Electrolyte abnormalities and clinical outcomes in children aged one month to 13 years hospitalized with acute gastroenteritis in two large referral hospitals in Botswana
Anita A. Kinasha, Jeffrey M. Pernica, Francis M. Banda, David M. Goldfarb, Henry D. Welch, Andrew P. Steenhoff, Sarah A. MacLean

TL;DR
This study examines how electrolyte imbalances in children with acute gastroenteritis in Botswana affect hospital stays and mortality.
Contribution
The study identifies specific electrolyte abnormalities and risk factors for mortality in children with acute gastroenteritis in Botswana.
Findings
37% of hospitalized children with acute gastroenteritis had electrolyte abnormalities.
Malnutrition, hypokalaemia, and hypernatraemia were strong predictors of mortality.
Children with hypokalaemia or hyponatraemia had longer hospital stays.
Abstract
Acute gastroenteritis (AGE) is a common childhood disease, with a median of 2.5 diarrhoea episodes per child per year in both low- and middle-income countries. Morbidity and mortality from AGE result from a number of causes, including electrolyte abnormalities. This study characterized children hospitalized for AGE in Botswana with and without electrolyte abnormalities. This was a prospective observational study of children under the age of 13 years who were admitted with AGE in Princess Marina Hospital (PMH) and Nyangabgwe Referral Hospital (NRH) between May 2011 and April 2013. All children with serum electrolyte values obtained within 48 hours of admission were included. Patient characteristics and prevalence of electrolyte abnormalities were described. Risk factors for mortality were explored using univariate and multivariate logistic regression analyses. Among 544 patients, 37% had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
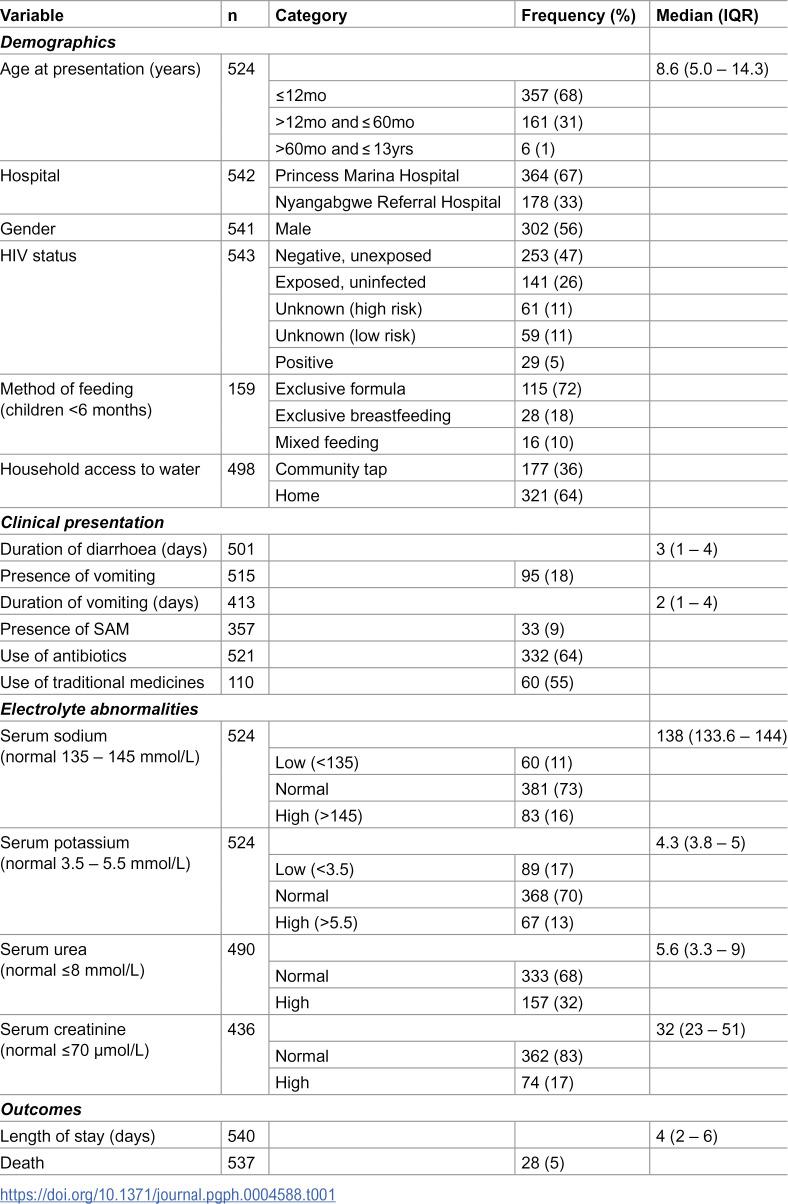 Figure 1
Figure 1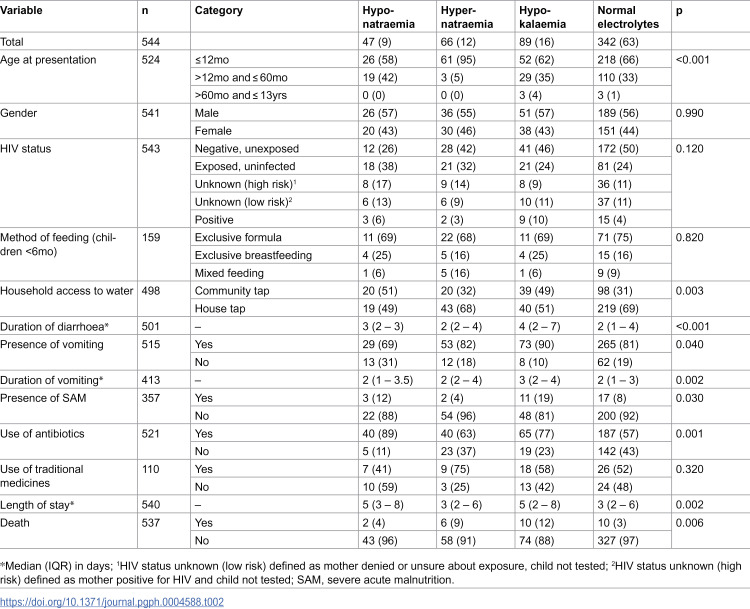 Figure 2
Figure 2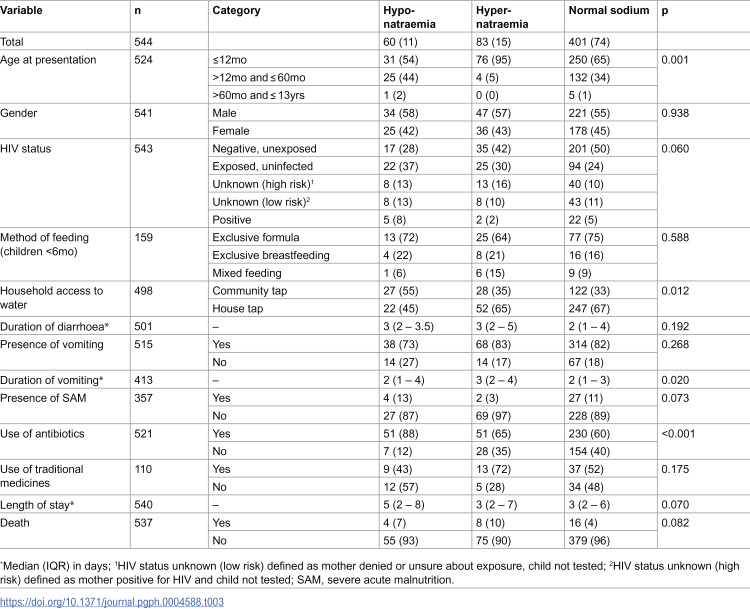 Figure 3
Figure 3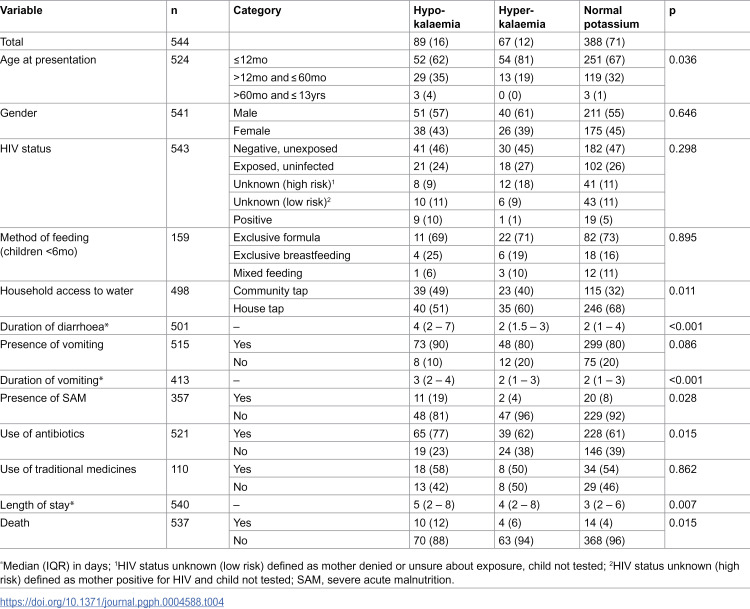 Figure 4
Figure 4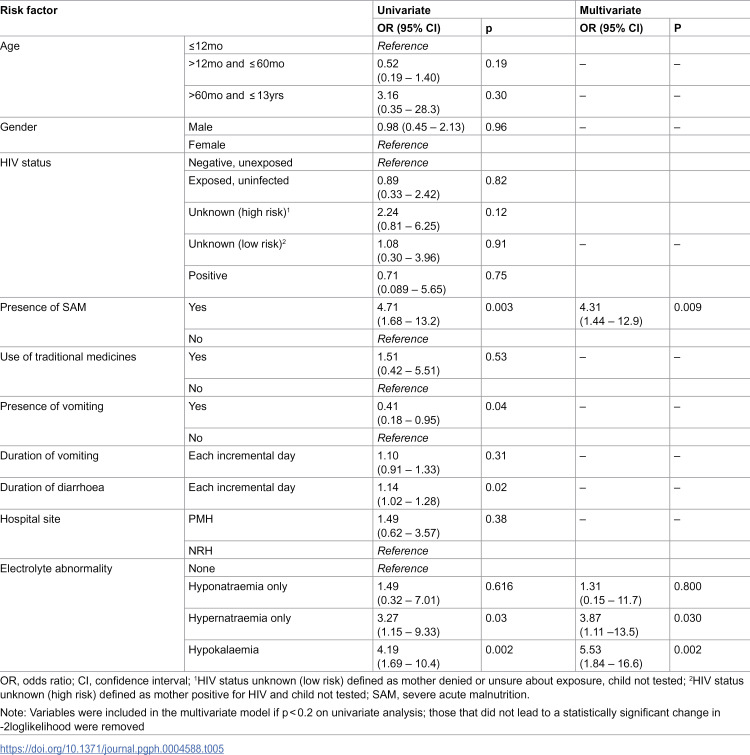 Figure 5
Figure 5- —http://dx.doi.org/10.13039/501100004828Grand Challenges Canada
- —Penn Center for AIDS research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral gastroenteritis research and epidemiology · Child Nutrition and Water Access · Child Nutrition and Feeding Issues
Introduction
Globally, acute gastroenteritis (AGE) is the second leading cause of death in young children after the neonatal period [1]. Gastroenteritis is defined as inflammation of the mucosal lining of the gastrointestinal tract which leads to vomiting and/or diarrhoea [2,3]. Diarrhoea is defined by the World Health Organization (WHO) as passage of three or more loose or watery stools per day or more frequent passage of stool than normal [4,5]. AGE is differentiated from persistent gastroenteritis by it lasting less than 14 days [4,5]. Severe AGE is that which causes hospital admission [4]. In 2016, about 90% of diarrhoeal deaths among children younger than 5 years occurred in South Asia and Sub-Saharan Africa [3]. Diarrhoeal illnesses are also known to cause long-term morbidity, leading to conditions including undernutrition and cognitive impairment [6]. Children under the age of five years are particularly at risk, with studies reporting a decreasing prevalence of diarrhoeal disease in children with increasing age [7–9].
In general, low and middle-income countries (LMIC) have higher rates of hospital admissions, morbidity and mortality from gastroenteritis compared to high-income countries (HIC) [7]. In Africa, among children under 5 years of age, there were between 2.04 and 2.85 episodes of diarrhoea per child per year in 2016 [10]. Factors contributing to higher rates of AGE in LMIC include undernutrition, increased vulnerability to infections, poor education, lower socio-economic status, the growing trend of breastmilk substitutes, poor health services, poor sanitation and unavailability of clean water [11,12]. In 2018 in Botswana, diarrhoea was the second leading cause of under-five mortality excluding neonates, accounting for 12% of deaths [13]. Between 2011 and 2013 at Princess Marina Hospital (PMH) and Nyangabgwe Referral Hospital (NRH), Botswana’s two largest hospitals, children with severe AGE had an in-hospital mortality rate of 4% [14]. These data confirm that AGE is a major cause of under-five morbidity and mortality in LMIC, including Botswana.
It is widely known that electrolyte abnormalities frequently occur in children with severe AGE with estimates varying between 30% to 60% [15–20]. Early mortality in patients with AGE usually occurs due to dehydration, which results from loss of fluid and electrolytes in diarrhoeal stools [21,22]. A study of AGE in Iran found 41.6% of participants had sodium abnormalities and 13% had hypokalaemia. In that study, the concentration of oral rehydration solution (ORS) given prior to admission played an important role in the type and severity of electrolyte abnormalities [20]. Both morbidity and mortality may be exacerbated by co-existent electrolyte abnormalities [19]. In Botswana, a number of studies have described the epidemiology and aetiology of AGE in children [14,23,24], but there have been no Botswana-based studies which explored the profile of serum electrolytes in children with AGE, the severity of electrolyte abnormalities seen in association with AGE, risk factors associated with severe electrolyte abnormalities, and clinical outcomes. Moreover, there is a paucity of data from the African continent on this topic. The primary objective of this study was to determine the rates of electrolyte abnormalities in a cohort of children hospitalized with AGE at two large referral hospitals. The secondary objective was to identify covariates associated with electrolyte abnormalities and clinical outcomes among children with and without electrolyte abnormalities.
Methods
Study setting and design
This was a prospective observational study conducted using an existing set of deidentified data collected between May 2011 and April 2013. The larger study enrolled 671 children admitted for severe acute gastroenteritis and analyzed stool samples to detect common enteropathogens. All participants were followed through hospital discharge and data on clinical outcomes was recorded. Inclusion criteria included being less than 13 years of age and having acute diarrhoea (defined as at least 3 loose stools or a single loose stool with at least 2 episodes of emesis in any 24-hour period prior to enrolment) for less than 14 days. Participants were admitted to the two largest public referral hospitals in Botswana, Princess Marina Hospital (PMH) and Nyangabgwe Referral Hospital (NRH) [14]. PMH has an average of about 130 admissions per month with 10% of these being children with AGE. Both hospitals follow protocols for community-acquired AGE based on WHO guidelines. These protocols include fluid resuscitation, zinc supplementation, and targeted blood investigations including full blood counts, electrolytes, and renal function tests within 48 hours of admission. At both hospitals, the decision to test electrolytes was ultimately at the discretion of the admitting clinician.
Inclusion criteria.
Children were included if they were less than 13 years old, admitted with less than 14 days of diarrhoea (defined as at least 3 loose stools or a single loose stool with at least 2 episodes of emesis in any 24-hour period prior to enrolment), and had electrolytes measured upon admission.
Exclusion criteria.
Patients were excluded if they did not have electrolyte values recorded on admission. They were also excluded if they had nosocomial infections, defined as developing diarrhoea more than 48 hours after admission or being readmitted with diarrhoea within 7 days of discharge from a previous hospital admission.
Data analysis
Covariates used for the analysis included age, gender, method of feeding, HIV status, presence of vomiting, duration of vomiting, severity of vomiting, duration of diarrhoea, severity of diarrhoea, use of antibiotics at admission, presence and type of malnutrition, traditional medicine use, and serum sodium, potassium, urea and creatinine. For the multivariate analysis, electrolyte abnormalities were classified in order to create three distinct groups: hyponatraemia, defined as serum sodium <135 mmol/L, with normal potassium; hypernatraemia, defined as serum sodium >145 mmol/L, with normal potassium; and hypokalaemia, defined as serum potassium <3.5 mmol/L regardless of sodium level. Hyperkalaemia was not included in the multivariate analysis because in clinical practice it is not a common abnormality associated with AGE, but rather a result of the test being performed on a haemolysed blood sample, hence providing a falsely elevated potassium level. To determine whether there were differences in demographic characteristics, clinical history, and outcomes between children with different electrolyte abnormalities, either chi-square tests or Fisher’s exact test were used for categorical independent variables; t-tests or Kruskal-Wallis equality-of-populations testing were used to determine whether continuous variables (i.e., duration of diarrhoea, length of stay) were associated with categorical variables of interest.
The final analysis sought to determine which covariates were associated with death in the cohort. Certain covariates of interest (age, sex, HIV status, vomiting, diarrhoea, malnutrition, and electrolyte abnormalities) were run as univariate logistic regression and those predictive factors that were found to be associated with a p-value <0.2 were then entered into a forward stepwise multivariate logistic regression analysis. Only those covariates that led to a statistically significant (p < 0.05) improvement in the -2loglikelihood of the model were retained in the final multivariate model. The database was accessed on 19/03/2019 for this study and he data were analyzed using STATA version 11.0 (College Station, TX).
Ethical considerations
Ethical approval was obtained from the ethics committees of the Botswana Ministry of Health, PMH, and the University of Botswana; written informed consent was obtained from the parent/guardian of each participant below 18 years of age.
Results
Among the 671 children enrolled in the database, 544 (81%) had electrolyte values recorded on admission and were included in the study. Their demographic data, clinical characteristics and electrolyte abnormalities are summarized in Table 1. The median age was 8.6 months (IQR [interquartile range] 5–14 months) and the majority of patients were less than 12 months of age. Two thirds of patients were admitted to PMH and 56% were males. Almost half of patients (47%) were HIV negative/unexposed, one quarter (26%) were exposed but uninfected, and 5% were HIV positive. Among those <6 months, most patients (72%) were exclusively formula fed. In terms of clinical presentation, 18% of children had vomiting in addition to diarrhoea and 9% had severe acute malnutrition (SAM) as per WHO standards.
Table 1: Demographic characteristics, clinical presentation, and electrolyte abnormalities among children with severe acute gastroenteritis (N = 544).
As shown in Table 2, 37% of patients had electrolyte abnormalities. Of these, 9% had hyponatraemia with a normal potassium level, 12% had hypernatraemia with a normal potassium level, and 16% were hypokalaemic. There were statistically significant differences in the age distributions of the participants in each of the electrolyte groups (p value <0.001). In particular, almost all (95%) of children with hypernatraemia were ≤12mo. There were no significant differences in gender, HIV status, or method of feeding of the patients with electrolyte abnormalities compared to those without. However, household water source was associated with electrolyte abnormalities (p = 0.003) with higher rates of hyponatraemia and hypokalaemia amongst those using a community tap.
Table 2: Characteristics and clinical outcomes of children with severe acute gastroenteritis with and without electrolyte abnormalities.
There were statistically significant differences in the duration of diarrhoea (p < 0.001) and vomiting (p = 0.002) observed between the groups. In both cases, the hypokalaemia group had the longest duration of symptoms. There were statistically significant differences in the proportion of children with severe acute malnutrition between the groups (p = 0.03); the hypokalaemia group had the largest proportion of malnourished children. There were also statistically significant differences in length of stay between groups (p = 0.002), with a median length of stay of 5 days in both the hypokalaemia (IQR 2–8) and hyponatraemia (IQR 3–8) groups. Finally, there were statistically significant differences in case-fatality rates between groups (p = 0.006), with the most mortality (12%) observed in the hypokalaemia group.
Table 3 compares patients with sodium abnormalities to those with normal sodium, showing statistically significant differences in the age at presentation between the groups (p = 0.001). Of note, almost all patients with hypernatraemia (95%) were under 12 months of age.
Table 3: Characteristics and clinical outcomes of children with severe acute gastroenteritis with and without sodium abnormalities.
Table 4 compares patients with potassium abnormalities to those with normal potassium. There were statistically significantly differences in the duration of diarrhoea between the groups (p < 0.001); for example, those with hypokalaemia had a median of 4 days of diarrhoea (IQR 2–7), whereas those with normal potassium only had a median of 2 days of diarrhoea (IQR 1–4). There were also statistically significantly differences in the length of hospital stay between the different groups (p = 0.007). Patients with hypokalaemia had a median duration of stay of 5 days (IQR 2–8), whereas those with normal potassium had a median duration of stay of only 3 days (IQR 2–6).
Table 4: Characteristics and clinical outcomes of children with severe acute gastroenteritis with and without potassium abnormalities.
In the multivariable logistic regression analysis (Table 5), malnutrition was associated with 4-fold higher odds of mortality (p = 0.009). Also, a statistically significant association between electrolyte abnormality and mortality was noted. Children with hypokalaemia had 5 times higher odds of mortality than those without electrolyte abnormalities (p = 0.002), whereas those with hypernatremia had almost 4 times higher odds of mortality than those without electrolyte abnormalities (p = 0.03).
Table 5: Univariate and multivariate logistic regression analysis of the factors associated with mortality in children with severe acute gastroenteritis.
Hospital site was included in the analysis to account for one site (PMH) having a particular protocol for managing patients with AGE, which was not utilized at the other site (NRH). There was no statistically significant difference between the two sites (p = 0.38).
Discussion
To the best of our knowledge, this is the first study on the prevalence of electrolyte abnormalities in children admitted with AGE in Botswana and one of the first in Sub-Saharan Africa [16]. The study describes associations of these electrolyte abnormalities to patient characteristics and clinical outcomes. The overall prevalence of electrolyte abnormalities was 37%. In the multivariate model, three factors were associated with higher odds of death: hypokalaemia (OR 5.5), hypernatraemia (OR 3.9) and malnutrition (OR 4.3).
Prevalence of electrolyte abnormalities
In this study, 37% of subjects had electrolyte abnormalities. Hypokalaemia was the most common (16%) followed by hypernatraemia (12%) and hyponatraemia (9%). Hypokalaemia may be explained by the potassium loss that commonly occurs in children with diarrhoea and a subsequent physiological response to excessive fluid loss [25]. Hyponatraemia is commonly caused by fluid losses, which can lead to the release of antidiuretic hormone and subsequent retention of excessive water [25,26] whereas hypernatraemia may be caused by excessive fluid loss and ineffective rehydration [27]. The prevalence of hypokalaemia in malnourished children with AGE has been found in other studies in Pakistan and the Netherlands to be about 60%, with the rationale that these children tend to have an underlying subclinical hypokalaemia thought to be caused by a “whole body” chronic potassium depletion [28–30]. In contrast, studies of electrolyte abnormalities in children with AGE in Nigeria and India described hyponatremia as the most common abnormality in over 60% of children [16,19], whereas another study in Germany showed hypernatremia (77%) to be the commonest among patients with AGE, specifically children with rotavirus diarrhoea [31]. The differences with other studies may be attributed to different rates of ORS use prior to presentation to the hospital [32] and possibly use of incorrectly prepared infant formula [19]. Comparing AGE studies across continents has significant limitations, though, as there are many differences in factors such as local microbiology and rates of environmental enteropathy.
Covariates associated with electrolyte abnormalities
In this study, hypernatraemia was more prevalent in younger patients. These findings are similar to those of a study on children admitted for severe diarrhoea in Bangladesh, where the median age for patients with hypernatraemia was seven months [32]. Hypernatraemia has been associated with dehydration in children younger than one year of age and is believed to be caused by ineffective breastfeeding or rehydration by the caregiver [27]. Younger children are unable to respond to thirst by drinking fluids on their own and are therefore at a greater risk of developing hypernatraemic dehydration [25].
Hypokalaemia is another important complication of AGE. Generally, a longer duration of diarrhoea is associated with hypokalaemia as was seen in this study, likely due to greater excretion of potassium in stool than sodium [25]. In this study, hypokalaemia was the most common abnormality amongst the 9% of subjects with SAM. Several studies have shown an association between malnutrition and electrolyte imbalances in children with AGE [30,33]. This is likely due to children with malnutrition being chronically potassium depleted even before they develop AGE [29,30,33]. Similarly, two studies in Pakistan showed about 60% of patients with malnutrition had hypokalaemia [28,29]. There were higher rates of hypokalaemia amongst those using a community tap. Prior studies have found that using a community tap is a risk factor for developing diarrhoea, but further research on the association between hypokalaemia and use of a community tap is warranted [3,12,34,35].
Clinical outcomes
Electrolyte abnormalities are known to increase morbidity and mortality in patients with AGE [36]. In this study, both electrolyte abnormalities and malnutrition were associated with higher odds of mortality. Similarly, a study of children hospitalized for diarrhoea in Turkey showed an overall death rate of 6.75%, with hypokalaemia as a significant risk factor for mortality in univariate analysis [37]. A study in Bangladesh described a higher case fatality rate of 12% in hypernatraemia compared to 5% in hyponatraemia [32]. Furthermore, a study in Kenya found greater odds of death in patients with malnutrition (OR 3.5) and hypokalaemia (OR 2.5); that study also found 4.6-fold odds of death in patients with hyponatraemia [33]. Finally, in Mozambique, malnutrition was found to be an independent risk factor for death in patients with AGE with a hazard ratio of 4.1 in the multivariate analysis [21]. In combination, these studies reinforce the importance of having access to clinical electrolyte testing for any hospital that is managing patients with severe AGE. This is also supported by WHO which, in its Essential Diagnostics List, recommends electrolyte testing via automated chemistry analyser to be made available at the district hospital level and higher [38]. Nevertheless, recent surveys conducted in LMIC hospitals reveal that chemistry analysers are often not available [39]. The current WHO AGE management guidelines do not advocate for the routine measurement of serum electrolytes as these values are often misinterpreted, however in light of the study findings it may be necessary to revisit these guidelines [40,41]. In clinical practice, oral rehydration therapy (ORT) is generally recommended as the first-line treatment for paediatric gastroenteritis and dehydration, except in cases of severe dehydration where the use of intravenous fluids may be warranted. With the ability to measure serum electrolytes, clinicians would be better able to identify those patients with severe dehydration and provide the most appropriate options for their care. This is particularly important in LMIC where intravenous fluids are particularly limited [2,39].
Study limitations
This study has some limitations. Although a prospective observational study with real-time data collection, there are unmeasured confounders including the possible impact of ORT, method of formula preparation, different aetiologies of diarrhoea as well as physical exam findings at presentation. Measurements of whether patients received ORT preadmission were not included, which could have affected their serum electrolyte profile at presentation. Similarly, 72% of patients under six months were exclusively formula fed, but the method of preparation was not recorded, which may have affected electrolyte values on admission.
Conclusion
This study of electrolyte abnormalities in children admitted with AGE in Botswana found that hypokalaemia, hypernatraemia, and malnutrition were each associated with increased odds of mortality. It is imperative that clinicians take additional care and precautions when admitting children with the above risk factors. Given the global impact of paediatric AGE, further studies like this from other countries are needed to explore optimal management, minimize mortality, and obtain a clearer assessment of the impact of confounders that were unmeasured in this study.
Supporting information
S1 AppendixDefinitions of HIV status and severe acute malnutrition.(DOCX)
S2 AppendixAGE database.(XLS)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pavlinac PB, Tickell KD, Walson JL. Management of diarrhea in HIV-affected infants and children. Expert Rev Anti Infect Ther. 2015;13(1):5–8. doi: 10.1586/14787210.2015.981157 25384353 PMC 4609505 · doi ↗ · pubmed ↗
- 2Chow CM, Leung AK, Hon KL. Acute gastroenteritis: from guidelines to real life. Clin Exp Gastroenterol. 2010;3:97–112. doi: 10.2147/ceg.s 6554 21694853 PMC 3108653 · doi ↗ · pubmed ↗
- 3Abdoli A, Maspi N. Commentary: estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: a systematic analysis for the Global Burden of Disease Study 2015. Front Med (Lausanne). 2018;5:11. doi: 10.3389/fmed.2018.00011 29435450 PMC 5796900 · doi ↗ · pubmed ↗
- 4Winckel MVAN, Chevalier P, Loof GDE, Lierde SVAN, Petrovic M. Acute gastro-enteritis. huisarts Nu. 2011;40(4):S 118–29.
- 5Diarrhoeal disease [Internet]. [cited 2024 Feb 28]. Available from: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease
- 6Troeger C, Colombara DV, Rao PC, Khalil IA, Brown A, Brewer TG, et al. Global disability-adjusted life-year estimates of long-term health burden and undernutrition attributable to diarrhoeal diseases in children younger than 5 years. Lancet Glob Health. 2018;6(3):e 255–69. doi: 10.1016/S 2214-109X(18)30045-7 29433665 PMC 5861379 · doi ↗ · pubmed ↗
- 7Troeger C, Forouzanfar M, Rao PC, Khalil I, Brown A, Reiner RC, et al. Estimates of global, regional, and national morbidity, mortality, and aetiologies of diarrhoeal diseases: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17(9):909–48. doi: 10.1016/S 1473-3099(17)30276-1 28579426 PMC 5589208 · doi ↗ · pubmed ↗
- 8View of prevalence of diarrhoea and its association with wasting, age, and gender in children below the age of five years | International Journal of Medical Research and Review [Internet]. [cited 2020 Oct 1]. Available from: https://ijmrr.medresearch.in/index.php/ijmrr/article/view/108/210