Heterotopic pancreatic tissue presenting as an unusual cause of gastric outlet obstruction in infancy: a case report
Ahmed Oshiba, Karim Darweesh, Hend Sharafeldin, Mostafa Kotb

TL;DR
A 2-month-old girl had repeated vomiting due to a rare condition where pancreatic tissue blocked her stomach's outlet, requiring surgery for removal.
Contribution
This case report highlights heterotopic pancreatic tissue as a rare cause of gastric outlet obstruction in infants.
Findings
A 2-month-old girl had gastric outlet obstruction caused by ectopic pancreatic tissue.
Surgical removal of the mass resolved the obstruction, confirmed by pathological analysis.
Histology is essential for definitive diagnosis despite initial imaging results.
Abstract
Gastric outlet obstruction beyond the neonatal period is an extremely rare condition when other causes such as infantile hypertrophic pyloric stenosis, pyloric atresia, and antral diaphragm are ruled out. Herein, we present the case of a 2-month-old girl who presented with repeated nonbilious vomiting and showed ectopic pancreatic tissue compressing the pylorus of the stomach. A 2-month-old Caucasian girl who suffered from frequent attacks of projectile vomiting that was not resolved by medication presented to our institute. On ultrasonography, pyloric stenosis was excluded, while on gastrograffin study, there was a hugely dilated stomach with delayed passage of contrast to the distal bowel. On surgical exploration, there was an exophytic pyloric mass compressing the pyloric canal, which was completely excised. Pathological results confirmed the presence of heterotopic pancreatic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
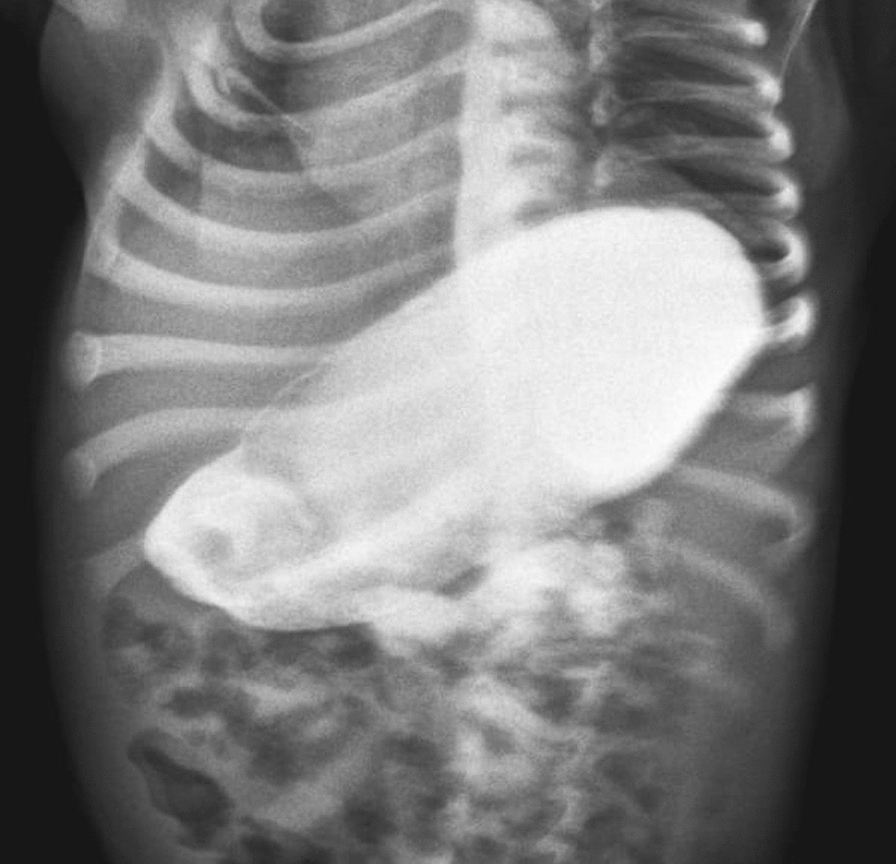 Figure 1
Figure 1 Figure 2
Figure 2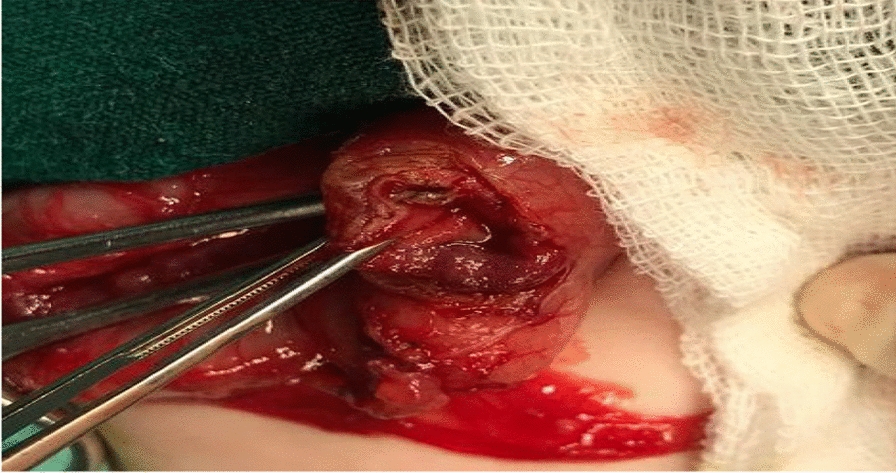 Figure 3
Figure 3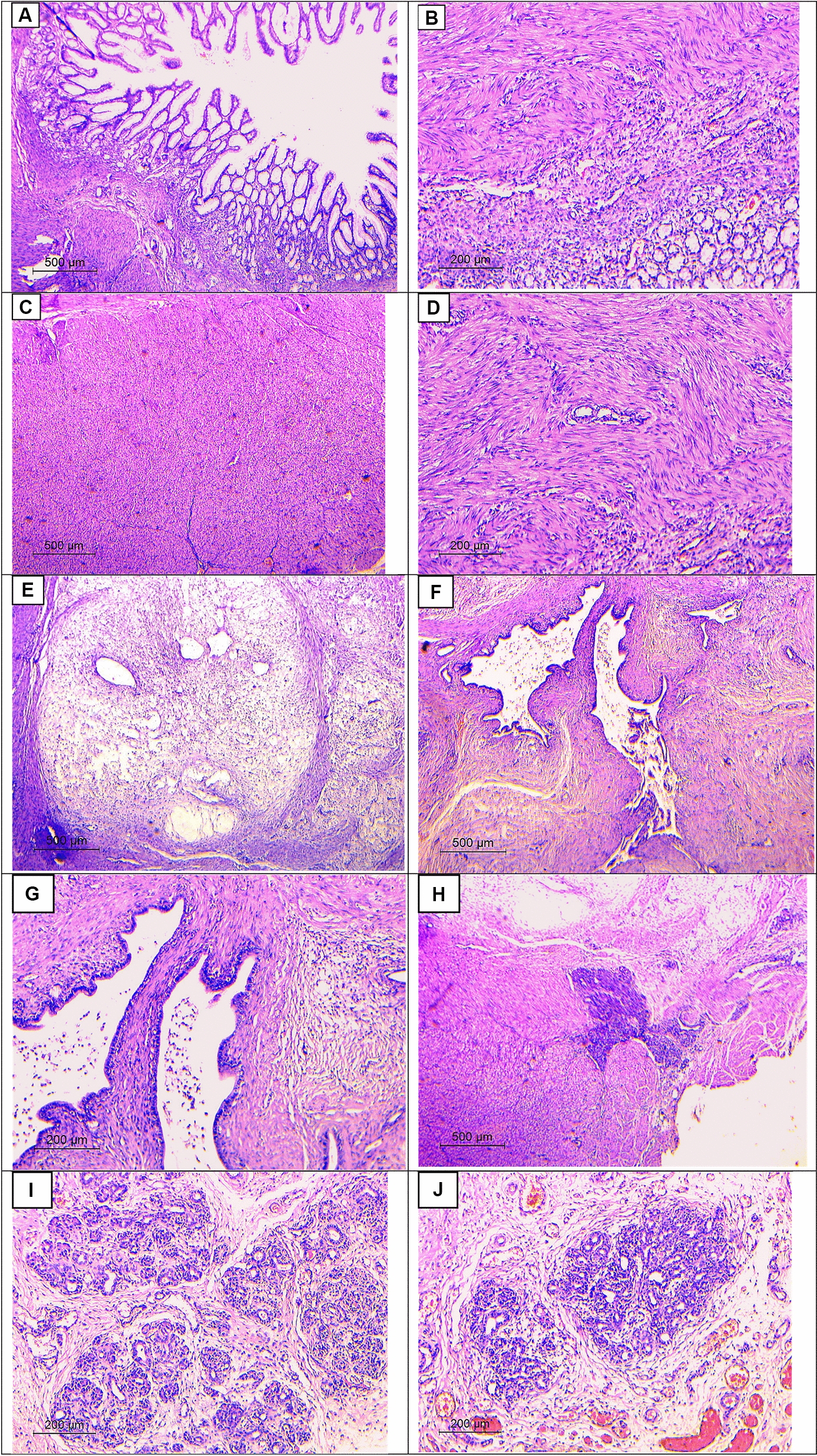 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Intestinal Malrotation and Obstruction Disorders · Pediatric Hepatobiliary Diseases and Treatments
Introduction
Gastric outlet obstruction (GOO) in infancy and childhood may result from congenital causes, for example, antral diaphragm, pyloric atresia, ectopic pancreatic tissue and infantile hypertrophic pyloric stenosis (IHPS), or acquired causes (peptic ulcer, caustic ingestion, tumor, and chronic granulomatous disease) [1]. With an incidence of up to 1–3.5:1000 per live birth, IHPS is the most frequent cause among them [2]. Whenever IHPS is excluded, the incidence of the latter causes was only 1 in 100,000 live births [3]. IHPS can be diagnosed easily and responds well to Ramstedt’s pyloromyotomy. Other causes of gastric outlet obstruction such as pyloric atresia, prepyloric webs, and diaphragm can be managed by excision of membrane and pyloroplasty. A pyloric mass compressing the pylorus is very rare in infants, but it ought to be considered after ruling out IHPS.
“Ectopic pancreas” is the term used to describe pancreatic tissue located in an organ or tissue that is not anatomically or vascularly connected to the normal pancreas. This condition is also called aberrant pancreas, heterotopic pancreas, or pancreatic rest. The exact mechanism remains controversial, but it has been theorized that it most likely arises congenitally during embryonic development [4, 5].
Case report
A 2-month-old Caucasian girl weighing 2.7 kg presented to our institute with continuous projectile nonbilious vomiting for 3 weeks. The frequency of vomiting had gradually increased in the last week. Although the infant was receiving antiemetics, the frequency of vomiting was uncontrollably high, with significant weight loss. Generally, the child was lethargic and severely dehydrated. Abdominal examination revealed fullness in epigastrium with visible peristalsis. Laboratory investigation showed anemia with hypokalemic hyponatremic metabolic alkalosis. Blood urea and serum creatinine were within normal limits. Abdominal sonography showed abnormal thickening in the pyloric canal and gastric dilatation; however, pyloric stenosis could not be excluded. The upper GI contrast study showed a dilated double loop of stomach with significant constriction at prepyloric region and delayed gastric emptying (Fig. 1).Fig. 1. Contrast study showing hugely dilated stomach, prepyloric stricture, and delayed gastric emptying
The diagnosis of gastric outlet obstruction was confirmed, and the baby was planned for elective laparotomy. Preoperatively, the child was managed with nasogastric aspiration, intravenous fluid, and antibiotics till serum electrolyte correction. On exploration, the stomach was distended with exophytic mass compressing the prepyloric region arising from the external wall (Fig. 2). Longitudinal incision was performed around the mass along the line of pylorus. The mass was firm in consistency, arising from the external wall of the pylorus, and was completely excised. The pylorus was transversally closed (Fig. 3). Patency was checked by passing normal saline through the segment. The postoperative period was uneventful, and the patient started oral feeding on the third day. The pathology of the excised specimen was heterotopic pancreatic tissue causing compression of the pyloric area (Fig. 4).Fig. 2. Exophytic pyloric mass, yellowish in color, compressing the pylorusFig. 3Opened pylorus after complete excision of the mass, closed transverselyFig. 4Histopathological examination: (A) unremarkable gastric mucosa (hematoxylin and eosin, 40×), B) unremarkable gastric mucosa with underlying thickened bundles of muscularis propria (hematoxylin and eosin, 100×), C, D) thickened bundles of muscularis propria (hematoxylin and eosin, 40× and 100×, respectively), E) areas of edema and mild inflammatory infiltrate (hematoxylin and eosin, 40×), F, G) pancreatic ducts (hematoxylin and eosin, 40× and 100×, respectively), and H, I, J) pancreatic acini (hematoxylin and eosin, 40×, 100×, and 100×, respectively)
Discussion
Gastric outlet obstruction (GOO) in infancy is a relatively rare condition with incidence of 1 in 100,000 live births when IHPS is excluded [1, 3]. The incidence of IHPS is 1.5–3 per 1,000 live births [3]. However, conditions such as gastric web, pyloric atresia, ectopic pancreatic tissue, and duplication of pylorus can also produce the sign symptoms of GOO. The acquired causes of GOO in infants are acid peptic disease, neoplasm, and caustic ingestion, and they are relatively uncommon [2, 6].
There is scant information on the incidence of ectopic pancreas in infancy as a cause of gastric outlet obstruction. In our case, it presented at age of 2 months; however, the lesion is found in 0.2% (1 in 500 surgeries) of abdominal surgeries in adult population, and in a large autopsy studies, the frequency of ectopic pancreas ranged from 0.6% to 13.7%, being commonly seen at 30–50 years of age with male preponderance [7, 8].
Ectopic pancreas is mostly found in the stomach (as in our patient), duodenum, and jejunum; nevertheless, it may also be found anywhere in the digestive tract, intraabdominally, or in the mediastinum or lungs [9]. Involvement of the stomach is seen in 25–40% of cases, most frequently being located along the greater curvature of the gastric antrum [10, 11]. In our case, this abnormal tissue was located in the pyloric region. In the stomach, the submucosal layer is the most common location of the pancreatic rest [12]. Preoperative diagnosis of ectopic pancreas is uncommon, and it usually occurs as an incidental finding [13]. Presentation may, however, be symptomatic in the form of weight loss, epigastric pain (the most common presentation), and vomiting resulting from mechanical gastric outlet obstruction [14]. In our case, the child presented with progressive projectile vomiting and failure to thrive.
Adult patients may also develop complications such as pancreatitis, pseudocyst, insulinoma, and pancreatic carcinoma [8]. The incidence of malignant transformation in ectopic pancreas was reported by Nakao et al. to be as high as 12.7% [15]. Clinically, ectopic pancreas is typically difficult to distinguish from leiomyomas, adenomatous polyps, gastrointestinal stromal tumor (GIST), and even peptic ulcer disease [16]. Endoscopy, sonogram, and computed tomogram may be helpful in diagnosis, but only histology is definitive to differentiate ectopic pancreas from other lesions [17]. In the asymptomatic patient, periodic monitoring is recommended. Patients with symptoms do not respond well to medical treatment; in these cases, localized surgical excision has been demonstrated to be a safe and sufficient procedure, unless malignant transformation has taken place [18, 19]. Prognosis following excision is excellent.
Conclusion
Ectopic pancreas should always be considered as one of the rare differentials of the causes of gastric outlet obstruction in infants. Although many investigations such as sonogram and upper GI series help in diagnosis, histology remains the definitive test in reaching the final diagnosis.