Aortoenteric Fistula: An Uncommon but Life-Threatening Complication of Pledget Use in Hiatal Hernia Repair
Jeet H Patel, Parag Brahmbhatt, Kalpit Devani, Jena Velji-Ibrahim

TL;DR
A rare case of a life-threatening aortoenteric fistula caused by a Teflon pledget used in hiatal hernia surgery is reported, highlighting the need for awareness and preventive measures.
Contribution
This paper presents a rare complication of Teflon pledget erosion and offers insights into its prevention.
Findings
A 74-year-old female developed an aortoenteric fistula due to erosion of a Teflon pledget.
TEVAR and endoscopic removal of the pledget successfully treated the complication.
The paper discusses causes of pledget erosion and possible countermeasures.
Abstract
The standard treatment for hiatal hernia repair and gastroesophageal reflux disease (GERD) is laparoscopic Nissen fundoplication, in which a Teflon pledget (TP) is used to buttress the hiatal hernia. We present an extremely rare case in which a 74-year-old female developed a postoperative aortoenteric fistula due to erosion of a TP used during paraesophageal hernia repair. A computed tomography (CT) angiogram and esophagogastroduodenoscopy (EGD) confirmed the diagnosis. Subsequently, a thoracic endovascular aortic repair (TEVAR) was performed to treat the aortoenteric fistula, and the TP was removed using a raptor grasping device and scissors during a repeat EGD at a tertiary care center. In this article, we discuss different causes of TP erosion and possible countermeasures that may help prevent such complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
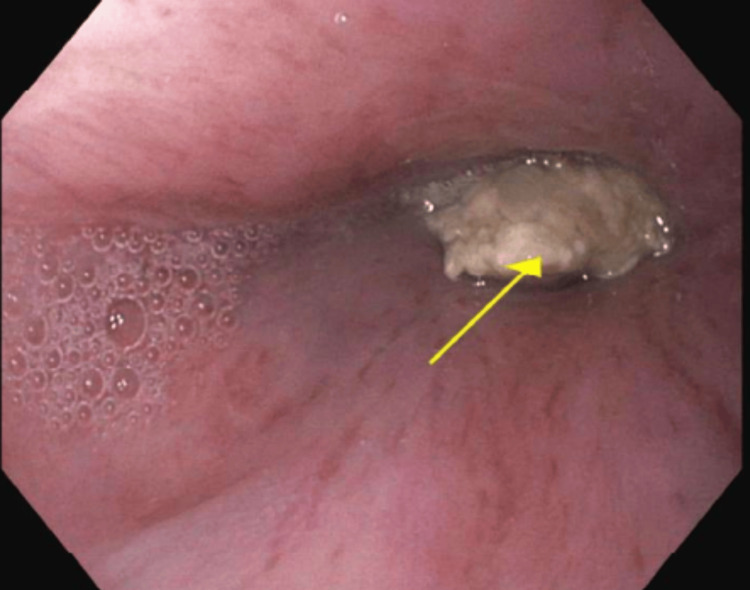 Figure 1
Figure 1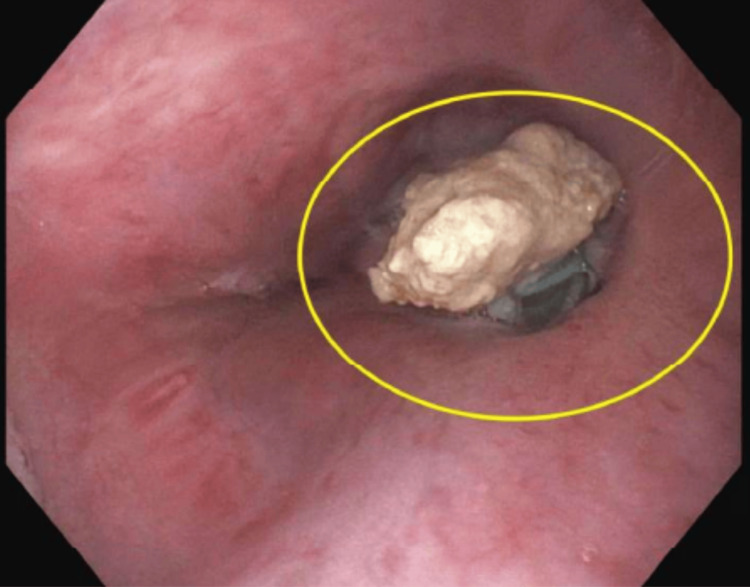 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastroesophageal reflux and treatments · Biliary and Gastrointestinal Fistulas
Introduction
Laparoscopic Nissen fundoplication has become a standard treatment for hiatal hernia repair and gastroesophageal reflux disease (GERD). A Teflon pledget (TP) is used in this procedure as a buttress under sutures to prevent tearing of the tissue, particularly in areas containing blood vessels, and to distribute tension evenly. According to previous studies, approximately 90% of patients undergoing laparoscopic fundoplication have had positive outcomes, and postoperative TP-related complications are rare. Among those rare cases, common late postoperative complications include gas-bloat syndrome (up to 85%), dysphagia (10%-50%), diarrhea (18%-33%), and recurrent heartburn (10%-62%) [1-6]. We present an extremely rare case in which a patient developed postoperative acute anemia due to an aortoenteric fistula caused by the TP used during paraesophageal hernia repair. A review of the current literature has not revealed any similar cases related to laparoscopic Nissen fundoplication.
Case presentation
A 74-year-old female was referred to a general surgeon for a paraesophageal hernia repair due to a history of refractory/recurrent episodes of LA grade C esophagitis with previous significant nonsteroidal anti-inflammatory drug (NSAID) use and GERD-related symptoms. Proton pump inhibitors (PPIs) were unsuccessful in relieving her of heartburn and regurgitation symptoms. She had undergone multiple endoscopies in the past, which indicated moderate to large hiatal hernia/paraesophageal hernia.
On January 24, 2024, she underwent robotic reduction of paraesophageal hiatal hernia with type II mediastinal dissection, primary repair of hiatal hernia, anterior and posterior gastropexy, Toupet fundoplication, and mesh reinforcement with surgical TPs.
On March 13, 2024, she presented due to a sudden episode of dizziness and nausea in the emergency department. Her vitals at that time were measured as blood pressure (BP): 101 mmHg/85 mmHg (reference range systolic: <120 mmHg, diastolic: <80 mmHg), pulse (P): 118 beats per minute (reference range 60-100 beats per minute), and respiratory rate (RR): 22 breaths per minute (reference range 12-20 breaths per minute). The lab results were normal except for her hemoglobin levels, which were 11.9 g/dL (reference range: 12.1-15.1 g/dL). She was subsequently discharged from care and sent home with conservative management. On March 21, 2024, she returned complaining of severe back pain and nausea. She presented with BP: 109 mmHg/67 mmHg (reference range systolic: <120 mmHg, diastolic: <80 mmHg), P: 72 beats per minute (reference range 60-100 beats per minute), and RR: 24 breaths per minute (reference range 12-20 breaths per minute). On further inquiry, she also complained of black/dark stools but was on iron supplementation. The lab results at the time were normal except for her hemoglobin levels, which were 5.2 g/dL (reference range: 12.1-15.1 g/dL), and her lactic acid levels were greater than 9 mmol/L (reference range <2 mmol/L). Subsequent computed tomography (CT) angiogram revealed findings suspicious for contained gastroesophageal perforation versus developing/early outer gastroesophageal fistula with abundant blood product in the lumen of the stomach. After a surgical consultation, esophagogastroduodenoscopy (EGD) was performed, and one large cratered esophageal ulcer with no active bleeding was discovered, 35 cm from the incisors. The ulcer seemed suspicious for a visible vessel or aorto-esophageal fistula; however, it was decided that advancing the scope further should be avoided as it could disrupt the clot and initiate bleeding.
Furthermore, the patient was also seen by a vascular surgeon whose interpretation of the CT angiogram indicated a concerning aortoenteric fistula, which may have been the cause of her prior bleeding episodes. Subsequently, the patient underwent an urgent thoracic endovascular aortic repair (TEVAR) for possible aortoenteric fistula as well as celiac artery stenting. Thereafter, she was given total parenteral nutrition (TPN) and had a gastrostomy tube (G-tube) placement on March 27, 2024, to avoid further complications. Nevertheless, she developed a peripherally inserted central catheter (PICC) line-associated deep vein thrombosis (DVT) requiring Eliquis therapy and was additionally placed on lifelong antibiotics due to the aortic stenting.
In August of 2024, she underwent a repeat EGD at a tertiary care center and was found to have a large suture TP (Figure 1, 2) implanted at 37 cm, which was removed with a raptor grasping device and scissors. The patient has been stable since, indicating that the pledget erosion was the cause of the aortoenteric complication, which led to her acute anemia episodes.
The arrow indicates the superficial border of the Teflon pledget discovered during repeat esophagogastroduodenoscopy at a tertiary care center.
The white structure in this figure is the eroded Teflon pledget discovered during the repeat esophagogastroduodenoscopy at a tertiary care center.
Discussion
The patient presented with acute anemia-related symptoms. An EGD and CT angiogram revealed an incidence of aortoenteric fistula. A repeat EGD confirmed the cause of the aortoenteric fistula to be the erosion of a TP used during the paraesophageal hernia repair procedure. TP-related complications are rare. Thus, finding relevant articles discussing this issue poses a challenge. A PubMed search, using the parameters “Teflon pledget and fistula” and “Teflon pledget and erosion” for a timeline between 1980 and 2024 revealed only two relevant articles. The first article involved a case report in which purulent drainage was noted from the formation of a cardiocutaneous fistula due to a TP that had been used six years earlier on the heart suture line for left ventricular aneurysm repair [7]. The second relevant article involved a case report where a patient presented with postoperative dysphagia because of an esophagogastric fistula, which was caused by the erosion of a TP four weeks after a laparoscopic fundoplication procedure [8]. No relevant literature regarding patients presenting with acute anemia due to TP use was found, further demonstrating how rare this case is.
As discussed previously, fistula formation due to TP is an extremely rare phenomenon, and the cause of TP erosion remains unclear. One possible explanation could be ischemic necrosis caused by over-compact suturing. In one case study, a Teflon membrane placed anterior to the uterus to prevent adhesions post-myomectomy eroded into the bladder four years later. In that case, they speculated that ischemia was due to the use of a compact suture to retain the patch, which eventually led to fistula formation and local sepsis [9].
Another possible cause of TP erosion could be infection resulting from the use of TP. A case report from 1999 presented a patient who developed a cardiocutaneous fistula extending through the left hemidiaphragm and draining at the abdominal wall six years after a ventricular aneurysmectomy. The cause of TP erosion, which led to the cardiocutaneous fistula, was theorized to be a delayed infection from the suture line involving TP [7].
Lastly, another possible explanation for this phenomenon could be an inflammatory reaction to the TP. A case report from 2000 presented a patient with postoperative dysphagia caused by an esophagogastric fistula resulting from the erosion of TP. In that case, the authors speculated that an inflammatory response to the TP may have contributed to the complication [8].
A possible solution to prevent erosion of pledgets could be to use absorbable pledgets, such as polyglycolic acid (PGA) pledgets. A review of the current literature revealed no studies in which absorbable pledgets were used for laparoscopic Nissen fundoplication. However, one study did explore the use of PGA pledgets to repair bronchus, lung fistula, and pleural defects in approximately 50 dogs. That evaluation suggested that PGA pledgets were a better alternative to conventional non-absorbable pledgets for pulmonary procedures [10].
Conclusions
In sum, absent conclusive evidence, mere speculations regarding the causes of TP erosion are insufficient to establish the theoretical reasons discussed above. Furthermore, TP use to buttress hiatal hernia repair will likely remain part of the standard procedure, as most patients experience successful outcomes. However, despite the lack of literature and evidence surrounding the use of PGA pledgets, we believe that resorbable pledgets could be a potential future alternative to TP to reduce complications. We hope that this article draws attention from other surgeons who may face similar challenges.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Use of mesh in laparoscopic paraesophageal hernia repair: a meta-analysis and risk-benefit analysis P Lo S One Müller-Stich BP Kenngott HG Gondan M 010201510.1371/journal.pone.0139547 PMC 460749226469286 · doi ↗ · pubmed ↗
- 2Cost effectiveness of medical versus surgical treatment in patients with severe or refractory gastroesophageal reflux disease in the Netherlands Scand J Gastroenterol Van Den Boom G Go PM Hameeteman W Dallemagne B Ament AJ 19311996892793310.3109/00365529609031619 · doi ↗ · pubmed ↗
- 3A rare and late postoperative complication of Nissen fundoplication: mixed hiatus hernia Euroasian J Hepatogastroenterol Kekilli M Dogan Z Karaahmet F 172820183082856110.5005/jp-journals-10018-1285 PMC 6395488 · doi ↗ · pubmed ↗
- 4Laparoscopic Nissen fundoplication: operative results and short-term follow-up Am J Surg Bittner HB Meyers WC Brazer SR Pappas TN 1931981671994831113210.1016/0002-9610(94)90073-6 · doi ↗ · pubmed ↗
- 5Teflon pledget reinforced fundoplication causes symptomatic gastric and esophageal lumenal penetration Am J Surg Dally E Falk GL 22622918720041476930910.1016/j.amjsurg.2003.11.028 · doi ↗ · pubmed ↗
- 6Gastroesophageal reflux disease treatment: side effects and complications of fundoplication Clin Gastroenterol Hepatol Richter JE 4654711120132326786810.1016/j.cgh.2012.12.006 · doi ↗ · pubmed ↗
- 7Cardiocutaneous fistula Heart Danias PG Lehman T Kartis T Missri JC 3253268119991002636610.1136/hrt.81.3.325PMC 1728979 · doi ↗ · pubmed ↗
- 8Esophagogastric fistula secondary to teflon pledget: a rare complication following laparoscopic fundoplication Dis Esophagus Baladas HG Smith GS Richardson MA Dempsey MB Falk GL 72741320001100533610.1046/j.1442-2050.2000.00083.x · doi ↗ · pubmed ↗