Methodological Quality of Systematic Reviews on Platelet-Rich Plasma Therapy for Osteoarthritis: A Meta-Research Study
Maria Eduarda Oliveira Onuki, Kamilla Mayr Martins Sá, Marcela Lourenço Alves, Maria Eduarda de Souza, Elaine Marcílio Santos, Ana Luiza Cabrera Martimbianco

TL;DR
This study evaluates the quality of systematic reviews on platelet-rich plasma therapy for osteoarthritis and finds most have significant methodological flaws.
Contribution
The study reveals widespread methodological shortcomings in PRP osteoarthritis reviews, emphasizing the need for improved research practices.
Findings
84% of reviews were rated as critically low quality, with major issues in search strategies and study exclusion reasons.
Only 19.3% of reviews used the GRADE approach to assess evidence certainty.
Most reviews failed to report protocol registration or risk of bias in results.
Abstract
Objective To assess the methodological quality of systematic reviews on the benefits and disadvantages of platelet-rich plasma (PRP) to treat osteoarthritis. Methods We conducted a comprehensive literature search, and the methodological quality of the included reviews was assessed using the tool A Measurement Tool to Assess Systematic Reviews, Version 2 (AMSTAR-2). In addition, the assessment of the certainty of evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was investigated. A total of 31 systematic reviews met the inclusion criteria. Results Almost 84% of the articles received an overall rating of critically-low quality, and 16.1%, of low quality. The methodological criteria most frequently reported in an inadequate manner were related to search strategies, with 77.3% of “no” or “partially yes” responses, and the reasons to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
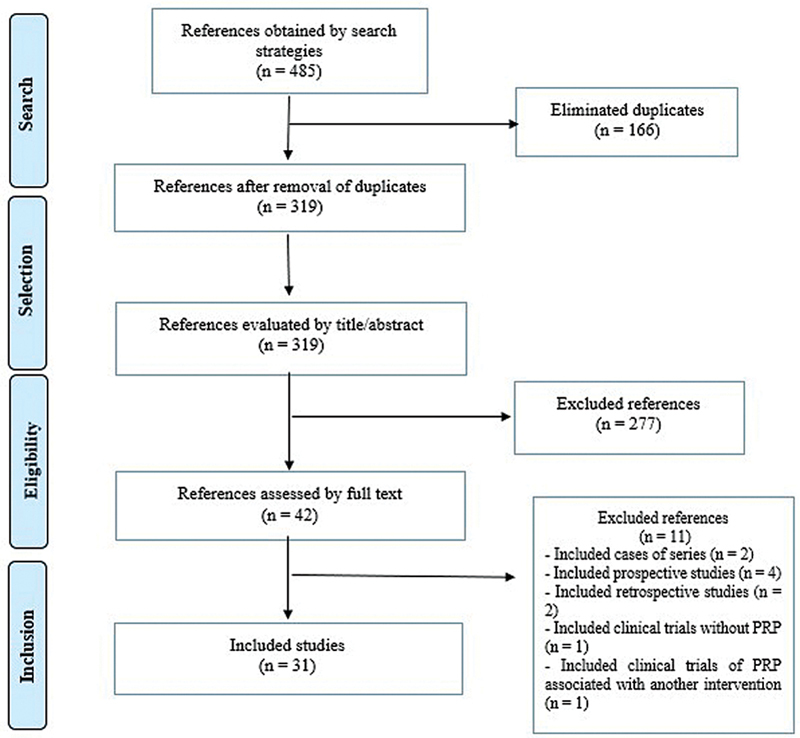 Fig. 1
Fig. 1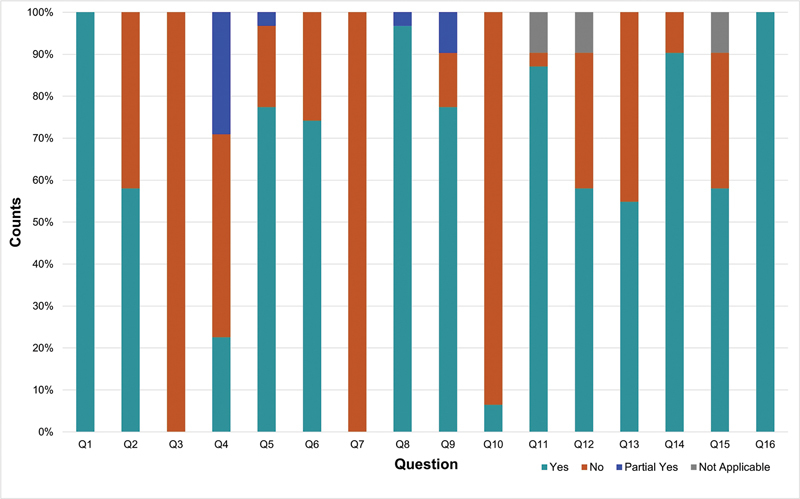 Fig. 2
Fig. 2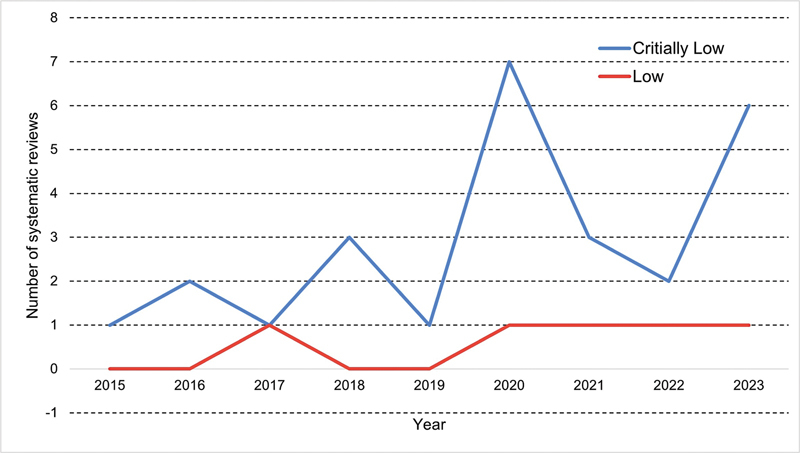 Fig. 3
Fig. 3| Database | Search strategies | Results |
|---|---|---|
| Medical Literature Analysis and Retrieval System Online (MEDLINE, via Pubmed) | #1 “Osteoarthritis” [Mesh] OR Osteoarthritides OR Osteoarthrosis OR Osteoarthroses OR (Arthritis, Degenerative) OR (Arthritides, Degenerative) OR (Degenerative Arthritides) OR (Degenerative Arthritis) OR Arthrosis OR Arthroses | 221 |
| The Cochrane Library (Cochrane Database of Systematic Reviews, CDSR) | #1 MeSH descriptor: [Osteoarthritis] explode all trees | 7 |
| Excerpta Medica Database (Embase, via Elsevier) | #1 'osteoarthritis'/exp OR Osteoarthritides OR Osteoarthrosis OR Osteoarthroses OR 'Arthritis, Degenerative' OR 'Arthritides, Degenerative' OR 'Degenerative Arthritides' OR 'Degenerative Arthritis' OR Arthrosis OR Arthroses | 135 |
| Epistemonikos | ((title:(Osteoarthritis OR Osteoarthritides OR Osteoarthrosis OR Osteoarthroses OR (Arthritis, Degenerative) OR (Arthritides, Degenerative) OR (Degenerative Arthritides) OR (Degenerative Arthritis) OR Arthrosis OR Arthroses) OR abstract:(Osteoarthritis OR Osteoarthritides OR Osteoarthrosis OR Osteoarthroses OR (Arthritis, Degenerative) OR (Arthritides, Degenerative) OR (Degenerative Arthritides) OR (Degenerative Arthritis) OR Arthrosis OR Arthroses))) OR abstract:((title:(Osteoarthritis OR Osteoarthritides OR Osteoarthrosis OR Osteoarthroses OR (Arthritis, Degenerative) OR (Arthritides, Degenerative) OR (Degenerative Arthritides) OR (Degenerative Arthritis) OR Arthrosis OR Arthroses) OR abstract:(Osteoarthritis OR Osteoarthritides OR Osteoarthrosis OR Osteoarthroses OR (Arthritis, Degenerative) OR (Arthritides, Degenerative) OR (Degenerative Arthritides) OR (Degenerative Arthritis) OR Arthrosis OR Arthroses)))) AND (title:((Plasma, Platelet-Rich) OR (Platelet Rich Plasma) OR PRP) OR abstract:((Plasma, Platelet-Rich) OR (Platelet Rich Plasma) OR PRP)) | 122 |
| Systematic Review | Justification |
|---|---|
|
| Associated PRP with another intervention (BMAC) |
|
| Included retrospective studies |
|
| Associated PRP with another intervention |
|
| Included case series |
|
| Included cohort studies |
|
| Included cohort studies |
|
| Included cohort studies |
|
| Included cohort studies |
|
| Trials without PRP |
|
| Included prospectives and retrospectives studies |
|
| Included case series |
| First author, year | Included RCTs (n) | Interventions versus (vs.) comparators | Systematic review protocol | Methodological quality assessment | Outcomes | Meta-analysis | Funding sources |
|---|---|---|---|---|---|---|---|
| Ali, 2018 | 3 | PRP vs. HA; | Not registered |
Jadad
| Pain | No | No funding |
| Belk, 2020 | 18 | PRP vs. HA | Not registered |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Cavazos, 2019 | 5 | Single injection of PRP vs. multiple injections of PRP | Registered on PROSPERO (CRD42018106429) |
Cochrane RoB tool
| Pain and | Yes | No funding |
| Chen, 2020 | 14 | PRP vs. HA | Not registered |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Chung, 2018 | 5 | PRP vs. placebo; | PROSPERO register (number not reported) |
Cochrane RoB tool
| Pain and | Yes | No funding |
| Costa, 2022 | 40 | PRP vs. HA; | Registered on PROSPERO (CRD42018093247) |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Dai, 2017 | 10 | PRP vs. HA; | Not registered |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Di, 2018 | 7 | PRP vs. HA | Registered on PROSPERO (CRD42016048394) |
Cochrane RoB tool
| Pain and | No | No funding |
| Filardo, 2020 | 34 | PRP vs. placebo; | Registered on PROSPERO (CRD42019145409) |
Cochrane RoB tool 2.0
| Pain, | Yes | No funding |
| Garcia, 2020 | 7 | PRP vs. HA; | Registered on PROSPERO (CRD42020159802) |
Coleman Methodology Score
| Pain, | Yes | No funding |
| Gong, 2021 | 6 | PRP vs. HA | Registered on PROSPERO (CRD42020182571) |
Cochrane RoB tool
| Pain, | Yes | National Natural Science Foundation of China; Scientific Research Project of Chinese Academy of Traditional Chinese Medicine |
| Hohmann, 2020 | 12 | PRP vs. HA | Not registered |
Cochrane RoB tool 1
| Pain and | Yes | No funding |
| Hong, 2021 | 23 | PRP vs. placebo; | Not registered |
Modified version of the Jadad Scale
| Pain, | Yes | Beijing Municipal Science and Technology Commission, the National Natural Science Foundation of China, the National Key Research and Development Program of China, the Capital Health Research and Development of Special |
| Idres, 2023 | 9 | PRP vs. corticosteroids | Not registered |
Cochrane RoB tool
| Pain, | No | No funding |
| Kanchanatawan, 2015 | 9 | PRP vs. HA; | Not registered |
PRISMA
| Pain, | Yes | No funding |
| Kim, 2023 | 21 | PRP vs. HA | PROSPERO (register number not reported) |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Meheux, 2016 | 6 | PRP vs. corticosteroids; | Registered on PROSPERO (CRD42014013032) |
Modified Coleman Methodology Score
| Pain, | No | No funding |
| Nie, 2021 | 21 | PRP vs. corticosteroids; | Registered on PROSPERO (CRD42019122002) |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Peng, 2021 | 14 | PRP vs. HA | Registered on PROSPERO (CRD42022347244) |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Porqueres, 2020 | 4 | PRP vs. HA | Registered on PROSPERO (CRD42014010210) |
Cochrane RoB tool
| Pain, | Yes | No funding |
| Sadabad, 2016 | 6 | PRP vs. HA | Not registered |
Cochrane RoB tool
| Pain | Yes | Health Technology Assessment Department at Shahid Sadoughi University of Medical Sciences, Yazd |
| Sambe, 2023 | 7 | PRP vs. HA | Not registered |
Cochrane RoB tool 2.0
| Pain, | Yes | No funding |
| Sax, 2022 | 24 | PRP vs. CS; | Registered on PROSPERO (CRD42022296909) | Modified Coleman | Pain | Yes | No funding |
| Shang, 2023 | 14 | PRP vs. HA | Not registered |
Jadad
| Pain | Yes | No funding |
| Shen, 2017 | 14 | PRP vs. HA; | Registered on PROSPERO (CRD42016045410) |
Cochrane RoB tool
| Pain, | Yes | National Natural Science Foundation of China and Shanghai Youth Science and Technology start-up grants |
| Simental, 2023 | 14 | PRP vs. placebo | Registered on PROSPERO (CRD42022320169) |
Cochrane RoB tool 2.0
| Pain and | Yes | No funding |
| Tan, 2020 | 26 | PRP vs. HA | Not registered | Modification of the tool used by the Cochrane bone, joint, and | Pain, | Yes | No funding |
| Tao, 2023 | 7 | Single injection of PRP vs. Multiple injections of PRP | Not registered |
Cochrane RoB tool
| Pain and | Yes | No funding |
| Vilchez, 2022 | 31 | PRP vs. HA; | Registered on PROSPERO (CRD42020202048) |
Cochrane RoB tool 2.0
| Pain and | Yes | No funding |
| Xiong, 2023 | 24 | PRP vs. saline solution; | Registered on PROSPERO (CRD42022362066) |
Cochrane RoB tool
| Pain, | Yes | Science and Technology Research Project of Jiangxi Provincial Education |
| Zhao, 2020 | 30 | PRP vs. saline solution; | Registered on PROSPERO (CRD42018100067) |
Cochrane RoB tool
| Pain and | Yes | National Key Research and Development Program of China; the National Natural Science Foundation of China |
| First author, year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 | Overall quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ali, 2018 | Y | N | N | PY | Y | N | N | Y | PY | N | N | N | N | N | N | Y | Critically low |
| Belk, 2020 | Y | N | N | N | Y | Y | N | Y | Y | N | Y | N | N | Y | N | Y | Critically low |
| Cavazos, 2019 | Y | Y | N | Y | Y | Y | N | Y | Y | N | Y | Y | N | Y | N | Y | Critically low |
| Chen, 2020 | Y | N | N | N | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Critically low |
| Chung, 2018 | Y | Y | N | Y | Y | Y | N | Y | Y | N | Y | Y | N | Y | Y | Y | Critically low |
| Costa, 2022 | Y | Y | N | N | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Critically low |
| Dai, 2017 | Y | N | N | Y | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Critically low |
| Di, 2018 | Y | Y | N | N | Y | Y | N | Y | Y | Y | NA | NA | N | N | NA | Y | Critically low |
| Filardo, 2020 | Y | Y | N | Y | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Low |
| Garcia, 2020 | Y | Y | N | N | Y | N | N | Y | N | N | Y | N | N | Y | N | Y | Critically low |
| Gong, 2021 | Y | Y | N | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Low |
| Hohmann, 2020 | Y | N | N | N | Y | Y | N | Y | Y | N | Y | N | N | Y | Y | Y | Critically low |
| Hong ,2021 | Y | N | N | N | N | Y | N | Y | PY | N | Y | N | Y | Y | Y | Y | Critically low |
| Idres, 2023 | Y | N | N | N | Y | Y | N | Y | Y | N | NA | NA | Y | Y | NA | Y | Critically low |
| Kanchanatawan, 2015 | Y | N | N | N | Y | Y | N | Y | N | N | Y | N | Y | Y | Y | Y | Critially low |
| Kim, 2023 | Y | Y | N | PY | Y | N | N | Y | Y | N | Y | Y | N | Y | Y | Y | Critically low |
| Meheux, 2016 | Y | Y | N | N | PY | N | N | Y | N | N | NA | NA | Y | N | NA | Y | Critically low |
| Nie, 2021 | Y | Y | N | N | N | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Critically low |
| Peng, 2021 | Y | Y | N | N | N | N | N | Y | Y | N | Y | Y | N | Y | N | Y | Critically low |
| Porqueres, 2020 | Y | Y | N | N | Y | N | N | Y | Y | N | Y | N | Y | Y | N | Y | Critically low |
| Sadabad, 2016 | Y | N | N | PY | Y | Y | N | Y | Y | N | Y | Y | N | Y | Y | Y | Critically low |
| Sambe, 2023 | Y | N | N | N | N | N | N | Y | Y | N | Y | Y | Y | Y | N | Y | Critically low |
| Sax, 2022 | Y | Y | N | PY | N | N | N | PY | N | N | Y | N | N | Y | N | Y | Critically low |
| Shang, 2023 | Y | N | N | N | Y | Y | N | Y | PY | N | Y | Y | N | Y | N | Y | Critically low |
| Shen, 2017 | Y | Y | N | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Low |
| Simental, 2023 | Y | Y | N | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Low |
| Tan, 2020 | Y | N | N | Y | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Critically low |
| Tao, 2023 | Y | N | N | PY | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Critically low |
| Vilchez, 2022 | Y | Y | N | Y | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | Low |
| Xiong, 2023 | Y | Y | N | Y | Y | Y | N | Y | Y | N | Y | N | N | Y | Y | Y | Critically low |
| Zhao, 2020 | Y | Y | N | PY | N | Y | N | Y | Y | N | Y | N | N | Y | N | Y | Critically low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeriodontal Regeneration and Treatments · Total Knee Arthroplasty Outcomes · Reconstructive Surgery and Microvascular Techniques
Introduction
Health interventions often gain popularity and become the focus of widespread scientific investigation. This is often the ideal scenario for the proliferation of evidence syntheses derived from the results of the numerous clinical trials published on the efficacy and safety of these interventions. A notable example is platelet-rich plasma (PRP) therapy, 1 which involves injecting a solution with a high concentration of an individual's platelets, which is considered promising due to its potential to release growth factors, cytokines, and various substances that induce analgesia, anti-inflammatory, and tissue anabolic effects at the site of application, resulting in a possible renewal of damaged tissue. 2 3 4 In addition, it is a minimally-invasive and easily-accessible technique which has received significant attention in recent years due to the potential benefit of adjuvant treatment for various clinical conditions. In particular, the growing interest in the use of PRP in the treatment of osteoarthritis is highlighted by the importance of synovial inflammation in the pathophysiology and its high prevalence worldwide. 4 5
Given the significant increase in scientific publications on this topic, as expected, the number of systematic reviews on the effects of PRP for osteoarthritis has increased progressively in the last ten years, resulting in a mass of evidence synthesis that often disregards methodological standards and recommendations, compromising the results. 6 7 Given this scenario, meta-research studies emerge as an important tool to establish a connection between good science and its applicability in the clinical practice. 8 9 By gathering and evaluating methodological appropriateness in planning, conducting, and reporting different study designs, meta-research provide information about how common and harmful are certain biases to a research field. 10 In addition to identifying methodological flaws produced and reproduced in the numerous systematic reviews on PRP for osteoarthritis, a meta-research study can direct future efforts toward developing more pertinent and high-quality reviews in this field, increasing the transparency and reproducibility of their findings. 11 12
Thus, the current meta-research study aimed to evaluate the methodological quality of systematic reviews on the benefits and disadvantages of PRP compared to placebo, to other interventions, or to no intervention in the treatment of patients with osteoarthritis.
Materials and Methods
The present study followed the methodological guidance recommended for meta-research studies. 13 To improve reporting quality, the relevant items from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 14 were used. The study protocol was registered on the Open Science Framework (available at: https://doi.org/10.17605/OSF.IO/NZXT9 ).
Criteria to Include Systematic Reviews
Studies identified as systematic reviews on the effects of PRP in the treatment of any type of osteoarthritis were eligible for inclusion. Only those explicitly labelled as “systematic reviews” were considered, while review protocols and systematic reviews incorporating observational study designs were excluded. Additionally, systematic reviews available only as abstracts or in incomplete formats were excluded.
Information Sources
To identify eligible systematic reviews, we conducted a comprehensive search on January 31, 2024, on the following electronic databases: Medical Literature Analysis and Retrieval System Online (MEDLINE, via Pubmed), The Cochrane Library (Cochrane Database of Systematic Reviews, CDSR), Excerpta Medica Database (Embase, via Elsevier), and Epistemonikos. No restrictions on publication date or language were applied. The detailed search strategies are presented in Table 1 .
Study Selection
A pair of reviewers (MEO and MLA) analyzed the title and abstract of the references obtained with the search strategy. This initial screening was performed through the Rayyan (Qatar Computing Research Institute, Doha, Qatar) application, 15 which enabled the evaluation process to occur independently. After that first stage, the full text of the studies classified as potentially included was thoroughly examined. Any conflicts in both stages were resolved through a third reviewer. The excluded studies were recorded in the table of excluded studies, accompanied by the respective reasons for exclusion ( Table 2 ). Two independent reviewers used a pre-established data extraction form to collect data from the included studies. Following this process, a third reviewer (ALCM) resolved potential inconsistencies.
Data Extraction
For eligible systematic reviews, we extracted the following information: year of publication, number of included studies, aspects of the intervention and comparators, review protocol, tool used to assess methodological quality, outcomes, if meta-analyses were conducted, and funding sources. The authors evaluated several systematic reviews that assessed the certainty of the body of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach 16 and the adequacy of the protocol registration regarding selective reporting bias.
Methodological Quality Evaluation of the Included Studies
We used A Measurement Tool to Assess Systematic Reviews, Version 2 (AMSTAR-2) tool 17 to critically assess the methodological quality of the systematic reviews. The tool has 16 items, and after an overall assessment of the systematic reviews, the study was categorized into four quality levels: critically-low, low, moderate, and high, depending on the weaknesses detected in critical and non-critical items. Two independent reviewers (KMMS and MES) conducted the AMSTAR-2 assessment; a third reviewer (EMS) was consulted in case of disagreements.
Synthesis of the Results
The methodological characteristics of the included systematic reviews were tabulated and summarized descriptively using a Microsoft Excel (Microsoft Corp., Redmond, WA, United States) spreadsheet. Data were expressed as absolute and relative frequencies.
Results
Search Results
With the search strategies, we initially retrieved 485 references. After eliminating 166 duplicates, 319 references underwent title and abstract screening. Thus, 31 systematic reviews met the eligibility criteria and were included in the present meta-research study ( Fig. 1 ).
Flowchart of the study selection process.
Baseline Characteristics
Table 3 presents the detailed characteristics of the included systematic reviews, which assessed between 3 and 40 randomized clinical trials (RCTs) on the effects of PRP compared to placebo or other therapies. These reviews were published from 2015 to 2023, with the highest number of study publications in 2020. 18 19 20 21 22 23 24
Almost half of the reviews registered their protocol on the International Prospective Register of Systematic Reviews (PROSPERO), although two did not report the registration number. Meta-analyses were conducted in 87% (27/31) of the reviews. The RCT methodological quality tool most used was the Cochrane Risk of Bias Tool (RoB) (68%; 21/31). Regarding financial support, 80.64% (25/31) of the included reviews stated that there were no funding sources nor conflicts of interest.
Methodological Quality of the Included Systematic Reviews
In the assessment of methodological quality using the AMSTAR-2 tool, 83.8% (26/31) of the systematic reviews were classified as having critically-low quality, followed by 16.13% (5/31) classified as low quality. Details of this assessment are presented in Table 4 , and Fig. 2 shows the frequency of adherence to each AMSTAR-2 item.
Proportion of categories of methodological quality according to the A Measurement Tool to Assess Systematic Reviews, Version 2 (AMSTAR-2) tool. Abbreviation: Q: question. Notes: Q1–about the Patient, Intervention, Comparison, Outcome (PICO) strategy; Q2–about protocol a priori; Q3–about study design for inclusion; Q4–about search strategy; Q5–about study selection; Q6–about data extraction; Q7–about list of excluded studies; Q8–about description of the the included studies; Q9–about method to assessing the risk of bias; Q10–about funding of included studies; Q11–about methods for statistical combination; Q12–about impact of risk of bias in individual studies on meta-analysis; Q13–about discussion of risk of bias in individual studies; Q14–about heterogeneity; Q15–about publication bias; and Q16–about conflict of interest.
The current study revealed a significant increase in the number of systematic reviews over the years, with most exhibiting critically-low quality, except for 2017 ( Fig. 3 ).
Number of systematic reviews classified as having low and critically-low quality by year.
Among the critical items assessed in the AMSTAR-2, items 4 and 7 emerged as particularly significant in the present evaluation:
Item 4: 48.3% (15/31) received a “no” response, and 29% (9/31) received a “partially yes” response regarding the performance of a comprehensive and adequate literature search. No systematic review classified as presenting low methodological quality received a negative score in this item, and 57.7% of those classified as “critically low” received “no” (15/31) answers. Reviews that exhibited deficiencies in the literature search were primarily hindered by language restrictions, as evidenced by 38% (12/31) that limited their search only to RCTs written in English. Additionally, 11 reviews that received a poor score on this criterion failed to use trial registry platforms such as ClinicalTrials.gov in their search strategy.Item 7: 100% (31/31) did not inform the reasons for excluding RCTs during the study selection process.
Systematic Reviews that Assessed the Certainty of the Evidence (GRADE approach)
Upon reviewing the AMSTAR-2 tool, we found no mention of assessmets of the certainty of evidence. However, we extracted additional data and found that only 19.35% (6/31) of the included systematic reviews conducted this assessment according to the GRADE approach; however, the complete assessment of each GRADE domain was not fully reported.
Discussion
Given the significant impact of systematic reviews on clinical recommendations and the development of medical guidelines, they must be conducted using methods that transparently minimize errors and biases. 25 However, despite the widespread dissemination of tools, such as the Cochrane Handbook of Systematic Reviews and the PRISMA statement, 14 26 27 28 and the increasing production of systematic reviews over the years, many reviews are still poorly conducted and exhibit a high risk of bias. 29 This finding aligns with the results of the current meta-research study, which observed an increase in reviews on PRP since 2015 but no improvement in their methodological and reporting quality.
As previously mentioned, 83.8% (26/31) of the included systematic reviews received an overall classification of critically-low quality and 16.13% (5/31) were classified as low-quality according to the AMSTAR-2 tool criteria. Considering the critical items, those most inadequately reported are related to search strategies (item 4), with 77,3% of “no” or “partially yes” responses, and the reasons for the exclusion of studies during the selection process (item 7), which was not described in 100% (31/31) of the reviews. Additionally, 42% did not mention the review protocol registry (item 2), 13% did not use the adequate methodological quality tool to assess the risk of bias in RCTs (item 9), 3.5% did not use appropriate statistical methods (item 11), 35.7% did not assess the impact of the RCT's risk of bias on the results (item 12), and 45.2% did not consider the risk of bias in interpreting the data obtained in the discussion section (item 13). Therefore, 32.26% did not meet the item 15 criteria, which involved a plan to investigate publication bias and discuss its impact on the systematic review results. It is important to mention that 100% (31/31) of the included reviews did not report reasons for choosing only RCT to be included in the review (item 3), and 93.5% did not mention the funding sources of their respective included RCTs (item 10). Also, the GRADE approach was used in only 19.3% of the reviews.
Despite methodological recommendations encouraging pre-established protocols for systematic reviews, 29 half of the PRP reviews examined in the present study did not register their protocols beforehand. Without this registration, it is not possible to compare the results obtained with those intended, which compromises the evaluation of possible protocol deviations, 30 and also hinders the to identification of redundancy of systematic reviews on a similar topic without additional contributions. 31
Another topic observed was the absence of a list of excluded references and detailed justifications in all analyzed systematic reviews. This indicates a potential transparency failure in the study selection process. 17 Due to this omission, the interpretation of the results can be underestimated or overestimated. 32
Regarding the design of the studies included in the evaluated systematic reviews (AMSTAR-2, item 3), 100% (31/31) of the reviews did not clarify in the article that this is the best study design to answer research questions. As it is well established, RCTs are considered the gold-standard type of study and the most reliable to test interventions. 33 Therefore, it is assumed that this information is already a consensus, and the authors do not mention it in the text of their reviews.
Almost half of the reviews also conducted search strategies incompletely. In systematic reviews, search strategies involve multiple stages that must be transparent to the reader. Limiting language, mainly selecting only studies written in English, leads to monolingual bias and the potential loss of relevant studies. 32 33 34 35
Even though adherence to the risk of bias tool was high among the systematic reviews on PRP investigated, some studies did not consider the RCTs' risk of bias results in the meta-analysis and discussion, making their conclusions weak. A cross-sectional study 36 showed that efficacy studies with a high risk of bias tend to present higher effect estimates than those with low bias.
No meta-research studies on PRP to treat osteoarthritis were identified. However, a study 37 assessed the methodological quality of systematic reviews in the orthopedic field across the top five impact factor journals between 2006 and 2010. This study 37 revealed that the main areas of deviation were the protocol registry and the assessment of publication bias likelihood, with only 54% of methodological components being fulfilled.
In addition, most reviews (80.6%) did not employ the GRADE approach to assess the certainty of the evidence. Failure to acknowledge evidence certainty and the strength of recommendation through the GRADE approach can lead to misguided guidelines and recommendations, negatively impacting patient health. 38 Due to its critical importance, we suggest that GRADE assessment be included as an item in a future version of the AMSTAR tool.
For the present study, a comprehensive literature search was conducted without date and language restrictions. However, it is possible that eligible reviews were eventually missed. Nevertheless, the decision to include systematic reviews involving only RCTs was due to the excessive number of clinical trials on the topic in question, considering the best primary study to assess the effects of therapeutic interventions. It is important to emphasize that, as meta-research, a sample of studies on the topic was analyzed to generate an overview of the current methodological situation of the published articles.
Conclusion
The methodological quality of the systematic reviews on the effects of PRP in the treatment of osteoarthritis was classified as having low and critically-low quality through the AMSTAR-2 assessment. Furthermore, most of them did not assess the certainty of the evidence using the GRADE approach. Despite the numerous systematic reviews conducted on this topic over the years, the current study identified that most of these reviews are not rigorously planned and conducted, presenting methodological flaws that could affect the reliability of the clinical findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bennell K L Hunter D J Paterson K L Platelet-Rich Plasma for the Management of Hip and Knee Osteoarthritis Curr Rheumatol Rep 201719052428386761 10.1007/s 11926-017-0652-x · doi ↗ · pubmed ↗
- 2Shirokova K Gorokhkova V Shirokova L The impact of the administration of PRP and disease-modifying therapy on the synovial environment, general health and treatment efficacy in patients with osteoarthritis of the knee Osteoarthritis Cartilage 20192701502503
- 3Rodríguez-Merchán E C Intra-Articular Platelet-Rich Plasma Injections in Knee Osteoarthritis: A Review of Their Current Molecular Mechanisms of Action and Their Degree of Efficacy Int J Mol Sci 20222303130135163225 10.3390/ijms 23031301 PMC 8836227 · doi ↗ · pubmed ↗
- 4Tonutti A Granata V Marrella V The role of WNT and IL-1 signaling in osteoarthritis: therapeutic implications for platelet-rich plasma therapy Front Aging 202341.201019 E 610.3389/fragi.2023.1201019 PMC 1028566737362206 · doi ↗ · pubmed ↗
- 5Liu-Bryan R Synovium and the innate inflammatory network in osteoarthritis progression Curr Rheumatol Rep 2013150532323516014 10.1007/s 11926-013-0323-5PMC 3643293 · doi ↗ · pubmed ↗
- 6Page M J Moher D Mass Production of Systematic Reviews and Meta-analyses: An Exercise in Mega-silliness?Milbank Q 2016940351551927620684 10.1111/1468-0009.12211 PMC 5020155 · doi ↗ · pubmed ↗
- 7Ioannidis J P The Mass Production of Redundant, Misleading, and Conflicted Systematic Reviews and Meta-analyses Milbank Q 2016940348551427620683 10.1111/1468-0009.12210 PMC 5020151 · doi ↗ · pubmed ↗
- 8Zhang Z Meta-epidemiological study: a step-by-step approach by using RJ Evid Based Med 2016902919726924387 10.1111/jebm.12191 · doi ↗ · pubmed ↗