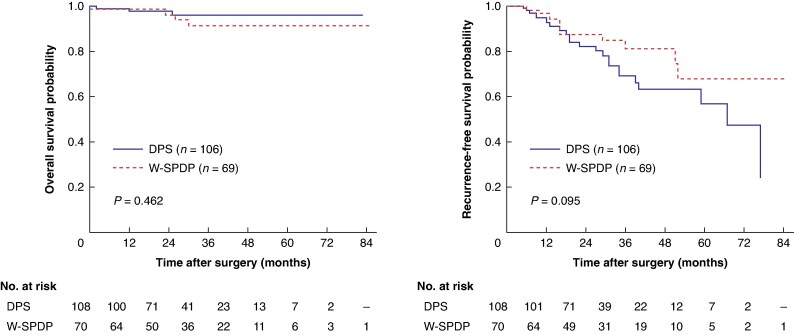 Fig. 3
Fig. 3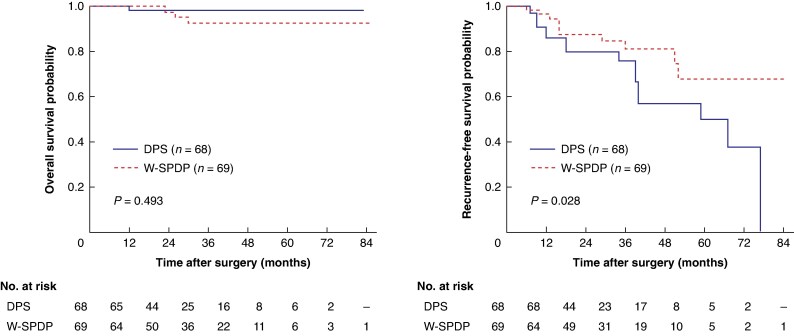 Fig. 4
Fig. 4| Overall ( | DPS ( | K-SPDP ( | W-SPDP ( |
| |
|---|---|---|---|---|---|
|
| |||||
| Age (years), median (i.q.r.) | 60 (50–67) | 62 (52–68) | 60 (52–67) | 59 (47–66) | 0.291 |
| Gender, female | 129 (51.4%) | 50 (46.3%) | 39 (53%) | 40 (57%) | 0.338 |
| BMI (kg/m2), median (i.q.r.) | 26 (23.2–29.7) | 26 (23.2–29.7) | 26.5 (23.5–29.7) | 25.7 (21.5–30) | 0.733 |
| ASA score > 2 | 21 (8.4%) | 12 (11.1%) | 5 (7%) | 4 (6%) | 0.382 |
| Diabetes mellitus | 37 (14.7%) | 15 (13.9%) | 13 (18%) | 9 (13%) | 0.668 |
| Cardiovascular disease | 16 (6.4%) | 6 (5.6%) | 4 (5%) | 6 (7%) | 0.675 |
|
| |||||
| Minimally invasive | 118 (47%) | 55 (50.9%) | 31 (42%) | 38 (54%) | 0.518 |
| Pancreatic neck section | 158 (62.9%) | 81 (75%) | 36 (49%) | 41 (59%) | 0.001 |
| Operative time (min), median (i.q.r.) | 180 (140–227) | 183 (149–240) | 164 (140–240) | 173 (120–210) | 0.080 |
| Blood transfusion | 9 (3.6%) | 5 (4.6%) | 2 (3%) | 2 (3%) | 0.741 |
| Estimated blood loss (ml), median (i.q.r.) | 200 (100–400) | 200 (100–400) | 200 (77–387) | 150 (100–400) | 0.460 |
|
| |||||
| 90-day mortality | 3 (1.2%) | 2 (1.9%) | 0 | 1 (1%) | 0.520 |
| Reintervention | 31 (12.4%) | 12 (11.1%) | 7 (10%) | 12 (17%) | 0.173 |
| 90-day Clavien–Dindo grade ≥3 | 35 (13.9%) | 14 (13%) | 8 (11%) | 13 (19%) | 0.391 |
| Clinically relevant PPH | 14 (5.6%) | 6 (5.6%) | 2 (3%) | 6 (9%) | 0.130 |
| Clinically relevant POPF | 46 (18.3%) | 21 (19.4%) | 12 (16%) | 13 (19%) | 0.875 |
| Hospital stay (days), median (i.q.r.) | 10 (8–15) | 11 (8–17) | 11 (8–15) | 9 (7–13) | 0.048 |
| Hospital readmission rate | 33 (13.1%) | 14 (13%) | 16 (22%) | 3 (4%) | 0.002 |
|
| |||||
| Tumour size (mm), median (i.q.r.) | 25 (14–40) | 30 (20–50) | 15.5 (11–24) | 25 (16–40) | <0.001 |
| Grade | 0.005 | ||||
| Grade 1 | 128 (51%) | 40 (37%) | 54 (74%) | 34 (49%) | |
| Grade 2 | 104 (41.4%) | 55 (50.9%) | 16 (22%) | 33 (47%) | |
| Grade 3 | 8 (3.2%) | 7 (6.5%) | 0 | 1 (1%) | |
| Unknown | 11 (4.4%) | 6 (5.6%) | 3 (4%) | 2 (3%) | |
| R0 resection | 236 (94%) | 98 (90.7%) | 70 (96%) | 68 (97%) | 0.154 |
| Number of retrieved lymph nodes, median (i.q.r.) | 5 (0–41) | 8 (3–13) | 1 (0–7) | 7 (1–14) | <0.001 |
| Overall ( | DPS ( | W-SPDP ( |
| |
|---|---|---|---|---|
|
| ||||
| Age (years), median (i.q.r.) | 61 (50–67) | 62 (52–68) | 59 (47–66) | 0.131 |
| Gender, female | 90 (50.6%) | 50 (46.3%) | 40 (57%) | 0.157 |
| BMI (kg/m2), median (i.q.r.) | 26 (22.9–29.7) | 26 (23.2–29.7) | 25.7 (21.5–30) | 0.838 |
| ASA score > 2 | 16 (9%) | 12 (11.1%) | 4 (6%) | 0.219 |
| Diabetes mellitus | 24 (13.5%) | 15 (13.9%) | 9 (13%) | 0.844 |
| Cardiovascular disease | 12 (6.7%) | 6 (5.6%) | 6 (7%) | 0.433 |
|
| ||||
| Minimally invasive | 87 (48.9%) | 55 (50.9%) | 38 (54%) | 0.497 |
| Pancreatic neck section | 122 (68.5%) | 81 (75%) | 41 (59%) | 0.021 |
| Operative time (min), median (i.q.r.) | 180 (140–222) | 183 (149–240) | 173 (120–210) | 0.027 |
| Blood transfusion | 7 (3.9%) | 5 (4.6%) | 2 (3%) | 0.552 |
| Estimated blood loss (ml), median (i.q.r.) | 200 (100–400) | 200 (100–400) | 150 (100–400) | 0.251 |
|
| ||||
| 90-day mortality | 3 (1.7%) | 2 (1.9%) | 1 (1%) | 0.830 |
| Reintervention | 24 (13.5%) | 12 (11.1%) | 12 (17%) | 0.250 |
| 90-day Clavien–Dindo grade ≥3 | 27 (15.2%) | 14 (13%) | 13 (19%) | 0.308 |
| Clinically relevant PPH | 12 (6.7%) | 6 (5.6%) | 6 (9%) | 0.433 |
| Clinically relevant POPF | 34 (19.1%) | 21 (19.4%) | 13 (19%) | 0.885 |
| Hospital stay (days), median (i.q.r.) | 10 (8–15) | 11 (8–17) | 9 (7–13) | 0.017 |
| Hospital readmission rate | 17 (9.6%) | 14 (13%) | 3 (4%) | 0.054 |
|
| ||||
| Tumour size (mm), median (i.q.r.) | 30 (20–45) | 28 (20–50) | 25 (16–40) | 0.162 |
| Grade | 0.205 | |||
| G1 | 74 (41.6%) | 40 (37%) | 34 (49%) | |
| G2 | 88 (49.4%) | 55 (50.9%) | 33 (47%) | |
| G3 | 8 (4.5%) | 7 (6.5%) | 1 (1%) | |
| Unknown | 8 (4.5%) | 6 (5.6%) | 2 (3%) | |
| R0 resection | 166 (93.3%) | 98 (90.7%) | 68 (97%) | 0.129 |
| Number of analysed lymph nodes, median (i.q.r.) | 7 (2–14) | 8 (3–13) | 7 (1–14) | 0.278 |
| Lymph node status | 0.065 | |||
| pN0 | 96 (53.9%) | 52 (48.1%) | 44 (63%) | |
| pN1–2 | 53 (29.8%) | 39 (36.1%) | 14 (20%) | |
| pNx | 29 (16.3%) | 17 (15.7%) | 12 (17%) | |
| Overall ( | DPS ( | W-SPDP ( |
| |
|---|---|---|---|---|
|
| ||||
| Age (years), median (i.q.r.) | 60 (50–66) | 61 (54–68) | 59 (47–66) | 0.201 |
| Gender, female | 77 (55%) | 37 (53%) | 40 (57%) | 0.386 |
| BMI (kg/m2), median (i.q.r.) | 25.8 (25.7–30) | 25.8 (23.2–29.8) | 25.7 (21.5–30) | 0.672 |
| ASA score > 2 | 10 (7.1%) | 6 (8%) | 4 (6%) | 0.327 |
| Diabetes mellitus | 21 (15%) | 12 (17%) | 9 (13%) | 0.478 |
| Cardiovascular disease | 9 (6.4%) | 3 (4%) | 6 (9%) | 0.301 |
|
| ||||
| Minimally invasive | 76 (54.3%) | 38 (54%) | 38 (54%) | 0.999 |
| Transection at the neck | 90 (64.3%) | 49 (70%) | 41 (59%) | 0.158 |
| Operative time (min), median (i.q.r.) | 180 (179–240) | 203 (148–250) | 173 (120–210) | 0.011 |
| Blood transfusion | 9 (6.4%) | 7 (10%) | 2 (3%) | 0.085 |
| Estimated blood loss (ml), median (i.q.r.) | 200 (100–400) | 200 (62–400) | 150 (100–400) | 0.436 |
|
| ||||
| 90-day mortality | 3 (2.1%) | 2 (3%) | 1 (1%) | 0.559 |
| Reintervention | 20 (14.2%) | 8 (11%) | 12 (17%) | 0.179 |
| 90-day Clavien–Dindo grade ≥3 | 23 (16.4%) | 10 (14%) | 13 (19%) | 0.278 |
| Clinically relevant PPH | 10 (7.1%) | 4 (6%) | 6 (9%) | 0.275 |
| Clinically relevant POPF | 26 (18.6%) | 13 (19%) | 13 (19%) | 0.999 |
| Hospital stay (days), median (i.q.r.) | 10 (7–15) | 10 (8–16) | 9 (7–13) | 0.066 |
| Hospital readmission rate | 17 (12.1%) | 14 (20%) | 3 (4%) | 0.004 |
|
| ||||
| Tumour size (mm), median (i.q.r.) | 27 (16–40) | 27 (25–45) | 25 (16–40) | 0.404 |
| Grade | 0.367 | |||
| G1 | 65 (46.4%) | 31 (44%) | 34 (49%) | |
| G2 | 69 (49.3%) | 36 (51%) | 33 (47%) | |
| G3 | 2 (0.1%) | 1 (1%) | 1 (1%) | |
| Unknown | 4 (0.3%) | 2 (3%) | 2 (3%) | |
| R0 resection | 132 (94.3%) | 64 (91%) | 68 (97%) | 0.145 |
| Number of analysed lymph nodes, median (i.q.r.) | 7 (2–14) | 8 (2–13) | 7 (1–14) | 0.476 |
| Lymph node status | 0.168 | |||
| pN0 | 85 (60.7%) | 41 (59%) | 44 (63%) | |
| pN1–2 | 33 (23.6%) | 19 (27%) | 14 (20%) | |
| pNx | 22 (15.7%) | 10 (14%) | 12 (17%) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Pancreatic and Hepatic Oncology Research · Gastrointestinal Tumor Research and Treatment
Introduction
Pancreatic neuroendocrine tumour (PNET) prognosis remains acceptable with median overall survival classically exceeding 10 years. Still, the presence of nodal metastases is a well-established risk factor of recurrence and decreased survival^1^. In case of left-sided grade 1 or 2 PNET larger than 2 cm without distant lesion, a distal pancreatectomy (DP) with regional lymph nodes dissection (LND) is indicated. European guidelines from the European Neuroendocrine Tumour Society do not define the type of LND for PNET^2^. Conversely, North American Neuroendocrine Tumor Society guidelines are rather centred on the quality of the dissection with a recommended number of lymph nodes ranging between 11 and 15, without recommending clearly which technique should be preferred^3^. The splenic preservation during DP may be technically demanding, could be associated with post-pancreatectomy haemorrhage or spleen infarction, and may also limit nodal retrieval. The spleen preserving distal pancreatectomy (SPDP) may preserve patients’ innate immune responses and some have argued that it is associated eith fewer complications than distal splenopancreatectomy (DPS)^4–6^. Further, although the lymphatic drainage pathway of the pancreatic body and tail is mostly directed towards the coeliac trunk, there are no data warranting routine splenectomy for left-sided PNET resection.
The current study aimed to evaluate the impact of DP techniques for non-functional PNET in terms of short- and long-term outcomes and on LND.
Methods
Study population
This was a retrospective and multicentre study carried out in high-volume referral centres, defined as those performing more than 20 pancreatectomies per year^7^. Patients aged ≥18 years were included if they underwent elective distal pancreatectomy for PNET, between 2014 and 2018, with or without spleen preservation, with open or minimally invasive approach. Patients who underwent DP in the setting of multiple endocrine neoplasia type 1 (MEN1), functioning PNETs, and extended DP as defined by the International Study Group for Pancreatic Surgery (ISGPS) were excluded^8^. Different DP techniques were defined as DPS (harvesting all lymph nodes along splenic vessels including those at the splenic hilum), SPDP with splenic vessels preservation according to the Kimura technique (K-SPDP, harvesting lymph nodes along the splenic vessels while preserving those vessels), and SPDP with splenic vessels resection according to the Warshaw technique (W-SPDP, harvesting all lymph nodes with resected splenic vessels while leaving in place those at the splenic hilum)^9,10^.
Data collection
Demographic and baseline characteristics regarding patients and tumour features were collected. Intraoperative variables (type of surgical approach, operative time, estimated blood loss, spleen preservation techniques), data on final pathology (tumour size, tumour grade, nodal status, and resection margin) were also retrieved. Complete resection (R0) margin was defined as surgical margin larger than 1 mm. Postoperative mortality and morbidity rates within 90 days were recorded according to the Clavien–Dindo classification with severe morbidity rate corresponding to morbidity grade greater than 2^11^. Pancreas-specific postoperative complications including postoperative pancreatic fistula (POPF), delayed gastric emptying, and post-pancreatectomy haemorrhage (PPH) were defined according to ISGPS definitions^12–14^. Similarly, clinically relevant splenic complications defined as splenic ischaemia or haemorrhage requiring reoperation for splenectomy were collected. In case of postoperative complication, reintervention was defined as either involving interventional radiology, endoscopy, or surgery. Reason for any reintervention was monitored. Oncological follow-up with data concerning tumour recurrence and overall survival were also collected.
Management and outcomes
All patients were managed according to national guidelines and decision for DP was discussed at dedicated multidisciplinary tumour boards in each centre^15^. Preoperative work-up comprised systematically thoracoabdominal CT, liver magnetic resonance imaging, and ^68^Ga-DOTATATE PET/CT to detect regional and distant metastases. Decision for indication and techniques of spleen preservation was at the discretion of the primary surgeon at each centre.
Statistics analysis
Categorical variables, presented as numbers and percentages, were compared using the χ^2^ test. Continuous variables with a normal distribution are presented as mean(s.d.) and non-normally distributed variables as median (i.q.r.), and were compared using the Kruskal–Wallis test. Comparisons between resection types were performed regarding preoperative and intraoperative data and postoperative outcomes in the full cohort. Additionally, due to obvious differences between patients who underwent K-SPDP and those in both the W-SPDP and DPS groups, patients in the W-SPDP group were compared to those undergoing DPS, before and after matching using the propensity score matching (PSM) method. The propensity score for an individual was calculated using a multivariable logistic regression model including the following variables: age, gender, body mass index, ASA score, tumour size, and tumour grade. Using a standard calliper width of 0.2, patients were matched without replacement to the closest matching propensity score in a 1 : 1 ratio.
Patients who died within 90 days after surgery were excluded from survival analysis. Overall survival (OS) was calculated from the date of resection to the date of death, or the date of last follow-up, and recurrence-free survival (RFS) was calculated from the date of resection to the date of first recurrence, the date of death, or last follow-up. OS and RFS were estimated using the Kaplan–Meier method and compared between groups using the Log-rank test. Two-tailed P < 0.05 were considered statistically significant. Statistical analyses were carried out using SPSS Statistics 27.0 (IBM). The present study complied with the RECORD guidelines^16^.
Results
Study population
Over the study period, 272 patients were operated for PNETs in 21 hospitals, of whom 16 patients with MEN1 and 5 patients with functioning PNETs were excluded. Of 251 patients included in the study, 108 (43%) underwent DPS, 73 (29.1%) K-SPDP, and 70 (27.9%) W-SPDP (Fig. S1). Patients’ characteristics, tumour features, and perioperative outcomes are listed in Table 1. Overall, 133 resections (53%) were performed minimally invasively including 110 laparoscopic resections and 23 robotic resections. Conversion rate was 9% (n = 12) and reasons for conversion to open surgery were exposure difficulty (n = 7) and intraoperative bleeding (n = 5). Following surgery, 90-day mortality and severe morbidity rates were 1.2% (n = 3) and 13.9% (n = 35) respectively. Clinically relevant POPF and PPH rates were 18.3% (n = 46) and 5.6% (n = 14) respectively and 31 patients (12.4%) required reintervention. One patient experienced clinically relevant splenic complication requiring rescue splenectomy 11 days after W-SPDP, in the setting of POPF combined with PPH and arterial embolization failure. Median length of hospital stay was 10 days (range 4–242). Readmission rate was 13.1% (n = 33). Regarding tumour features, median tumour size was 25 mm (i.q.r. 15–40). The majority of PNET (92.4%, n = 232) were G1 or G2. R0 resection rate was 94% (n = 236).
Differences according to resection types
There was no difference in terms of patients’ characteristics and surgical approach between the three types of resections. Intraoperatively, pancreatic transection at the neck was significantly more frequently performed in case of DPS (P < 0.001). Following surgery, there was no difference regarding mortality and severe morbidity rates, except in terms of median hospital stay (P = 0.048) and readmission rate (P = 0.002). Tumour features were significantly different according to the type of resection. Tumours were significantly smaller in patients who underwent K-SPDP (median: 15.5 mm, i.q.r. 11–24) as compared to those in the W-SPDP (median: 25 mm, i.q.r. 16–40) or DPS (30 mm, i.q.r. 20–50) groups respectively (P < 0.001). Considering a 2-cm size cut-off, K-SPDP was mostly performed for PNET <2 cm whereas both W-SPDP and DPS were performed for PNET >2 cm (P < 0.001; Fig. 1). Similar differences were observed regarding tumour grade, with 74% (n = 54) of G1 PNET in K-SPDP patients as compared to those in the W-SPDP (48.6%, n = 34) or DPS (37%, n = 40) groups respectively (P = 0.005).
Distribution of tumour size according to the type of resection
With respect to lymph node dissection, at least one lymph node could be examined in 95 patients (88%) who underwent DPS, 58 patients (82.9%) who underwent W-SPDP, and 37 patients (50.7%) after K-SPDP (P < 0.001). When lymph node dissection was carried out (n = 190, 75.7%), there was a significant difference in the median number of harvested lymph nodes between DP types (P < 0.001). Among patients with at least one retrieved lymph nodes, 56 patients (29.5%) had nodal disease. Nodal disease was associated with tumour size (pN0 = 22 mm, i.q.r. 15–35; pN1 = 40 mm, i.q.r. 25–50; P < 0.001).
Regarding long-term outcomes (Fig. 2), median follow-up was 24 months (i.q.r. 16–41). There was no difference in terms of OS (P = 0.683) whereas there was a statistically significant difference in median RFS estimates (DPS = 64 months, W-SPDP = not reached, K-SPDP = not reached; P = 0.017).
Overall and recurrence-free survival estimates in the whole cohort (n = 251)
Comparison between W-SPDP and DPS
After excluding patients who underwent K-SPDP, patients who underwent W-SPDP (n = 70) were compared to those with DPS (n = 108) before PSM (Table 2). No statistically significant difference between the two groups was demonstrated except regarding operative time (P = 0.027) and length of hospital stay (P = 0.017) that were shorter in the W-SPDP group. There was no difference observed in terms of tumour size (P = 0.162) or tumour grade (P = 0.205). Similarly, there was no difference regarding R0 resection rate (P = 0.129) and the number of retrieved lymph nodes (P = 0.278). Regarding survival data, there was no difference in terms of OS (P = 0.462) and RFS (P = 0.095) between DP (Fig. 3).
Overall and recurrence-free survival estimates in patients who underwent DPS or W-SPDP before propensity score matching
After PSM, patients who underwent W-SPDP (n = 70) were compared to those with DPS (n = 70) (Table 3). Overall, there was no difference regarding all perioperative variables except regarding operative time (P = 0.011). Regarding survival data, there was no difference in terms of overall survival (P = 0.493), but median RFS was shorter in the DPS group (59 months) as compared to the W-SPDP group (not reached; P = 0.028) (Fig. 4).
Overall and recurrence-free survival estimates in patients who underwent DPS or W-SPDP after propensity score matchingDPS, distal pancreatectomy with splenectomy; W-SPDP, Warshaw spleen-preserving distal pancreatectomy.
Discussion
In the current series, there was an obvious difference in the indications of distal pancreatectomy with or without spleen preservation techniques. K-SPDP was mostly performed in patients with smaller PNET, mostly G1, irrespective of patients’ characteristics. Pancreatic section was significantly more frequently performed at the neck in case of DPS, despite the absence of difference in terms of tumour location between groups. There was no difference in terms of mortality and severe morbidity rates between the three techniques and there was only a marginal difference in terms of length of hospital stay and readmission rate, favouring W-SPDP.
DPS is generally seen as the technique of choice for the sake of oncological radicality, especially regarding lymph nodes dissection. Regarding the PNET, Sahara and colleagues showed spleen preservation as associated with comparable or even better perioperative outcomes than DPS^17^, including patients operated at expert centres performing only W-SPDP. They concluded that W-SPDP might be better considered in selected cases, such as PNET <2 cm, centrally located in the pancreas. And SPDP should be avoided in tumours invading the splenic vessels or with suspicious lymph nodes in the splenic hilum. In the current study, there was no difference in terms of OS between W-SPDP and DPS. Nevertheless, there was a trend towards longer RFS in the W-SPDP group as compared to DPS before PSM, and this difference became statistically significant after PSM. Although long-term follow-up limited to a median time of 24 months should restrict any conclusion on long-term oncological outcomes, one could hypothesize that such a difference may be related to the potential immune preservation in the W-SPDP group^18^. At least, the absence of a survival advantage in the DPS group may suggest that splenectomy does not confer any oncological advantage in the surgical management of left-sided PNET. Future studies should be focused on long-term survival.
Regarding surgical quality, there was no difference in terms of R0 resection rates and regarding the median number of retrieved lymph nodes between W-SPDP and DPS. Although lymph nodes metastases are related to adverse tumour features, the relevance of lymphadenectomy in PNET management remains disputed^19–23^. According to current guidelines, lymphadenectomy is routinely recommended for PNET >3 cm and/or G2 PNET^3^. In such a situation, W-SPDP could rather be considered as a safe alternative to DPS, especially for tumours located at the body of the pancreas, with no suspected lymph nodes on preoperative imaging.
Several points of limitation need to be addressed. The current study design and retrospective nature imply potential bias. For instance, besides missing histological data such as vascular invasion and perineural invasion, other data were lacking. Mostly, reasons driving the choice of each surgical technique would have been of interest. Indeed, such a choice might have been driven by surgeon preference, patient characteristics, or tumour features. As previously mentioned, given the limited duration of follow-up, long-term outcomes analysis should be carefully interpreted. Many left-sided PNET can also be removed using parenchyma-sparing resection such as enucleation or central pancreatectomy to reduce postoperative pancreatic insufficiency^24,25^. As such, the whole story of left-sided PNET management is not fully captured in the present cohort. K-SPDP is classically indicated for small PNET, when routine lymphadenectomy is not warranted^26^. In the current study, K-SPDP was mostly performed in patients with significantly smaller PNET and more frequently G1 as compared to W-SPDP and DPS patients. Conversely, Warshaw and DPS were performed in patients with more advanced tumour features, similar in terms of tumour size and grade between both techniques. Consequently, the current study focused on differences between W-SPDP and DPS. Further studies would be justified to determine the adequate SPDP technique for small PNET. Another key limitation of the study was the low number of retrieved lymph nodes which limited the analysis on the nodal disease. However, this number was quite similar to those reported in existing series for PNET or intraductal papillary mucinous neoplasm^17,27^.
In conclusion, SPDP could be routinely considered as an option for left-sided PNET. In situations warranting lymphadenectomy and in the absence of spleen involvement, W-SPDP could stand as a safe alternative to DPS. Like prospective studies in pancreatic ductal adenocarcinoma, the added value of splenectomy during DP for PNET would have to be defined based on oncological criteria such as the rate of splenic hilum lymph node metastasis and survival outcomes^28^.
Collaborators
Mustapha Adham, Marie André, Philippe Bachellier, Louise Barbier, Thomas Bardol, Zineb Cherkaoui, Thibault Durin, David Fuks, Zaher Lakkis, Cloé Magallon, Fabien Robin, Edouard Roussel, Ecoline Tribillon, Stéphanie Truant, and Stylianos Tzedakis
Supplementary Material
zraf038_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE et al One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;26:3063–307218565894 10.1200/JCO.2007.15.4377 · doi ↗ · pubmed ↗
- 2Kos-Kudla B, Castano JP, Denecke T, Grande E, Kjaer A, Koumarianou A et al European Neuroendocrine Tumour Society (ENETS) 2023 guidance paper for nonfunctioning pancreatic neuroendocrine tumours. J Neuroendocrinol 2023;35:e 1334337877341 10.1111/jne.13343 · doi ↗ · pubmed ↗
- 3Howe JR, Merchant NB, Conrad C, Keutgen XM, Hallet J, Drebin JA et al The North American Neuroendocrine Tumor Society consensus paper on the surgical management of pancreatic neuroendocrine tumors. Pancreas 2020;49:1–3331856076 10.1097/MPA.0000000000001454 PMC 7029300 · doi ↗ · pubmed ↗
- 4Hang K, Zhou L, Liu H, Huang Y, Zhang H, Tan C et al Splenic vessels preserving versus Warshaw technique in spleen preserving distal pancreatectomy: a systematic review and meta-analysis. Int J Surg 2022;103:10668635605839 10.1016/j.ijsu.2022.106686 · doi ↗ · pubmed ↗
- 5Kristinsson SY, Gridley G, Hoover RN, Check D, Landgren O. Long-term risks after splenectomy among 8,149 cancer-free American veterans: a cohort study with up to 27 years follow-up. Haematologica 2014;99:392–39824056815 10.3324/haematol.2013.092460 PMC 3912973 · doi ↗ · pubmed ↗
- 6Zhou ZQ, Kim SC, Song KB, Park KM, Lee JH, Lee YJ. Laparoscopic spleen-preserving distal pancreatectomy: comparative study of spleen preservation with splenic vessel resection and splenic vessel preservation. World J Surg 2014;38:2973–297924968894 10.1007/s 00268-014-2671-3 · doi ↗ · pubmed ↗
- 7El Amrani M, Clement G, Lenne X, Farges O, Delpero JR, Theis D et al Failure-to-rescue in patients undergoing pancreatectomy: is hospital volume a standard for quality improvement programs? Nationwide analysis of 12,333 patients. Ann Surg 2018;268:799–80730048329 10.1097/SLA.0000000000002945 · doi ↗ · pubmed ↗
- 8Hartwig W, Vollmer CM, Fingerhut A, Yeo CJ, Neoptolemos JP, Adham M et al Extended pancreatectomy in pancreatic ductal adenocarcinoma: definition and consensus of the International Study Group for Pancreatic Surgery (ISGPS). Surgery 2014;156:1–1424856668 10.1016/j.surg.2014.02.009 · doi ↗ · pubmed ↗