Nap duration and its association with hypertension-diabetes comorbidity in minority populations: evidence from the CMEC study
Renhua Zhang, Enhui Zhou, Leilei Liu, Yuan Wang, Fei Xiao, Feng Hong

TL;DR
The study found that longer nap durations are linked to a higher risk of having both hypertension and diabetes in minority populations in China.
Contribution
This study is the first to explore the association between nap duration and hypertension-diabetes comorbidity in minority populations using the CMEC dataset.
Findings
Longer nap durations were associated with increased odds of hypertension-diabetes comorbidity.
The relationship between nap duration and comorbidity varied by age group, showing linear and inverse J-shaped patterns.
Subgroup analyses revealed higher risk in males, older individuals, and specific ethnic groups.
Abstract
Limited information is available on the effect of nap duration and hypertension-diabetes comorbidity (HDC) in minority people. We aimed to explore the relationship between nap duration and HDC for the co-management of hypertension and diabetes mellitus in the minority. A total of 16,911 participants from the China Multi-Ethnic Cohort (CMEC) were enrolled in this cross-sectional study. Nap duration was then categorized into four groups: 0 hours (reference group), 0–0.5 hours, 0.5–1 hour, and >1 hour. Multiple logistic regression was applied to analyze the association between nap duration and HDC. Restricted cubic splines (RCS) analysis was conducted to assess the nonlinear relationship between nap duration and the co-occurrence of HDC. Subgroup analyses were subsequently performed, stratified by sex, age, and ethnicity. Among 16,911 participants with a median age of 51.79 years, of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
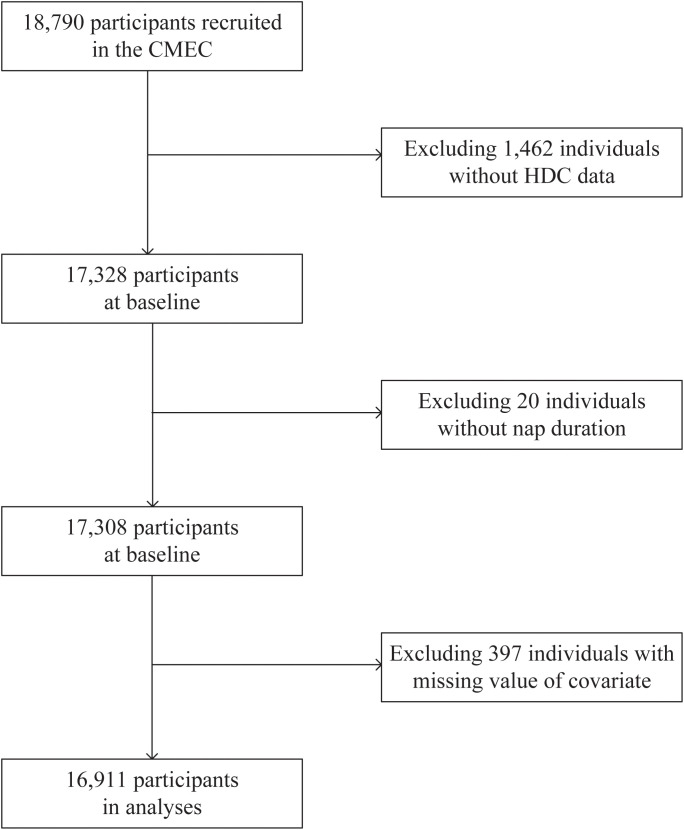 Figure 1
Figure 1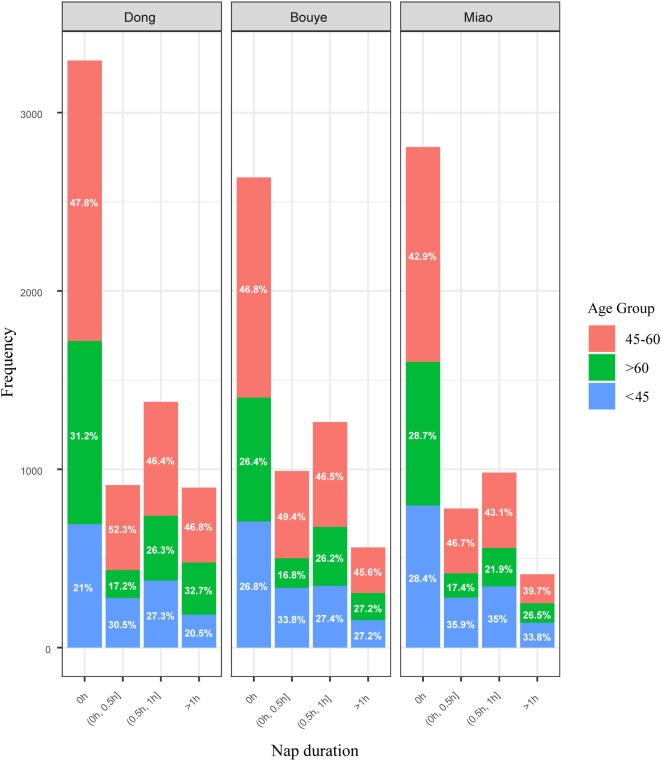 Figure 2
Figure 2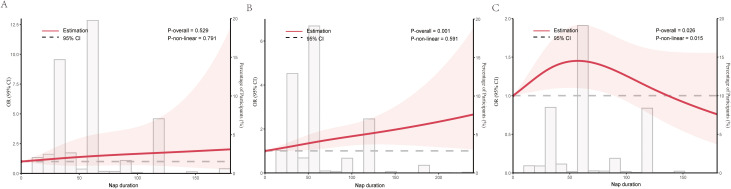 Figure 3
Figure 3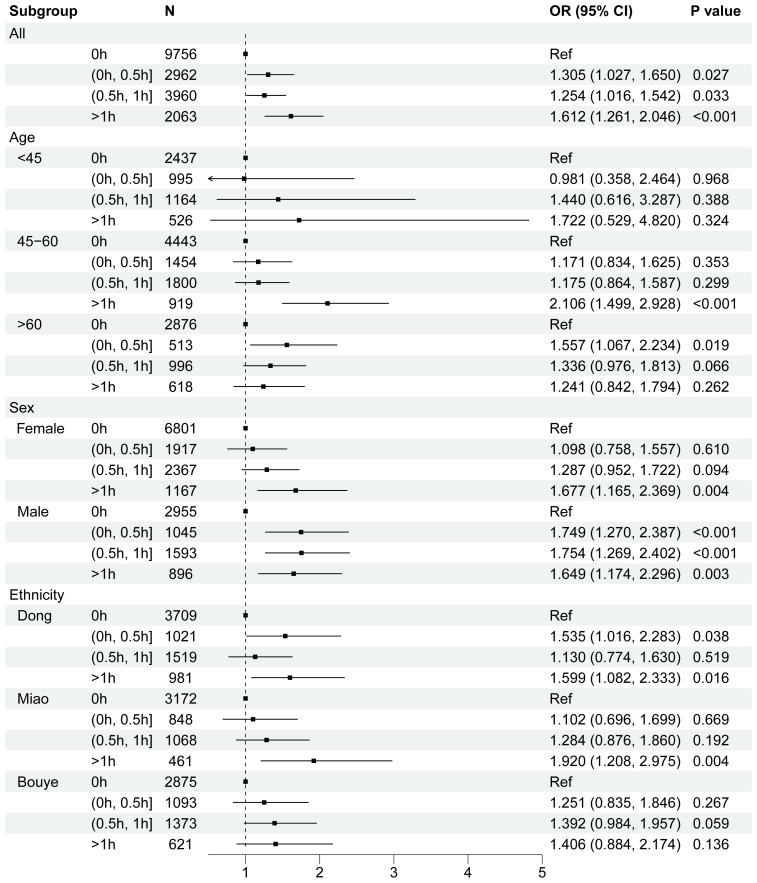 Figure 4
Figure 4| Overall | 0h | (0h, 0.5h] | (0.5h, 1h] | >1h |
| |
|---|---|---|---|---|---|---|
| N | 16911 | 8736 | 2681 | 3624 | 1870 | |
| Age, median (IQR) | 51.79 [44.27, 60.66] | 52.67 [44.96, 61.86] | 49.28 [43.00, 55.77] | 51.01 [43.71, 60.10] | 52.49 [44.81, 61.82] | <0.001 |
| Sex, n (%) | <0.001 | |||||
| Male | 5750 (34.00) | 2585 (29.59) | 937 (34.95) | 1437 (39.65) | 791 (42.30) | |
| Female | 11161 (66.00) | 6151 (70.41) | 1744 (65.05) | 2187 (60.35) | 1079 (57.70) | |
| Ethnicity, n (%) | <0.001 | |||||
| Dong | 6478 (38.31) | 3292 (37.68) | 911 (33.98) | 1378 (38.02) | 897 (47.97) | |
| Bouyei | 5454 (32.25) | 2637 (30.19) | 990 (36.93) | 1265 (34.91) | 562 (30.05) | |
| Miao | 4979 (29.44) | 2807 (32.13) | 780 (29.09) | 981 (27.07) | 411 (21.98) | |
| Residence, n (%) | <0.001 | |||||
| Rural | 13381 (79.13) | 7394 (84.64) | 1779 (66.36) | 2632 (72.63) | 1576 (84.28) | |
| Urban | 3530 (20.87) | 1342 (15.36) | 902 (33.64) | 992 (27.37) | 294 (15.72) | |
| Annual household | <0.001 | |||||
| <100000 CNY | 15440 (91.30) | 8176 (93.59) | 2278 (84.97) | 3218 (88.80) | 1768 (94.55) | |
| 100000-199999 CNY | 1315 ( 7.78) | 497 ( 5.69) | 365 (13.61) | 364 (10.04) | 89 ( 4.76) | |
| ≥200000 CNY | 156 ( 0.92) | 63 ( 0.72) | 38 ( 1.42) | 42 ( 1.16) | 13 ( 0.70) | |
| Central obesity, n (%)a | 0.584 | |||||
| No | 5538 (32.75) | 2868 (32.83) | 899 (33.53) | 1180 (32.56) | 591 (31.60) | |
| Yes | 11373 (67.25) | 5868 (67.17) | 1782 (66.47) | 2444 (67.44) | 1279 (68.40) | |
| Smoke, n (%) | <0.001 | |||||
| Never | 13531 (80.01) | 7225 (82.70) | 2214 (82.58) | 2755 (76.02) | 1337 (71.50) | |
| Current | 2754 (16.29) | 1240 (14.19) | 371 (13.84) | 707 (19.51) | 436 (23.32) | |
| Ever | 626 ( 3.70) | 271 ( 3.10) | 96 ( 3.58) | 162 ( 4.47) | 97 ( 5.19) | |
| Alcohol, n (%) | <0.001 | |||||
| Never | 8627 (51.01) | 4804 (54.99) | 1232 (45.95) | 1711 (47.21) | 880 (47.06) | |
| Occasionally | 6256 (36.99) | 3030 (34.68) | 1153 (43.01) | 1414 (39.02) | 659 (35.24) | |
| Frequently | 2028 (11.99) | 902 (10.33) | 296 (11.04) | 499 (13.77) | 331 (17.70) | |
| Salt intake, median (IQR) | 49.71 [34.52, 69.04] | 51.40 [34.52, 69.04] | 48.33 [34.25, 68.08] | 49.32 [34.52, 69.04] | 53.70 [38.07, 76.32] | <0.001 |
| Physical activity, n (%)b | <0.001 | |||||
| Low | 5598 (33.10) | 2765 (31.65) | 897 (33.46) | 1252 (34.55) | 684 (36.58) | |
| Moderate | 5659 (33.46) | 2861 (32.75) | 928 (34.61) | 1251 (34.52) | 619 (33.10) | |
| High | 5654 (33.43) | 3110 (35.60) | 856 (31.93) | 1121 (30.93) | 567 (30.32) | |
| Sleep duration, median (IQR) | 7.00 [6.00, 8.00] | 7.00 [6.00, 8.00] | 7.00 [6.00, 8.00] | 7.00 [6.00, 8.00] | 7.00 [6.00, 8.00] | <0.001 |
| Sleep disorder, n (%) | <0.001 | |||||
| 0 | 9047 (53.50) | 4553 (52.12) | 1497 (55.84) | 1999 (55.16) | 998 (53.37) | |
| 1 | 3326 (19.67) | 1747 (20.00) | 467 (17.42) | 728 (20.09) | 384 (20.53) | |
| 2 | 2977 (17.60) | 1575 (18.03) | 469 (17.49) | 585 (16.14) | 348 (18.61) | |
| 3 | 1561 ( 9.23) | 861 ( 9.86) | 248 ( 9.25) | 312 ( 8.61) | 140 ( 7.49) | |
| HDC, n (%) | <0.001 | |||||
| No | 16264 (96.17) | 8459 (96.83) | 2570 (95.86) | 3468 (95.70) | 1767 (94.49) | |
| Yes | 647 ( 3.83) | 277 ( 3.17) | 111 ( 4.14) | 156 ( 4.30) | 103 ( 5.51) |
| Nap duration | N | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
| ||
| 0h | 9756 | Ref | Ref | Ref | |||
| (0h, 0.5h] | 2962 | 1.318 (1.052, 1.639) | 0.015 | 1.553 (1.235, 1.941) | <0.001 | 1.305 (1.027, 1.650) | 0.027 |
| (0.5h, 1h] | 3960 | 1.361 (1.114, 1.655) | 0.002 | 1.386 (1.132, 1.691) | 0.001 | 1.254 (1.016, 1.542) | 0.033 |
| >1h | 2063 | 1.768 (1.402, 2.214) | <0.001 | 1.638 (1.293, 2.061) | <0.001 | 1.612 (1.261, 2.046) | <0.001 |
- —National Key Research and Development Program of China 10.13039/501100012166
- —National Natural Science Foundation of China 10.13039/501100001809
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity, Physical Activity, Diet · Sleep and related disorders
Introduction
Napping, or the practice of taking a short daytime sleep, has become an integral part of daily life, particularly in many Asian countries, including China. The prevalence of napping among Chinese adults increases with age, with 61.7% of males and 46.8% of females aged 60 and above reporting a habitual napping behavior (1). Napping is often regarded as a healthy lifestyle practice that contributes to improved mental well-being (2).However, as lifestyles modernize, the duration of napping have become more varied, with some individuals napping for longer durations (3). Emerging research suggests that napping may influence the development of chronic diseases. While short naps are generally associated with improved cognitive function, mental health, and cardiovascular outcomes (4–6), prolonged or irregular napping patterns are linked to a higher risk of developing chronic conditions such as hypertension and diabetes (7, 8). Disrupted sleep patterns, which include excessive daytime sleep, may interfere with circadian rhythms and lead to metabolic disturbances (9).
Hypertension and diabetes are major non-communicable diseases and significant global public health challenges (10). Although they are separate conditions, they frequently coexist, and patients with comorbid hypertension and diabetes face a heightened risk of cardiovascular disease (CVD) and cognitive impairment (CI) that exceeds the sum of the risks associated with either condition alone (11, 12). According to a meta-analysis, the prevalence of hypertension-diabetes comorbidity (HDC) in China has shown an upward trend, reaching 8.7% among adults (13). Notably, racial disparities in the prevalence of multimorbidity may stem from distinct cultural practices and lifestyle habits among ethnic minorities (14). In China’s northwestern regions, the prevalence of HDC among adults is 4.58% (15), while in the eastern coastal regions, among community-dwelling elderly individuals aged 65 and older, the comorbidity rate is 12.5% (16). However, studies examining the prevalence and associated factors of HDC in socioeconomically disadvantaged regions remain limited. Furthermore, ethnic minorities such as the Dong, Miao, and Bouyei in southwestern China face even greater challenges in managing hypertension and diabetes. Compared to urban patients, these ethnic minorities, predominantly residing in rural areas, encounter significant barriers to accessing local health services due to high travel costs and limited healthcare availability (17).
To date, in China, particularly in the southwestern region, no large-scale studies have specifically investigated the association between nap duration and HDC. Instead, most research has primarily focused on individual diseases. It is essential to explore how nap duration could influence the development and progression of co-existence diseases. This study aims to investigate the relationship between nap duration and hypertension-diabetes comorbidity, using epidemiological methods to examine how nap duration may affect metabolic processes and contribute to the risk of these diseases. By focusing on the metabolic health impacts of napping, this research seeks to provide new insights into the prevention and management of hypertension-diabetes comorbidity.
Methods
Study design and participants
We conducted a population-based prospective study among three main ethnic minorities in the southwest China, including the Bouyei, Dong, and Miao, aged 30 to 79 years. The data used in this study were derived from the baseline survey conducted in the China Multi-Ethnic Cohort Study from July 2018 to August 2019. Detailed information about the study population has been previously described (18).
Exclusion criteria: 1) participants without basic information; 2) participants who did not self-report hypertension or diabetes and did not undergo laboratory testing; 3) incomplete data on key variables such as nap duration. Figure 1 illustrates the details of the participant enrollment process. Finally, a total of 16,911 individuals were included in this analysis. Each participant completed electronic questionnaires through face-to-face interviews and underwent physical examinations and clinical laboratory tests. This study was approved by the Medical Ethics Review Committee of Sichuan University (K2016038) and the Research Ethics Committee of The Affiliated Hospital of Guizhou Medical University (2018[094]), and all methods were performed in accordance with relevant guidelines and regulations. Written informed consent was obtained from each participant before study initiation.
Flowchart of study participants.
Exposure – self-reported duration of daytime napping
Participants were first asked whether they had a habit of napping. If they answered yes, they were further asked: “How long, on average (in minutes), do you usually nap after lunch?” Based on their responses to these two questions, participants were categorized into four groups: no daytime napping (0 min/day), short daytime napping (1–30 min/day), moderate daytime napping (31–60 min/day), and long daytime napping (>60 min/day) (19).
Outcome – HDC
In this study, diabetes was defined as meeting any of the following criteria: (1) self-reported physician-diagnosed diabetes, (2) fasting plasma glucose (FPG) ≥ 7.0 mmol/L or glycosylated hemoglobin (HbA1c) ≥ 6.5%. Hypertension was defined as: (1) self-reported physician-diagnosed hypertension, or (2) systolic blood pressure (SBP) ≥ 140 mmHg or diastolic blood pressure (DBP) ≥ 90 mmHg. HDC was defined as the coexistence of both hypertension and diabetes.
Covariates
Face-to-face structured questionnaires were used to collect demographic information and lifestyle factors, including demographics (sex, age, and ethnicity), socioeconomic gradient (residence and annual household income), health behaviors (smoking (20), alcohol consumption (21), physical activity, duration of night sleep, sleep disorder), central obesity and salt intake per day. Physical activity considered participants’ occupational, traffic, chores, and leisure time activities, and were divided into low and high based on the median value of metabolic equivalent for task (MET).Night sleep duration and sleep disorders were classified into three types of insomnia based on participants’ responses to the following questions: (1) Disorders of Initiation and Maintenance (DIMS): defined as taking more than 30 minutes to fall asleep at least three days per week; (2) Early Morning Awakening (EMA): defined as waking up early in the morning and being unable to fall back asleep at least three days per week; (3) Daytime Dysfunction (DDF): defined as difficulty staying awake during the day while working, eating, or talking to others at least three days per week. The total number of insomnia types reported by each participant was summed and categorized as follows: 0 (none), 1 (any one type), 2 (any two types), and 3 (all three types) (22).
Statistical analysis
The baseline demographic characteristics of the participants were described according to the four levels of nap duration (no nap, ≤30 min, 31–60 min, and >60 min). The Kolmogorov–Smirnov (K–S) test was used to assess the normality of continuous variables. Normally distributed continuous variables were presented as mean ± standard deviation (SD), while non-normally distributed variables were summarized as mean (SD) and median (25th, 75th percentiles). Categorical variables were expressed as frequency counts and percentages. Group comparisons for continuous variables were performed using the Kruskal–Wallis H test, and the Chi-square test was used for categorical variables. Restricted cubic spline (RCS) analysis was employed to explore the nonlinear relationship between nap duration and the risk of hypertension-diabetes comorbidity (HDC). Multiple logistic regression analyses were used to evaluate the associations between nap duration and HDC. Model 1 was an unadjusted crude model. In Model 2, we adjusted for sex, age, ethnicity. Model 3 further adjusted for central obesity, smoking status, alcohol consumption, annual household income, physical activity, salt intake, night sleep duration, and night sleep disorders based on Model 2. In addition, in different age groups (<45 years, 45–60 years, and >60 years), restrictive cubic splines (RCS) were used to describe the potential relationship between nap duration and HDC risk (23). Subgroup analyses were conducted to explore the potential modifiers of the association between nap duration and HDC, stratified by sex, age (<45 years, 45–60 years, and >60 years), and ethnicity (Dong, Miao, and Bouyei). All statistical analyses were performed using R software (version 4.3.1). A two-sided P-value < 0.05 was considered statistically significant.
Results
Population characteristics
The data presented in Figure 2 indicates “0 h” is the most common nap duration, with proportions decreasing as nap time increases across all groups. The 45–60 age group dominates most categories, particularly in longer nap durations, while the <45 group shows a higher proportion in shorter naps. Variations in nap patterns reflect differences across ethnicities and age groups.
Distribution of different ethnic groups and age groups across various nap duration categories.
The study, which involved 16,911 participants classified by nap duration into groups of no nap (0h), naps between 0 and 0.5 hours, 0.5 to 1 hour, and greater than 1 hour, revealed several key trends. The detailed data are presented in Table 1. Regarding age and sex, participants with longer nap durations were generally older, and the proportion of males was higher in these groups compared to those with no or shorter naps. In terms of ethnicity and residence, ethnic distribution varied across nap - duration groups, with the Dong ethnic group more common in longer - nap groups, and participants from rural areas were more likely to have no nap or longer naps. Considering socio - economic factors, individuals with lower household incomes were more prone to report longer nap durations, especially the lowest - income group in the no - nap and >1h nap categories. For lifestyle factors, longer nap durations were associated with lower physical activity levels, increased alcohol consumption, higher salt intake, and a greater likelihood of sleep disorders. Finally, in relation to health outcomes, the prevalence of HDC was higher among those with longer nap durations, suggesting a potential link between longer naps and an increased risk of chronic disease.
Observational analyses of nap duration on HDC
The results of nap duration and HDC in Multiple logistic regression are shown in Table 2. In the crude model, long nap duration(>1h) (OR = 1.768, 95% CI: 1.402, 2.214; P < 0.001) had significantly higher risk of HDC compared to those who slept in daytime at all. The positive association of nap duration and HDC was still statistically significant though attenuated after adjusting for age, sex, ethnicity, residence, annual household income, central obesity, smoke, drink, salt intake, physical activity, night sleep duration, night sleep disorder (OR = 1.638, 95% CI: 1.293, 2.061; P < 0.001). Further adjustment of chronotype and snoring did not change the positive association between nap duration group and HDC (OR = 1.612, 95% CI: 1.261, 2.046; P < 0.001).
Dose–response relationship between nap duration and HDC in different age group
Participants were stratified into three age groups: 30–45, 45–60, and 60–80 years (20). In the group aged <45 years, no significant nonlinear association was observed between naptime duration and HDC (P for overall = 0.529; P for nonlinearity = 0.791) (Figure 3A). For participants aged 45–60 years, HDC probability increased linearly with longer naptime duration (P for overall = 0.001; P for nonlinearity = 0.591) (Figure 3B). In contrast, an inverse J-shaped correlation (peaking at 60 minutes) was identified in those aged >60 years (P for overall = 0.026; P for nonlinearity = 0.015) (Figure 3C).
Multivariable restricted cubic spline of nap duration. (A) <45 years; (B) 45–60 years; (C) >60 years. Solid lines indicate ORs, and shadow shape indicate 95% CIs. The gray column depicts the percentage of participants of different durations of napping.
Subgroup analysis
The subgroup analysis of nap duration and risk of HDC stratified by age, sex, and ethnicity are conducted to investigate whether there had differences among groups. The results are presented in Figure 4 (forest plot) and Supplementary Tables S1–S3.
Forest plot for stratified analyses of the associations between nap duration and the risk of HDC for age, sex, ethnicity, residence, annual household income, central obesity, smoke, drink, salt intake, physical activity, sleep duration, sleep disorder. Each group were adjusted for the other covariates except itself.
The subgroup analysis examining the association between nap duration and HDC, stratified by age, sex, and ethnicity, identified several notable findings. Among younger individuals, both short naps (0.5–1 h) and prolonged naps (>1 h) were associated with an increased risk of HDC compared to non-nappers. However, these associations were not statistically significant in the fully adjusted model (0.5–1 h: OR = 1.440, 95% CI: 0.616–3.287, P = 0.388; >1 h: OR = 1.722, 95% CI: 0.529–4.820, P = 0.324). For individuals aged 46–60, naps lasting more than 1 hour were significantly associated with a higher risk of HDC compared to non-nappers (model 3: OR = 2.106, 95% CI: 1.499–2.928, P < 0.001). Among older adults (>60 years), short naps (0–0.5 h) also showed an increased risk of 55.7% (OR = 1.557, 95% CI: 1.067–2.234), while no significant association was observed for naps lasting 0.5–1 h (OR = 1.336, 95% CI: 0.976–1.183). Naps shorter than 30 minutes were linked to an elevated risk of HDC in the fully adjusted model (OR = 1.557, 95% CI: 1.067–2.234, P = 0.019).
In the sex-stratified analysis, females with nap durations exceeding 1 hour exhibited a significant positive association with HDC (model 3: OR = 1.677, 95% CI: 1.165–2.369, P = 0.004). Similarly, in males, prolonged naps (>1 h) were consistently associated with a higher risk of HDC across all models (model 3: OR = 1.649, 95% CI: 1.174–2.296, P = 0.003). Ethnicity-stratified analysis revealed that among the Dong ethnic group, both short and long naps were linked to an elevated risk of HDC. For the Miao group, extended naps (>1 h) were associated with an increased risk of HDC compared to non-nappers, even after adjusting for potential confounders. In contrast, no significant associations were observed in the Bouyei group, regardless of nap duration.
Discussion
The present study explored the association between nap duration and HDC, revealing a significant relationship between nap duration and HDC risk. Our dose-response analysis indicated a clear duration-effect relationship: as nap duration increased, it was associated with an increased risk of HDC. This finding aligns with previous studies, suggesting a potential link between nap duration and the occurrence of hypertension and diabetes.
However, it is important to note that the underlying mechanisms of this association remain unclear. Prolonged napping may reduce energy expenditure and lead to obesity, which plays a significant role in the development of both diabetes and hypertension (24, 25). Additionally, long naps may disrupt individuals’ circadian rhythms of sleep and wakefulness (26, 27). The circadian rhythm, an internal biological clock, governs a wide array of physiological processes in the body. When long naps occur, they can misalign this internal clock. This misalignment directly affects the timing of hormone release, including insulin (28). With circadian rhythm disruption due to long naps, the normal pattern of insulin secretion is disrupted. For instance, insulin may be released at inappropriate times or in insufficient amounts (29). This disruption in insulin secretion leads to reduced insulin sensitivity. Insulin sensitivity refers to the body’s cells’ ability to respond effectively to insulin. When sensitivity decreases, cells do not take up glucose from the bloodstream as efficiently (30). As a result, blood glucose levels rise, and over time, this can lead to insulin resistance. Insulin resistance is a key precursor to both diabetes and hypertension (31). In relation to hypertension, insulin resistance can trigger a cascade of physiological changes. It can lead to increased sodium reabsorption in the kidneys, which in turn increases blood volume and ultimately raises blood pressure (32). All these factors ultimately contribute to HDC (33).
Although previous studies have highlighted the positive effects of daytime napping on learning, memory, work performance, and energy restoration (34, 35), most research has focused on the general population. This study, however, targeted ethnic minorities in southwest China, particularly the Dong, Miao, and Bouye groups. These groups have distinct cultural backgrounds, and socioeconomic conditions compared to the Han population (36, 37), which may uniquely influence the relationship between nap duration and HDC. For example, research has shown a positive correlation between higher socioeconomic status and hypertension prevalence among individuals with self-reported diabetes (38). In this study, among those with nap durations >1 hour, 47.55% were from the Dong ethnic group, with a higher proportion of individuals aged >60 years. In contrast, these proportions were only 30.10% and 22.35% among the Bouyei and Miao ethnic groups, respectively. This may explain why the relationship between nap duration and HDC differs across ethnic groups, as ethnicity could account for these discrepancies. Our study fills this research gap.
Moreover, our findings highlighted that individual who napped for more than 1 hour, particularly those aged 45–60 years from minority groups, had a significantly higher risk of HDC. While existing studies on napping have primarily focused on individuals aged 45 years and older, we categorized adults into three groups (<45, 45–60, and >60 years), thereby expanding the scope of research. Notably, we observed that the risk of HDC significantly increased only in the 45–60 age group when nap duration exceeded 1 hour compared to those who did not nap, which is consistent with previous findings (39).For individuals aged 45–60 years, prolonged nap durations likely reflect excessive fatigue or poor lifestyle habits, such as irregular sleep patterns (40). Extended periods of inactivity, such as naps lasting more than one hour, can adversely affect circulation and metabolism. Prolonged sedentary behavior is closely associated with the increased risk of various chronic conditions, particularly hypertension and diabetes (41, 42), and research has shown that prolonged sitting and physical inactivity can contribute to increased insulin resistance (41), leading to elevated blood glucose levels and negatively impacting cardiovascular health. This finding suggests that regulating nap duration may play a crucial role in the prevention of diabetes and its associated complications.
For individuals aged over 60, however, a nap duration of 0–30 minutes significantly increased the prevalence of HDC. The reduced physiological resilience of older adults means that short naps may be insufficient to provide adequate rest and recovery, particularly when compounded by pre-existing fatigue or physical weakness. A shorter nap duration may reflect an incomplete recovery process, exacerbating chronic fatigue and affecting the endocrine and metabolic systems, which in turn increases the risk of hypertension and diabetes (43, 44). These underlying mechanisms require further investigation to better understand the relationship between nap duration and the comorbidity of hypertension and diabetes.
These results highlight the age-dependent differences in the health impacts of nap duration, likely linked to factors such as physiological needs, lifestyle habits, and the body’s capacity for recovery. Therefore, tailored nap duration recommendations and increased physical activity may help reduce the risk of hypertension and diabetes comorbidity in different age groups. At the level of health policy, research findings indicate a need to strengthen health management of nap habits, particularly by implementing health education and intervention measures in high-risk populations. Governments and health organizations can incorporate reasonable napping into chronic disease prevention and control guidelines, advocate for moderate napping, and avoid the potential health risks of excessive daytime sleep. Additionally, combining individualized health management plans can optimize workplace and community health promotion strategies to reduce the incidence of HDC. In clinical practice, physicians should consider patients’ nap habits when assessing their risk of HDC, as part of a comprehensive evaluation of lifestyle factors. For individuals with a habit of long naps, healthcare professionals can offer appropriate lifestyle adjustment recommendations, such as limiting nap duration, improving nighttime sleep quality (45), and increasing physical activity (46), to reduce the risk of HDC. Furthermore, future research could consider incorporating nap behavior into comprehensive risk assessment models for HDC to enhance the precision of disease prediction and early intervention.
This study utilized a representative large sample database to investigate the relationship between nap duration and the co-occurrence of HDC in ethnic minority populations. To ensure the comprehensiveness and reliability of the results, subgroup analyses were conducted to validate the stability and generalizability of the findings across multiple dimensions. However, several limitations exist in this study. First, the assessment of nap duration was based on subjective self-reported data, which may introduce recall bias and, consequently, affect the accuracy of the data. Second, while the main focus of this study was on nap duration, factors such as nap frequency and timing, which are also important, were not explored. Most importantly, as a cross-sectional analysis, our study design inherently precludes causal inferences between napping and health outcomes. Although this investigation is embedded within an ongoing cohort study with planned longitudinal follow-ups, we strongly agree that future research should employ causal inference approaches—such as longitudinal designs tracking nap patterns over time, or Mendelian randomization studies leveraging genetic variants as instrumental variables—to formally test potential causal relationships (47).
Conclusion
This study suggests that nap duration is significantly associated with the co-occurrence of HDC in minority populations, with both short and long naps duration increasing the risk of HDC. These findings highlight the complex relationship between rest patterns and metabolic health, emphasizing the need for careful consideration of nap duration as part of health management strategies. Future research should explore the mechanisms behind these associations and whether regulating nap time could be an effective preventive measure, particularly in high-risk ethnic groups.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang L Wang K Liu LJ Zhang YY Shu HN Wang K. Associations of daytime napping with incident cardiovascular diseases and hypertension in Chinese adults: A nationwide cohort study. Biomed Environ Sci. (2022) 35:22–34. doi: 10.3967/bes 2022.004 35078559 · doi ↗ · pubmed ↗
- 2Wannamethee SG. Napping and Obesity in Adults – What do we Know? Curr Diabetes Rep. (2024) 24:237–43. doi: 10.1007/s 11892-024-01551-5 PMC 1140548839145893 · doi ↗ · pubmed ↗
- 3Li H Shi Z Chen X Wang J Ding J Geng S. Relationship between obesity indicators and hypertension–diabetes comorbidity in an elderly population: a retrospective cohort study. BMC Geriatrics. (2023) 23:789. doi: 10.1186/s 12877-023-04510-z 38036950 PMC 10691080 · doi ↗ · pubmed ↗
- 4Kitamura K Watanabe Y Nakamura K Takano C Hayashi N Sato H. Short daytime napping reduces the risk of cognitive decline in community-dwelling older adults: a 5-year longitudinal study. BMC Geriatr. (2021) 21:474. doi: 10.1186/s 12877-021-02418-0 34454431 PMC 8401113 · doi ↗ · pubmed ↗
- 5Zhang W Zhou B Jiang C Jin Y Zhu T Zhu F. Associations of daytime napping and nighttime sleep quality with depressive symptoms in older Chinese: the Guangzhou biobank cohort study. BMC Geriatr. (2023) 23:875. doi: 10.1186/s 12877-023-04579-6 38114908 PMC 10731710 · doi ↗ · pubmed ↗
- 6Leng Y Wainwright NWJ Cappuccio FP Surtees PG Hayat S Luben R. Daytime napping and the risk of all-cause and cause-specific mortality: A 13-year follow-up of a British population. Am J Epidemiol. (2014) 179:1115–24. doi: 10.1093/aje/kwu 036 PMC 399282124685532 · doi ↗ · pubmed ↗
- 7Han B Chen WZ Li YC Chen J Zeng ZQ. Sleep and hypertension. Sleep Breath. (2020) 24:351–6. doi: 10.1007/s 11325-019-01907-2 PMC 712799131402441 · doi ↗ · pubmed ↗
- 8Wang H Chen L Shen D Cao Y Zhang X Xie K. Association of daytime napping in relation to risk of diabetes: evidence from a prospective study in Zhejiang, China. Nutr Metab (Lond). (2021) 18:18. doi: 10.1186/s 12986-021-00545-4 33557863 PMC 7869458 · doi ↗ · pubmed ↗