The Hidden Cost of Bariatric Surgery: Wernicke’s Encephalopathy and Polyneuropathy
Lailus Sabikunnahar Mishu, Esraa Abuelgassem Hagahmed Mohamed, Tochukwu Samuel Odogwu, Muhammad Aftab Toor, NoimUddin Jibon

TL;DR
Bariatric surgery can lead to serious neurological issues due to thiamine deficiency, highlighting the need for better nutritional monitoring and patient education.
Contribution
This case report highlights the risk of thiamine deficiency post-bariatric surgery and advocates for improved preoperative and postoperative nutritional management.
Findings
A 27-year-old patient developed neurological symptoms due to thiamine deficiency after gastric sleeve surgery.
Thiamine deficiency can lead to Wernicke’s encephalopathy and polyneuropathy, which are often overlooked post-bariatric surgery.
The report underscores the importance of nutritional monitoring and supplementation to prevent such complications.
Abstract
Bariatric surgery is a recognised intervention for severe obesity, a global epidemic associated with numerous comorbidities like diabetes, hypertension, and cardiovascular diseases. Procedures such as Roux-en-Y gastric bypass facilitate significant weight loss, improving metabolic health and quality of life. However, these surgeries carry hidden costs, particularly concerning nutritional deficiencies that are often overlooked in preoperative assessments. This case report presents a 27-year-old patient who, after undergoing gastric sleeve surgery, developed neurological symptoms due to thiamine deficiency. Thiamine, essential for energy metabolism, is crucial for neurological function, and its deficiency can lead to serious conditions like Wernicke’s encephalopathy and polyneuropathy. Despite the initial success of the surgery, the patient faced significant morbidity due to this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
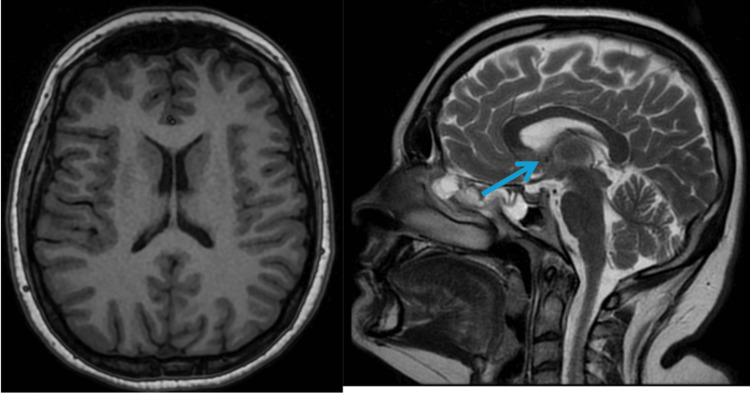 Figure 1
Figure 1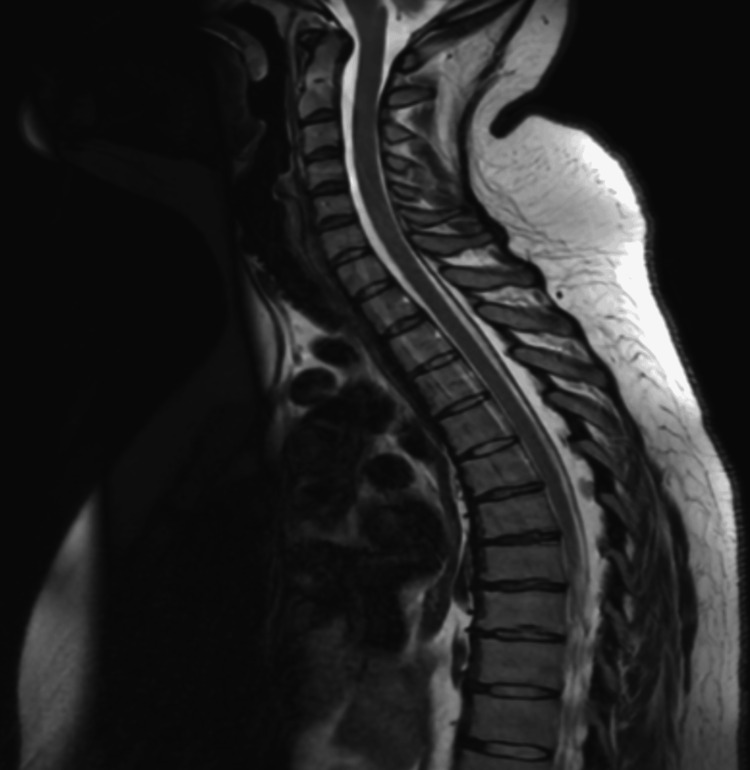 Figure 2
Figure 2 Figure 3
Figure 3| Nerve and Site | Onset Latency | Peak Latency | Amplitude | Segment | Latency Difference | Distance | Conduction Velocity |
| Median - R | |||||||
| Dig-II | NR | NR | NR | Dig-II-Wrist | ms | mm | m/s |
| Dig-III | NR | NR | NR | Dig-III-Wrist | ms | mm | m/s |
| Ulnar - R | |||||||
| Dig V | NR | NR | NR | Dig-V-Wrist | ms | mm | m/s |
| Radial - R | |||||||
| Forearm | NR | NR | NR | Forearm-wrist | ms | mm | m/s |
| Radial - L | |||||||
| Forearm | NR | NR | NR | Forearm-wrist | ms | mm | m/s |
| Median - R | |||||||
| Wrist | NR | NR | NR | Wrist-Dig-II | ms | mm | m/s |
| Ulnar - R | |||||||
| Wrist | 1.9 ms | 2.5 ms | 14 μv | Wrist-Dig-V | 1.9 ms | 100 mm | 54 m/s |
| Sural - R | |||||||
| Calf | NR | NR | NR | Calf-ankle | ms | mm | m/s |
| Superficial peroneal - R | |||||||
| Calf | NR | NR | NR | Calf-ankle | ms | mm | m/s |
| Sural - L | |||||||
| Calf | NR | NR | NR | Calf-ankle | ms | mm | m/s |
| Superficial peroneal - L | |||||||
| Calf | NR | NR | NR | Calf-ankle | ms | mm | m/s |
| Nerve and Site | Latency | Amplitude | Segment | Latency Difference | Distance | Conduction Velocity |
| Median - R | ||||||
| Wrist | NR | NR | Abductor pollicis brevis-wrist | ms | mm | m/s |
| Ulnar - R | ||||||
| Wrist | 2.3 ms | 5.7 mV | Wrist-Abductor digiti minimi | 2.3 ms | mm | m/s |
| Below elbow | 6.9 ms | 5.0 mV | Wrist-Below elbow | 4.6 ms | 210 mm | 46 m/s |
| Above elbow | 8.3 ms | 3.9 mV | Below elbow-Above elbow | 1.4 ms | 60 mm | 43 m/s |
| Median - L | ||||||
| Wrist | NR | NR | Abductor pollicis brevis-wrist | ms | mm | m/s |
| Ulnar - L | ||||||
| Wrist | 3.3ms | 0.3mV | Wrist-Abductor Digiti minimi | 3.3 ms | mm | m/s |
| Peroneal - R | ||||||
| Ankle | NR | NR | Ankle-Extensor digitorum brevis | ms | mm | m/s |
| Peroneal - L | ||||||
| Ankle | NR | NR | Ankle-Extensor digitorum brevis | ms | mm | m/s |
| Tibial - R | ||||||
| Ankle | 5.0 ms | 0.2 mV | Ankle-Abductor hallucis | 5.0 ms | mm | m/s |
| Tibial - L | ||||||
| Ankle | 4.7 ms | 0.1 mV | Ankle-Abductor hallucis | 4.7 ms | mm | m/s |
| Nerve | M-Latency | F-Latency |
| Ulnar - R | 2.3 | 30.4 |
| Insertional | Spontaneous and/or Volitional Activity | Maximum Volitional Activity | ||||||||
| Muscle | Insertional | Fibs | +Wave | Fasc | Duration | Amplitude | Poly | Amplitude | Pattern | Effort |
| Tibialis anterior - R | Increased | 4+ | 4+ | None | No Vol MU | No Vol MU | None | No Vol MU | None | Max. |
| Vastus lateralis - R | Increased | 4+ | 4+ | None | No Vol MU | No Vol MU | None | Normal | None | Max. |
| Gastrocnemius - R | Increased | 4+ | 4+ | None | Normal | Normal | None | Normal | Single unit | Max. |
| Tibialis anterior - L | Increased | 4+ | 4+ | None | No Vol MU | No Vol MU | None | No Vol MU | Single unit | Max. |
| Vastus lateralis - L | Increased | 4+ | 4+ | None | No Vol MU | No Vol MU | None | No Vol MU | None | Max. |
| 1st dorsal interosseous - R | Normal | None | None | None | Normal | None | Normal | Reduced | Max. | |
| Extensor digitorum communis - R | Increased | 4+ | 4+ | None | No Vol MU | No Vol MU | None | No Vol MU | None | Max. |
| Deltoid - R | Increased | None | None | None | Normal | Normal | None | Normal | Full | Max. |
| Extensor digitorum communis - L | Increased | 4+ | 4+ | None | No Vol MU | No Vol MU | None | No Vol MU | None | Max. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Alcoholism and Thiamine Deficiency · Diet and metabolism studies
Introduction
Obesity is a significant global health challenge, contributing to chronic conditions such as cardiovascular disease, diabetes, and obstructive sleep apnoea (OSA), which increase morbidity and mortality [1]. For severe obesity (BMI ≥ 40 kg/m² or ≥35 kg/m² with comorbidities), bariatric surgery remains the most effective treatment for sustained weight loss [2]. Sleeve gastrectomy (SG), a widely performed procedure, reduces gastric volume and alters gut hormone secretion, though its anatomical changes also predispose patients to micronutrient deficiencies [3].
Among these deficiencies, thiamine (vitamin B1) deficiency is particularly consequential, as it can lead to Wernicke’s encephalopathy (WE) and polyneuropathy-neurological emergencies often underrecognised in post-bariatric patients [4]. WE classically presents with confusion, ataxia, and ophthalmoplegia (though the full triad is rare), and untreated cases may progress to irreversible Korsakoff syndrome. This risk is exacerbated in settings with poor post-operative monitoring, such as medical tourism, where adherence to supplementation guidelines is inconsistent [5].
While guidelines (e.g., American Society for Metabolic and Bariatric Surgery (ASMBS)) recommend lifelong thiamine supplementation (≥12 mg/day) and multidisciplinary follow-up [4,5], cases of WE persist due to delayed diagnosis or inadequate care. We present a case highlighting this preventable complication, emphasising the need for heightened clinical vigilance and patient education post-SG.
Case presentation
A 27-year-old lady underwent gastric sleeve surgery abroad in February 2024 for the management of morbid obesity. The surgery was performed outside the United Kingdom, and the patient had no known history of nutritional deficiencies. She was not taking any nutritional supplements prior to the procedure. However, details of her preoperative nutritional screening were unavailable, as the evaluation was conducted abroad, and she was not enrolled in any post-operative follow-up programme. Within three months of the procedure, the patient presented to the Emergency Department with recurrent falls and progressive bilateral lower limb weakness. The symptoms initially manifested as weakness and paraesthesia in the feet, which gradually ascended proximally, leading to impaired ambulation. She was initially diagnosed with acute neuropathy with demyelination (Guillain Barre Syndrome) following review by neurologists. She was managed with intravenous immunoglobulins while on admission to the acute medical unit.
Initial laboratory investigations revealed a haemoglobin level of 137 g/L, red cell distribution width (RDW) of 18.0, and a white blood cell count of 7.3 × 10⁹/L, with normal neutrophil and lymphocyte counts. A venous blood gas showed a normal level of bicarbonate and lactate. Cerebrospinal fluid (CSF) analysis demonstrated clear, colourless fluid with a white cell count of 12, total protein of 0.40 g/L, and glucose level of 3.8 mmol/L. No organisms were identified on culture. Extensive viral PCR testing was negative for herpes simplex virus types I and II, varicella-zoster virus, enterovirus, and parechovirus. Serum vitamin B12 level was elevated at 732 pmol/L, and folate was within normal limits at 8.1 nmol/L. Myeloma screening performed during the admission yielded normal results.
MRI head and whole spine in Figures 1-3 was done to rule out intracranial or spinal pathologies. The only abnormality noted was mild diffuse disc bulging at L4/L5 Figure 3 without any significant neural compression. She was discharged after 7 days in the AMU with outpatient follow-up, electromyography (EMG) and nerve conduction studies appointments. The patient re-presented to the Emergency Department within one week with new-onset ophthalmoplegia and diplopia, along with worsening lower limb symptoms that had progressed to include upper limb numbness and weakness. On admission, she also exhibited diaphragmatic weakness, with type-2 respiratory failure on arterial blood gas (ABG) necessitating non-invasive ventilation (NIV) due to a reduced vital capacity of 1.2 L, though this later improved. MRI of the brain in Figure 1 was reported as normal, though there was some debate regarding a subtle abnormality in the mammillary bodies, which favours the diagnosis of WE. MRI of the spinal cord was unremarkable in Figures 2-3. EMG revealed a severe axonal neuropathy with distal predominance in Tables 1-4 and sleep study ruled out any OSA. Based on these findings, she was diagnosed with WE and associated polyneuropathy due to thiamine deficiency. She received aggressive treatment with intravenous Pabrinex over the course of one month. A blood sample was collected later for thiamine level, after the intensive thiamine therapy, and the result was normal - 292. A formal cognitive assessment identified deficits in memory, though these have gradually improved over time, as has her ataxia. She was subsequently transferred to specialist Inpatient neurological rehabilitation.
MRI Brain - Cross-sectional & Sagittal ViewsReported as normal.
MRI Cervical and Thoracic Spines.Reported as normal.
MRI of Lumbosacral Spine Showing Mild Diffuse Disc Bulging of L4/L5 Without Significant Neural Compression
However, she continues to experience significant motor and sensory neuropathy, with persistent marked weakness, particularly affecting her hands and wrists. Given the severity of her neuropathy, clinical recovery is expected to be slow and prolonged.
Discussion
Thiamine (vitamin B1) deficiency, though rare in the general population, is a well-documented complication following bariatric surgery, with prevalence rates ranging from 18% to 49% in post-operative patients [6]. This case highlights the critical importance of recognising and addressing thiamine deficiency early to prevent severe neurological sequelae such as WE and polyneuropathy.
WE is a medical emergency and the complete triad is present in only about 16% of cases [7]. In this patient, the initial presentation of recurrent falls, bilateral lower limb weakness, and subsequent development of ophthalmoplegia and diplopia were indicative of WE, though the diagnosis was initially missed. This delay in diagnosis is not uncommon, as the symptoms of WE can be nonspecific and overlap with other neurological conditions, such as Guillain-Barré syndrome, which was initially suspected in this case. The prevalence of WE following bariatric surgery is estimated to be between 0.2% and 2%, though this may be an underestimation due to under-diagnosis and misdiagnosis [6].
Thiamine deficiency in bariatric surgery patients stems from malabsorption due to anatomical changes, post-operative vomiting, reduced intake, and poor supplementation adherence [8, 9]. In this case, SG increased deficiency risks due to reduced food intake and malabsorption. The patient’s rapid progression to severe neurological symptoms within three months post-surgery underscores the need for vigilant monitoring and early intervention.
The management of WE requires aggressive thiamine replacement therapy, typically administered intravenously in the form of Pabrinex, as was done in this case. Early treatment is crucial to prevent the progression to Korsakoff syndrome, a chronic and often irreversible condition characterised by severe memory impairment and confabulation [7]. In this patient, the initiation of intravenous thiamine led to gradual improvement in cognitive function and ataxia, though significant motor and sensory neuropathy persisted. This underscores the importance of early recognition and treatment, as delayed intervention can result in long-term neurological deficits.
The prevalence of polyneuropathy following bariatric surgery is less well-documented, though it is recognised as a potential complication of thiamine deficiency. In this case, the patient developed severe axonal neuropathy with distal predominance, which contributed to her persistent weakness and sensory deficits. The slow and prolonged recovery expected in this patient is consistent with the natural history of axonal neuropathy, which often requires months to years for significant improvement, if at all [6]. This highlights the need for long-term neurological rehabilitation and support for patients who develop such complications.
Conclusions
In conclusion, this case highlights the hidden costs of bariatric surgery, particularly the risk of nutritional deficiencies and their severe neurological consequences. Thiamine deficiency, though preventable, remains a significant concern in post-bariatric surgery patients, with potentially devastating outcomes if not promptly recognised and treated. The prevalence of WE and polyneuropathy following bariatric surgery underscores the need for rigorous nutritional monitoring, proactive supplementation, and comprehensive patient education. By addressing these issues, healthcare providers can improve post-operative outcomes and enhance the quality of life for patients undergoing bariatric surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO). (2021). Obesity and overweight. Retrieved from https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight 3 2025 https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
- 2Benefits and risks of bariatric surgery in adults: A review JAMA Arterburn DE Telem DA Kushner RF Courcoulas AP 8798873242020 https://doi.org/10.1001/jama.2020.125673287030110.1001/jama.2020.12567 · doi ↗ · pubmed ↗
- 3Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss in Patients With Morbid Obesity: The SM-BOSS Randomized Clinical Trial JAMA Peterli R Wölnerhanssen BK Peters T 2552653192018 https://doi.org/10.1001/jama.2017.208972934067910.1001/jama.2017.20897 PMC 5833546 · doi ↗ · pubmed ↗
- 4American Society for Metabolic and Bariatric Surgery integrated health nutritional guidelines for the surgical weight loss Surg Obes Relat Dis Parrott J Frank L Rabena R Craggs-Dino L Isom KA Greiman L 727741132017 https://doi.org/10.1016/j.soard.2016.12.0182839225410.1016/j.soard.2016.12.018 · doi ↗ · pubmed ↗
- 5Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures - 2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic and Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists Obesity Mechanick JI Apovian C Brethauer S 0282020 https://doi.org/10.1002/oby.2271910.1002/oby.22719 · doi ↗ · pubmed ↗
- 6Vitamin status after bariatric surgery: A randomized study of gastric bypass and duodenal switch Am J Clin Nutr Aasheim ET Björkman S Søvik TT 1522902009 https://doi.org/10.3945/ajcn.2009.275831943945610.3945/ajcn.2009.27583 · doi ↗ · pubmed ↗
- 7Wernicke’s encephalopathy: New clinical settings and recent advances in diagnosis and management Lancet: Neurol Sechi G Serra A 442455620071743409910.1016/S 1474-4422(07)70104-7 · doi ↗ · pubmed ↗
- 8Nutritional deficiencies after bariatric surgery Nat Rev Endocrinol Bal BS Finelli FC Shope TR Koch TR 54455682012 https://www.nature.com/articles/nrendo.2012.482252573110.1038/nrendo.2012.48 · doi ↗ · pubmed ↗