Hydroa Vacciniforme: A Rare Pediatric Photodermatosis
Mouna Guechchati, Hanane Baybay, Meryem Zeryouhi, Layla Tahiri Elousrouti, FatimaZahra Mernissi

TL;DR
This paper describes a rare skin condition in a child caused by a virus and managed with sun protection.
Contribution
The study presents a new clinical case of hydroa vacciniforme with detailed diagnostic and management insights.
Findings
The patient showed chronic photodermatosis linked to Epstein-Barr virus infection.
Strict photoprotection led to sustained remission over two years.
Histopathology and immunohistochemistry confirmed characteristic lymphoid infiltrates and EBV involvement.
Abstract
Hydroa vacciniforme (HV) is a rare, chronic photodermatosis linked to Epstein-Barr virus (EBV) infection. We report a 12-year-old child with recurrent vesiculobullous facial lesions and photosensitivity for six years. Clinical examination revealed hemorrhagic crusts with atrophic scars. Dermoscopy showed whitish streaks and rosettes. Histopathology demonstrated epidermal spongiosis and a dense dermal lymphoid infiltrate. Immunohistochemistry confirmed CD3+, CD5+, CD7+, and CD8+ lymphocytes, with granzyme B and perforin expression, but no CD56. EBV serology was positive. Differential diagnoses, including cutaneous lupus, leishmaniasis, and porphyria, were excluded. The patient was managed with strict photoprotection, leading to sustained remission over two years. Early diagnosis and sun protection are essential for managing HV, as seen in our case.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
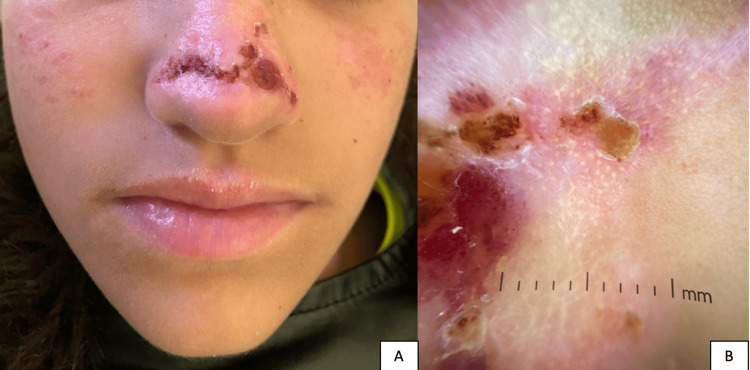 Figure 1
Figure 1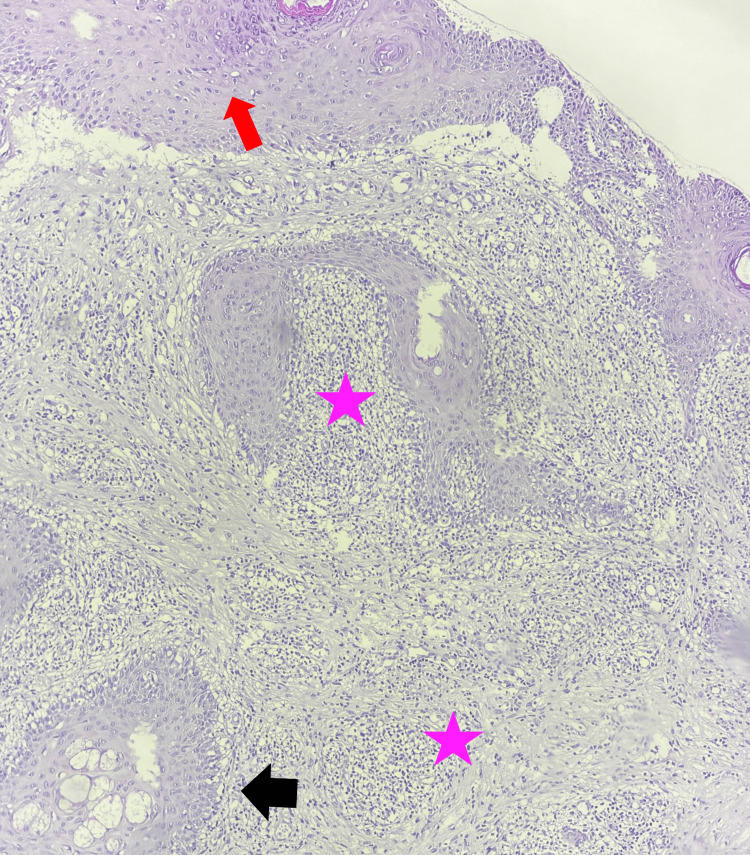 Figure 2
Figure 2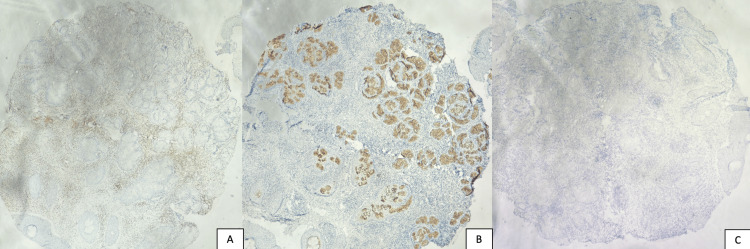 Figure 3
Figure 3| Feature | HV | DLE | Cutaneous leishmaniasis |
| Age/gender | Childhood, frequently resolving by adolescence | Typically young to middle-aged adults; more common in females | Any age; often in endemic areas |
| Trigger | Sun exposure (photosensitivity) | Sun exposure | Insect bites in endemic regions |
| Clinical lesions | Recurrent vesicles → crusts → varioliform scars on photo-exposed areas | Erythematous plaques with atrophic centers and adherent scales | Nodules/ulcers with raised borders in exposed areas |
| Common dermoscopic features | Whitish scar-like areas, rosettes, follicular plugs (our case) | Whitish scales, follicular plugs, arborizing blood vessels | Starburst pattern, yellow teardrop-shaped structures, central ulceration, hairpin, comma-shaped, vessels |
| Histopathology | Epidermal acanthosis, orthokeratotic hyperkeratosis, dermal lymphocytic infiltrate (perivascular and periadnexal) | Hyperkeratosis, follicular plugging, basal vacuolar degeneration, periadnexal/perivascular infiltrates | Mixed inflammatory infiltrate, amastigotes in macrophages (Leishman-Donovan bodies) |
| Immunohistochemistry | CD3+, CD5+, CD7+, CD8+, granzyme B+, perforin+, CD56- | Not routinely used; when done, interface T-cell infiltrate | Not routinely used; macrophage markers may be helpful |
| EBV findings | Positive EBV IgG; CISH testing for EBV DNA not performed | Not linked to EBV | Not linked to EBV |
| Systemic signs | None in our patient | May have systemic lupus signs in some cases | May have regional lymphadenopathy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · melanin and skin pigmentation · Dermatologic Treatments and Research
Introduction
Hydroa vacciniforme (HV) is a rare, idiopathic, and sporadic chronic photodermatosis characterized by recurrent vesicles and crusts on sun-exposed skin, typically leading to vacciniform or varioliform scarring [1]. It is a childhood photosensitivity disorder, initially considered benign due to its spontaneous resolution in adolescence [2]. Recent studies have linked HV to Epstein-Barr virus (EBV) infection. The role of EBV in HV pathogenesis remains unclear, but it is believed that EBV-induced immune dysregulation may play a role in disease development. Treatment options remain limited, with strict sun protection being the primary approach [3].
Although dermoscopy of hydroa vacciniforme is rarely discussed in the literature, it played a crucial role in this case by helping to exclude two major differential diagnoses, namely, lupus and leishmaniasis. The absence of dermoscopic signs characteristic of these diseases, such as the starburst pattern or corneal plugs, reinforced the clinical suspicion of hydroa vacciniforme. This case highlights the importance of a clinical, dermoscopic, and histological correlation to establish a rapid diagnosis, which can help minimize aesthetic damage by starting the appropriate treatment early.
Case presentation
We report the case of a 12-year-old girl from a non-consanguineous marriage who had been experiencing recurrent fluid-filled lesions on the central face for six years, with periods of remission and exacerbation, as well as a history of photosensitivity. The evolution was typical, with vesicular lesions appearing predominantly after sun exposure confined to the photo-exposed areas of the central face.
Clinical examination revealed hemorrhagic crusts associated with atrophic and varioliform scars on the cheeks and nasal tip (Figure 1A). There was no mucosal involvement (oral, conjunctival, corneal, or genital).
(A) Clinical presentation of hydroa vacciniforme with hemorrhagic crusts and atrophic varioliform scars on the cheeks and nasal tip. (B) Dermoscopy showing whitish scar-like areas scattered with rosettes and small, rounded follicular plugs.
The patient had no associated systemic symptoms such as joint swelling or pain, hair loss, lymphadenopathy, or hepatosplenomegaly. She also had no personal or family history of autoimmune disorders or similar dermatological conditions. There was no recent travel to a region endemic for leishmaniasis.
The dermoscopic image reveals whitish scar-like areas scattered with rosettes and small, rounded follicular plugs (Figure 1B). Unlike leishmaniasis, where facial follicular plugs often appear as peripheral teardrop-shaped structures, this pattern differs. It also contrasts with discoid lupus erythematosus, where follicular plugs are typically found at the periphery of scarring areas, indicating active disease. Additionally, the linear and dotted vascular pattern observed here differs from the short vessels seen in leishmaniasis and the arborizing vessels characteristic of discoid lupus. Also, lupus erythematosus and leishmaniasis were ruled out, as antinuclear antibodies and the leishmaniasis smear were negative. Laboratory studies, including complete blood count with differential, platelet count, liver and renal function tests, and red blood cell porphyrin levels, were all within normal limits.
Epstein-Barr virus (EBV) serology revealed positive IgG antibodies and negative IgM; however, PCR was not performed.
A skin biopsy of the lesions demonstrated an acanthotic epidermis with overlying orthokeratotic hyperkeratosis and focal spongiosis. The dermis contains a dense inflammatory infiltrate composed of lymphocytes, located periadnexally and perivascularly (Figure 2).
Histopathological findings of hydroa vacciniforme showing epidermal spongiosis (red arrow) with a dense dermal lymphoid infiltrate (pink star) located periadnexally and perivascularly (black arrow) (H&E stain, ×100 magnification).H&E: hematoxylin and eosin
In the immunohistochemical findings, the dermal lymphoid infiltrate, which showed positivity for CD3 (Figure 3A), CD5, CD7, and CD8, also included some cells that showed positivity for granzyme B and perforin (Figure 3B), indicating T-cell cytotoxic activity, with no CD56 expression (Figure 3C), helping to exclude NK/T-cell lymphoma. These findings supported a diagnosis of hydroa vacciniforme.
Immunohistochemical staining of the dermal lymphoid infiltrate: (A) CD3 expression highlighting T-cell predominance, (B) perforin positivity indicating cytotoxic activity, and (C) absence of CD56 expression, excluding NK/T-cell lymphoma.
Unfortunately, due to limited financial resources, chromogenic in situ hybridization (CISH) analysis for EBV DNA could not be performed.
The patient initially received fusidic acid both topically and orally, along with strict photoprotection combining both chemical and physical measures. Chemical photoprotection consisted of the application of a broad-spectrum sunscreen (SPF 50) specifically formulated for pediatric use and suited to her skin type, reapplied every two hours. Physical photoprotection included behavioral measures such as wearing wide-brimmed hats and protective clothing and avoiding sun exposure during peak UV hours to minimize ultraviolet radiation exposure. She showed excellent improvement with a two-year follow-up with close monitoring.
Discussion
Hydroa vacciniforme (HV) belongs to a rare and poorly described group of pediatric photodermatoses [4]. It mainly starts in childhood, frequently resolving by adolescence or young adulthood, with onset typically occurring between one and 11 years of age. It appears to have a slight male predominance. Its prevalence is 0.1-0.5 cases per 100,000 per year [5].
Hydroa vacciniforme (HV) is now recognized as a cutaneous manifestation of chronic active Epstein-Barr virus (EBV) infection, with lesions typically triggered by sun exposure [4]. The condition primarily affects sun-exposed areas such as the cheeks, nose, ears, and, less frequently, the forearms or hands. Clinically, the disease follows a chronic and recurrent course, with vesicles appearing shortly after sun exposure, subsequently evolving into crusts and leaving characteristic varioliform scars [6].
Although the disease is generally considered self-limiting and tends to resolve by adolescence, uncommon and more severe presentations have been reported. These include ocular involvement, ear and nasal deformities, or even finger contractures [2]. Importantly, the clinical presentation is the key factor in assessing prognosis. Features such as severe cutaneous involvement, loss of synchronization with sun exposure, lymphadenopathy, hepatosplenomegaly, or general deterioration should raise suspicion for a systemic form of chronic active EBV infection. This form carries a greater risk of progression to lymphoma and therefore warrants close, long-term monitoring [4].
The differential diagnosis of HV includes several blistering disorders triggered by light exposure, such as erythropoietic protoporphyria (EPP), bullous lupus erythematosus, solar urticaria, hydroa aestivale, and porphyria cutanea tarda (PCT). In our patient, a detailed clinical dermoscopical assessment, histopathological examination, and laboratory investigations allowed us to confirm the diagnosis of HV while ruling out other differential diagnoses [7].
A careful dermoscopic analysis can highlight key differences, aiding in the exclusion of major differential diagnoses. In this case, dermoscopy was instrumental in distinguishing HV from other conditions such as leishmaniasis and lupus erythematosus. The absence of characteristic dermoscopic signs, such as the peripheral teardrop-shaped follicular plugs seen in leishmaniasis or the active disease indicators such as peripheral follicular plugs in lupus [8], helped confirm the diagnosis of HV. Furthermore, the linear and dotted vascular pattern observed in our case contrasted sharply with the typical vascular patterns seen in both leishmaniasis and lupus, which further supported the diagnosis of hydroa vacciniforme. This underscores the importance of dermoscopy as a non-invasive tool in providing valuable diagnostic insights, particularly when dealing with difficult-to-diagnose cases and differentiating between similar-appearing disorders [9]. Table 1 highlights the distinguishing features between hydroa vacciniforme and its main differential diagnoses.
Therefore, clinicians should suspect HV in children presenting with recurrent vesicular eruptions on sun-exposed areas that evolve into varioliform scars, particularly when there is a history of photosensitivity, especially in cases where there is a lack of characteristic dermoscopic findings of other pathologies.
In managing HV, various therapeutic options have been explored, although evidence remains limited due to the rarity of the condition and the absence of randomized trials [5]. Preventive measures remain the cornerstone of management. These include rigorous photoprotection through the use of broad-spectrum sunscreens (SPF 30 or preferably 50) with high UVA protection, applied generously 15-30 minutes before sun exposure and reapplied every two hours or after swimming or towel-drying [10]. Sunscreens remain the most effective therapeutic agents and are essential even when other treatments are used [6]. Physical photoprotection, such as wearing thick or specialized sun-protective clothing, wide-brimmed hats, and UV-protective sunglasses, along with avoiding sun exposure during peak hours (11 a.m. to 3 p.m.), is equally crucial [10]. In moderate to severe disease, narrowband UVB or PUVA phototherapy may offer clinical improvement if carefully administered to avoid disease flares [5]. In more refractory cases, systemic therapies such as antimalarial agents, cyclosporine, or azathioprine have been used, although their efficacy is variable and their use in children must be weighed against the risk of adverse effects [11]. β-carotene and dietary fish oils rich in omega-3 fatty acids have been reported with occasional benefit in isolated cases [5]. Ultimately, treatment should be tailored based on severity, the patient's quality of life, and risk-benefit considerations.
Conclusions
In summary, we report a 12-year-old girl with the characteristic clinical and histopathological findings of HV, emphasizing the importance of clinically suspecting the diagnosis in typical presentations on photo-exposed areas and confirming it through histopathological examination. The use of dermoscopy, as demonstrated in this case, can help exclude other conditions such as lupus (absence of a starburst pattern) and leishmaniasis (absence of corneal plugs), further supporting a diagnosis of hydroa vacciniforme.
To our knowledge, dermoscopic features of HV have not been previously described in the literature, which underscores the need for further attention to their detailed characterization. In our patient, strict photoprotection has led to sustained remission, demonstrating the importance of early intervention in managing the disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An unusual case of hydroa vacciniforme with ocular involvement Med Arch OkumuşS Coskun E Cömez G Erbağci Z Cömez A Erbağci I 2112126620122282262810.5455/medarh.2012.66.211-212 · doi ↗ · pubmed ↗
- 2Hydroa vacciniforme Rice AS Bermudez R Treasure Island, FL Stat Pearls Publishing 314248962025 https://www.ncbi.nlm.nih.gov/books/NBK 545312/31424896 · pubmed ↗
- 3Antiviral treatment of a boy with EBV-associated hydroa vacciniforme BMJ Case Rep Pahlow Mose A Fisker N Clemmensen O Bygum A 2014201410.1136/bcr-2014-206488 PMC 424434825422336 · doi ↗ · pubmed ↗
- 4Cutaneous lymphoproliferation of the hydroa vacciniforme type: three cases (Article in French)Ann Dermatol Venereol Touzlian J Macagno N Hubiche T Richard MA Mallet S 01462019
- 5Hydroa vacciniforme Dermatology Hönigsmann H 108Elsevier 2018 https://doi.org/10.1016/B 978-0-7020-6912-3.00108-7
- 6Hydroa vacciniforme: a review of ten cases Br J Dermatol Sonnex TS Hawk JL 1011081181988334216810.1111/j.1365-2133.1988.tb 01757.x · doi ↗ · pubmed ↗
- 7A case of hydroa vacciniforme Ann Dermatol Park HY Park JH Lee KT Lee DY Lee JH Lee ES Yang JM 3123152220102071126810.5021/ad.2010.22.3.312PMC 2917685 · doi ↗ · pubmed ↗
- 8Dermoscopic criteria of discoid lupus erythematosus: an observational cross-sectional study of 28 patients Indian J Dermatol Venereol Leprol Fathy H Ghanim BM Refat S Awad A 3603668820223513806310.25259/IJDVL_207_19 · doi ↗ · pubmed ↗