Perianal Paget's Disease: A Challenge of Surgical Margins in Uncommon Clinical Presentations
Sarah K Whitehouse, Heng-Chin Chiam

TL;DR
This paper discusses a rare case of perianal Paget's disease that was challenging to surgically treat due to unclear tumor margins.
Contribution
The novelty lies in highlighting the difficulty of achieving clear surgical margins in perianal Paget's disease coexisting with adenocarcinoma.
Findings
Perianal Paget's disease was found alongside invasive adenocarcinoma of the anus.
Wide surgical resection failed to achieve clear margins due to ambiguous tumor borders.
The patient is undergoing topical treatments following surgery.
Abstract
Perianal Paget's disease is a rare entity that often presents with scaly, erythematous plaques. It manifests with an insidious onset, a high frequency of concurrence with malignancy, and difficulties in ensuring clear resection margins. This case highlights the unexpected findings of perianal Paget's disease when completing an excision of invasive adenocarcinoma of the anus. Due to the difficulty with ambiguous borders, wide resection still had involved margins. The patient is currently completing topical treatments.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
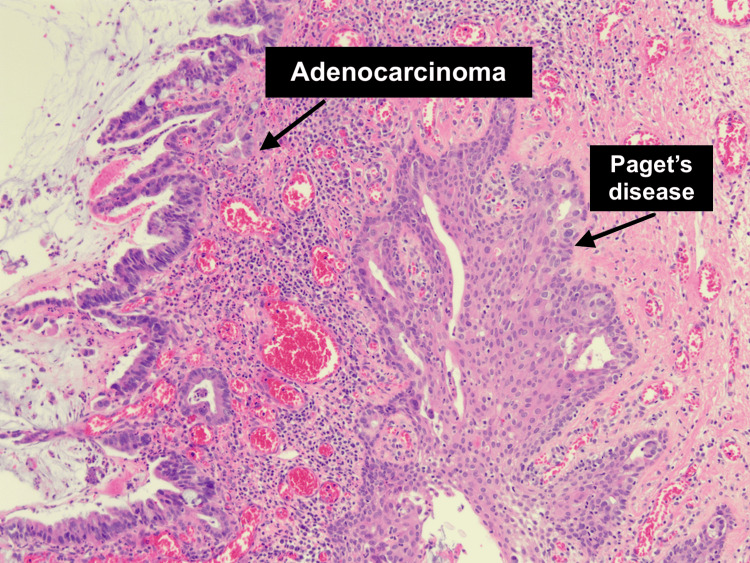 Figure 1
Figure 1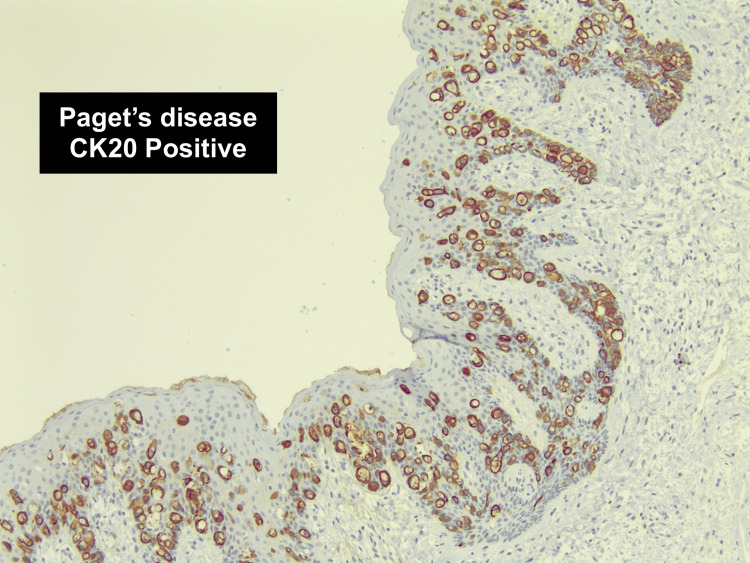 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Nonmelanoma Skin Cancer Studies · Ear and Head Tumors
Introduction
Paget's disease is an uncommon condition presenting as erythematous plaques on apocrine gland-bearing areas of the body [1]. Extramammary Paget's disease was first described in 1889 and is primarily found in vulval and perineal areas [2,3]. Less than 20% of extramammary Paget's disease occurs in the perianal area [2]. It can be clinically insidious, presenting with nonspecific erythematous or leukoplastic plaques [2,4].
The current standard of treatment for perianal Paget's disease is surgical excision of the lesion [2,4-6]. Many cases require a wide local excision, possibly with the requirement of flap reconstruction or diverting colostomy to promote wound healing [5,7]. Some wide excision cases may be complicated by anal stenosis [7,8]. Difficulty confirming margins is the main reason for a 33%-60% reoccurrence rate in the literature [5]. This can also complicate the re-excision of involved margins if flaps have been used, as it confuses the margins. This has led clinicians to use more radical surgical approaches such as abdominoperineal resection or Mohs micrographic surgery [2]. If surgery is contraindicated or margins are involved, alternative therapies such as imiquimod topical treatments, phototherapy, or radiation therapy have been utilized [2,6,8-12].
Case presentation
An 86-year-old female patient presented to the General Surgery Outpatients' clinic to investigate a new anal lump, suspected to be a fibroepithelial polyp, associated with bright red per-rectal bleeding. She had no trauma, pain, pruritus, or discharge associated with this lump. She was a frail lady due to advanced age and several health conditions, including atrial fibrillation (on anticoagulation), chronic obstructive pulmonary disease, latent tuberculosis, and hypothyroidism. She had also been investigated for non-specific dermatological issues in other parts of the body, which were severe enough to warrant consideration of immunosuppressive agents.
She underwent a transanal excision of an anal polyp with intraoperative findings documented as a 3 cm polyp at the anal verge at 6 o'clock with a broad stalk. Large hemorrhoids were also noted at 5 and 7 o'clock. Histology unexpectedly showed adenocarcinoma of the anus with involved margins.
After computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) scans showed no concerns for further invasive or metastatic disease, a multidisciplinary team (MDT) meeting recommended a further local resection of the tumor.
She underwent a further excision of this lesion, which was completed by a senior surgeon. Intraoperative findings showed no macroscopic lesion or recurrence of the malignant polyp. Hemorrhoids were present at 3, 11, and 7 o'clock, with the latter looking slightly irregular and in continuity with a warty-appearing skin tag. The final excision was from 5 o'clock to 8 o'clock, including both this area and the previous scar. Histology showed a completely excised invasive adenocarcinoma; however, it surprisingly revealed perianal Paget's disease involving the right lateral, left lateral, and distal margins (Figures 1, 2).
Histology (hematoxylin and eosin stain) slide showing areas of both adenocarcinoma and perianal Paget's disease
Histology slide (using cytokeratin 20 stain) showing perianal Paget's disease
After re-discussion at MDT, the patient underwent a repeat wide local excision of the previous excision site. Intraoperative findings note a perianal skin lesion at 4 o'clock, 10-15 mm from the anal verge. There were also ill-defined perianal skin changes at 6 o'clock, 10 mm from the anal verge (Figure 3).
Intraoperative images of the findings of perianal Paget's disease
An attempt was made to excise this entire area with generous margins. The excision involved 4-9 o'clock areas from 25 mm proximal to the verge to 20 mm radial to the skin. Unfortunately, histology still showed an R1 resection, positive for Paget's disease.
One month postoperatively, she was reviewed in general surgery clinics with an almost healed anal wound and no significant stenosis. Due to the ongoing involvement of margins in a preoperatively frail lady, a decision was made to abandon further attempts at excision and consider topical or photodynamic therapies. Radiation was declined by the patient due to expected side effects.
Discussion
Perianal Paget’s disease can be a surprise diagnosis, specifically due to its nonspecific and wide-ranging appearance. The link between perianal Paget's and anal or colorectal malignancy is well established but poorly understood due to the rarity of the condition and, thus, difficulty with enough data to analyze [8]. It adds to the body of evidence that would recommend wide-ranging investigation and exclusion of distant malignancies when a diagnosis of Paget's disease is made.
Even large centers, such as the Mayo Clinic or multiple centers, require very long study periods to get small data sets that are unable to guide treatment regimens with great authority [4,5]. Systematic reviews slowly achieve numbers for evidence-based guidelines [9-11].
Due to its association with cancer, targeted cancer screening should be undertaken, depending on its subtype [9,10].
This case, similar to others documented, shows the challenges associated with achieving adequate margin control in this condition. This difficulty and its tendency to occur in older patients leave a question not uncommon to many surgeons: how extensive an operation is too extensive for this patient? Due to our patient's overall frailty, a radical resection with colostomy would likely pose significant risks, both from prolonged anesthetic time and complications related to wound healing and colostomy management. Therefore, with increased risks of anal stenosis, a fourth operation was not undertaken, but management moved to field control.
Further consideration of localized or free flaps could be considered to allow for further wide local excisions. However, the challenge lies in identifying the original border of the excision when positive margins require re-excision. Radiation therapy has been successfully utilized in other cases [12]. Photodynamic therapy and topical immunotherapy have also been used in some cases.
Conclusions
In summary, this case involves an elderly and comorbid female patient who had a surprise finding of anal adenocarcinoma and Paget's disease of the anus when investigating bright red per-rectal bleeding. She underwent multiple local excisional surgeries to gain local control of the condition. Unfortunately, this was not achieved, and she is undergoing further adjuvant therapy for the area.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1On disease of mammary areola preceding cancer of mammary gland St Barts Hospital Rep Paget J 8789101874
- 2Extramammary Paget disease Dermatol Online J St Claire K Hoover A Ashack K Khachemoune A 130301303715201931046904 · pubmed ↗
- 3Paget’s disease affecting the scrotum and penis Transactions of the Pathological Society of London Crocker H 187191401888 https://wellcomecollection.org/works/texw 46xg
- 4Perianal Paget's disease: a clinicopathological and immunohistochemical study of 13 cases Diagn Pathol Liao X Liu X Fan X Lai J Zhang D 291520203220911910.1186/s 13000-020-00952-w PMC 7093992 · doi ↗ · pubmed ↗
- 5Perianal Paget's disease: presentation of six cases and literature review Int J Colorectal Dis Minicozzi A Borzellino G Momo R Steccanella F Pitoni F de Manzoni G 172520101970777410.1007/s 00384-009-0797-9 · doi ↗ · pubmed ↗
- 6Extramammary Paget's disease of the perianal region: a review of the literature emphasizing management Dermatol Surg Mengjun B Zheng-Qiang W Tasleem MM 69753920132312718110.1111/dsu.12019 · doi ↗ · pubmed ↗
- 7Perianal Paget's disease: one century later and still a challenge BMJ Case Rep Guidi GJ Pinto de Sousa J Marques R Ferreira C 14202110.1136/bcr-2020-240435 PMC 786827533541959 · doi ↗ · pubmed ↗
- 8Perianal Paget's—an aggressive disease Colorectal Dis Rudnicki Y Stapleton SM Batra R Gan T Mathis KL Kelley SR 121312212520233694512510.1111/codi.16549 · doi ↗ · pubmed ↗