Relationship between dental erosion and asthma medication in children: a systematic review
André Alexis Díaz Quevedo, Diana Guadalupe Anaya Rubina, Carol Magaly Cárdenas Flores

TL;DR
This study reviews the relationship between asthma medications and dental erosion in children, finding no clear link.
Contribution
The study provides a systematic review clarifying the ambiguous association between asthma medication and dental erosion in children.
Findings
Some studies show higher dental erosion in children using asthma medications.
Other studies report higher erosion in healthy children compared to those with asthma.
Asthma medications are not a determining factor for dental erosion in children.
Abstract
Dental erosion is an alteration that affects the integrity of teeth, which has several aetiologies. It is mentioned that asthma medications may be an etiologic factor; however, studies fail to clarify the possible association between these variables in children with asthma. Therefore, the purpose of this study will be to determine the relationship between dental erosion and asthma medication consumption in paediatric patients. A systematic research was performed in databases such as MEDLINE (PubMed), Scopus, Web of Science, Scielo, Cochrane Library, Embase, LILACS and gray literature (Open Gray). Two researchers independently selected the articles according to the population, exposure, outcome, study design (PEOS) question using the Rayyan program. Newcastle-Ottawa scale was used to assess the risk of bias. Six articles were included from 120 selected articles. The studies by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
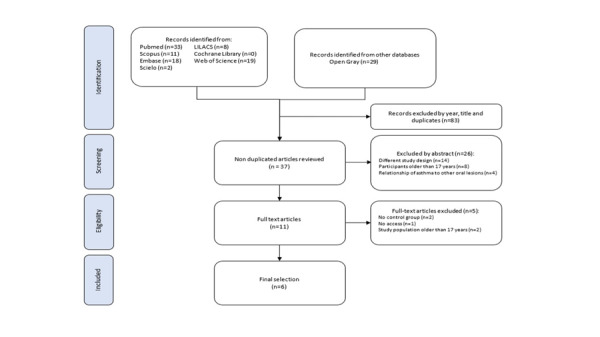 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Erosion and Treatment · Dental Anxiety and Anesthesia Techniques · Scientific and Engineering Research Topics
INTRODUCTION
Teeth are prone to structural changes due to the influence of the oral environment, in which a chemical wear process called dental erosion can develop with a group of specific factors. ^(^1^,^2 This tooth wear is caused by an interaction of the oral cavity with extrinsic or intrinsic acids. 1^-^4 The so-called acids can come from the diet, from the person's own gastric juices, or even certain medications used to treat diseases such as asthma. 4^-^6 Asthma is a chronic systemic condition characterized by airway obstruction due to an allergic or hypersensitivity reaction, which affects a considerable number of people worldwide. ^(^7^-^9 According to the International Study of Asthma and Allergies in Childhood, asthma is the most prevalent chronic condition in children overall. ^(^10 Although it is true that this pathology has no cure, however, asthma episodes can be controlled with inhalers such as bronchodilators (salbutamol) or steroids (beclomethasone). ^(^11^-^13 The frequency of use of these inhalers will depend greatly on exposure to the agents that cause asthmatic episodes and symptoms of the disease. 7^,^11
One study showed that the incidence of tooth erosion was higher in child patients suffering from asthma. 14 These results are consistent with other authors who evaluated the prevalence of this dental wear in children and adults with asthma problems. ^(^15^,^16 Furthermore, the asthma medications most associated with dental erosions were salbutamol, corticosteroids, or a combination of both in their inhaler presentation. 6^,^16^,^17 However, other studies did not find a significant relationship between the variables, mentioning that not all asthma medications are potentially erosive. ^(^17^-^19
There are studies in which they have investigated the relationship between dental erosion and the consumption of asthma medications in children, obtaining results that show that there is a relationship between these variables20^-^24, while others present the opposite. ^(^17^,^18^,^25 Therefore, the purpose of this study will be to determine the relationship between dental erosion and the consumption of asthma medications in paediatric patients, through a systematic review of published articles.
MATERIALS AND METHODS
Protocol and registration
This systematic review was registered in PROSPERO with the ID number CRD42021254243 and is under the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA). 26^)^
Selection criteria
The review mainly included observational studies of case-control and cohort studies, published from 2000 to 2024. The study population should be in the age range of 3 to 17 years. Similarly, articles that mention the consumption of asthma drugs were included.
Those articles that had as their study population patients with systemic disease other than asthma, patients with asthma and other associated comorbidity, studies that associate dental erosion with other factors such as eating disorders, or the consumption of acidic foods were excluded. Furthermore, studies with descriptive study design, studies with missing findings, and articles with a dubious methodological section were excluded.
Search strategies
A comprehensive bibliographic search strategy was carried out in the different databases such as MEDLINE (PubMed), Scopus, Web of Science, Scielo, Cochrane Library, Embase, LILACS and gray literature (Open Gray).
The search strategy was limited to paediatric patients from January 2000 to May 2024, with no language restriction. In addition, several search terms related to the population, exposure, outcome, study design (PEOS) question were used in conjunction with MeSH terms and Boolean operators (AND, OR). Keywords such as "dental erosion", "tooth erosion", "asthma", "children" were used. The consolidated search was as follows: ("tooth erosion"[MeSH terms] OR "tooth erosion"[Title/Abstract] OR "dental erosion"[MeSH terms] OR "dental erosion"[Title/Abstract] OR "children"[MeSH terms] or "children"[Title/Abstract] or "asthma"[MeSH terms] or "asthma"[Title/Abstract]). Thus, a manual search was carried out systematically. This search strategy was adapted in the different databases.
Study selection
All selected articles were exported to the EndNote X9 program for the evaluation of each content of the published articles. Thereupon, the information was exported to the Rayyan program for the selection and exhaustive review of the articles found in the different databases.
In the first stage, two reviewers (AADQ, DGAR) independently eliminated the duplicated articles using the Rayyan program, then carried out the selection of articles according to the title. Those articles that included the words that are related to the variables of the systematic review were selected.
In the second stage, both review authors independently analysed the abstracts of those selected articles to choose the appropriate studies for the third stage.
In the third stage, both reviewers downloaded the articles in full text for examination and subsequent selection, considering the established inclusion and exclusion criteria (Fig. 1). During the process of selecting the articles, there was disagreement between the two reviewers, so the presence of a third reviewer was necessary. In addition, information was requested via email from an author to purchase the full-text article.
Fig.1PRISMA flow diagram detailing the study selection
Standardization process
With all the information from the Rayyan program, the criteria were standardized and the agreement observed among the evaluators was evaluated using the Kappa test. The concordance found between the two evaluators (AADQ, DGAR) was greater than 0,80.
Data extraction
Data extraction was performed by the 2 review authors (AADQ, DGAR). In this regard, with the help of the Microsoft Excel program, a table was created that allows the compilation of the data of the selected articles: Author/year of publication (1); title (2); objective (3); type of study (4); population (age and number of patients): deciduous dentition (5), mixed dentition (6), permanent dentition (7); Methodology: type of drug (8), time of consumption of the drug (9), consumption of sugars (10); Results: Dental erosion (11) and conclusions (12). The accuracy of data collection was confirmed by a third reviewer who was responsible for resolving discrepancies.
Data analysis and assessment
The information obtained was described in an orderly manner to develop evaluation tables and better observe the homogeneity of the information obtained from the selected articles. The data found were not homogeneous because the studies used different diagnostic methods for dental erosion, were done in different countries, and not all studies detail the measures of association and the types of asthma medications they used. Therefore, meta-analysis was not performed.
Risk of bias
The risk of bias assessment of the selected observational studies was carried out by two review authors using the Newcastle-Ottawa scale (NOS) where each case-control and cohort study was assessed based on three domains: 1) Study group selection; 2) comparability of groups and 3) determination of exposure. ^(^27 According to the evaluation, each study will obtain a maximum score of 9 points. If the study score is seven to nine, the risk level will be low. A rating less than or equal to six will be high risk. 27
RESULTS
Study selection
A total of 120 articles were identified; after removing duplicates and some articles because they were outside the established search period and based on the title, 37 articles remained. The title and abstract of each article were independently assessed by the two reviewers. A further 26 articles were excluded because they did not meet the inclusion criteria. Five articles 28^-^32 were excluded due to missing findings, restricted access, and not considering a control group within the evaluation. A third author was requested to resolve discrepancies between the two reviewers regarding study selection. Finally, 6 articles met the inclusion criteria and were included for qualitative assessment (Figure 1).
Included studies characteristics
Of the total number of articles found, 5 6^,^17^-^19^,^22 were cohort studies and 120 was a case-control study. Regarding the sociodemographic context, Alazmah and Arafa et al. ^(^18^, 22)^ conducted the study in Saudi Arabia, while the studies by Bairappan et al., Dugmore and Rock, Rezende et al., and Domenzain et al. ^(^6^,^17^,^19^,^20 were conducted in India, England, Brazil, and Mexico, respectively. In relation to the age of the population, the studies by Dugmore and Rock, Alazmah, Rezende et al., Domenzain et al., and Arafa et al. 17-20, 22 evaluated similar populations in terms of age (3-12 years) and only the study by Bairappan et al. 6 evaluated adolescents aged 12 to 15 years. The study by Dugmore and Rock17 evaluated a more representative sample of 1753 participants, as opposed to the other studies6^,^18^-^20^,^22 which had 100, 180 or 228 participants. All studies6^,^17^-^20^,^22 have the characteristic of excluding patients with an associated comorbidity or if they had any other systemic condition other than asthma. The studies by Alazmah and Arafa et al. ^(^18^,^22 used the Smith and Knight Dental Wear Index as a diagnostic method, while Bairappan et al. ^(^6 used the dental erosion index from World Health Organization (WHO) oral health assessment form for children of the year 2013; Dugmore and Rock, and Rezende et al. ^(^17^,^19, the 1993 Children's Dental Health Survey Index in the United Kingdom; Domenzain et al. ^(^20, the Basic Erosive Wear Examination (BEWE) index. The studies by Bairappan et al., Dugmore and Rock, and Domenzain et al. ^(^6^,^17^,^20 were the only ones to evaluate the type of medication used by asthmatic patients, of which bronchodilators, corticosteroids and/or a combination of both stand out. The studies by Dugmore and Rock, and Domenzain et al ^ . ( ^17^,^20 refer to the surfaces most affected by dental erosion, of which Dugmore and Rock 17 highlight the palatal surfaces of the upper teeth and the buccal surface of the lower teeth, while Domenzain et al. ^(^20 mention the palatal surfaces of the anterosuperior teeth and the occlusal surface of the lower teeth (Table 1).
Table 1. Data extraction table.AuthorYearCountryStudy designPopulation ageInclusion and exclusion criteriaSample sizeDiagnostic methodsMention of medicationsMost affected tooth surfacesAbdulfatah Alazmah18 2021Saudi ArabiaCohort3-12 yearsInclude children under the age of 12 with parental consent and without other systemic disease100Smith and Knight Tooth Wear Index------------Dugmore and Rock17 2003EnglandCohort12 yearsInclude 12-year-olds from all state-maintained schools in Leicestershire and Rutland, selected based on the inclusion of one in five children in the respective school register1753Index from the 1993 UK Children´s Dental Health SurveyCorticosteroid Bronchodilators CromolynPalatal surfaces of the upper teeth Buccal surface of the lower teethDomenzain et al. ^(^20 2021MexicoCases controls5-12 yearsExclude children with systemic disease other than asthma228BEWE Index (Basic Erosive Wear Examination)-----Palatal surfaces of the anterosuperior teeth Occlusal surface of the lower teethRezende et al. ^(^19 2019BrazilCohort6-12 yearsInclude asthmatic children (registered in health units) and non-asthmatic children (registered with the Asthma program in health units)228Index from the 1993 UK Children´s Dental Health SurveyBronchodilator Bronchodilator + Corticosteroid or Glucocorticoid + Systemic corticoids-----Bairappan et al. ^(^6 2020IndiaCohort12-15 yearsAsthmatic patients with another associated systemic disease and with medication other tan asthma are excluded100Tooth Wear Index (WHO 2013 oral health assessment form for children)Bronchodilators Corticosteroids Bronchodilators + Corticosteroids Antihistamines + Bronchodilators Antihistamines + Bronchodilators + Corticosteroids-----Arafa et al. ^(^22 2017Saudi ArabiaCohort4-12 yearsExclude children with serious diseases or other chronic systemic conditions other than asthma180Smith and Knight Tooth Wear Index-----------UK, United Kingdom; WHO, World Health Organization
Risk of bias assessment
Overall, of the total number of studies analysed, three were at high risk(6^,^20^,^22 and three were at low risk of bias. ^(^17^-^19 Bairappan et al., Dugmore and Rock, and Arafa et al. ^(^6^,^17^,^22 did not meet the criterion of representativeness of the exposed cohort. Only Dugmore and Rock´s study17^)^ met the criterion related to sufficiently long follow-up (2 years) for results. Regarding the study by Domenzain et al. ^(^20, it did not meet the adequate case definition and control selection (Table 2 and 3).
Table 2. Risk of bias assessment for cohort studies.Study Selection Comparability Outcome NOS ScoreRepresentativeness of the exposed cohortSelection of the non-exposed cohortAssessment of exposureDemonstration that outcome of interest was not present at start of studyComparability of cohorts on the basis of the design or analysisAssessment of outcomeWas follow-up long enough for outcomes to occurAdequacy of follow up of cohorts Dugmore and Rock17
*******7Rezende et al. ^(^19
*7Arafa et al. ^(^22
*6Abdulfatah Alazmah18
*7Bairappan et al. ^(^6
*6NOS, Newcastle-Ottawa Scale
Table 3. Risk of bias assessment for case control studies.StudySelection Comparability Outcome NOS Score¿Is the case definition adequate?Representativeness of the casesSelection of controlsDefinition of controlsComparability of cases and control son the basis of the design or analysisAssessment of exposureSame method of ascertainment of exposureNon-response rate Domenzain et al. ^(^20
*****6NOS, Newcastle-Ottawa Scale
Relationship between medication exposure and presence of dental erosion
Of the total number of articles selected, the higher prevalence of dental erosion in asthmatic children compared to children without asthma was highlighted in the studies by Bairappan et al., Alazmah, Domenzain et al. and Arafa et al. ^(^6^,^18^,^20^,^22 with a total of 44%, (p<0.05), 24% (p>0.05), 36.8% (p<0.05, OR=2.018 (1.05 - 3.85)) and 40% (p<0.05) respectively. However, the study by Alazmah18 concluded that there is no correlation between asthma and the presence of dental erosion, unlike the studies by Bairappan et al., Domenzain et al. and Arafa et al. ^(^6^,^20^,^22 which concluded that there was a significant association between asthma and the presence of dental erosion. On the other hand, the studies by Dugmore and Rock, and Rezende et al. ^(^17^,^19 showed the highest prevalence of dental erosion in children without asthma, with an estimated 58.9% (p>0.05, OR=1.05) and 32.14% (p>0.05) respectively (Table 4).
Table 4. Association between medication exposure and dental erosion or outcome.AuthorSample sizeNº of children with asthmaNº of children without asthmaOutcome Dental erosion prevalence percentage (%) p valueMeasure of associationGeneral conclusionCACWACACWA
Abdulfatah Alazmah18 10050501292418> 0.05-There is no correlation between asthma and the presence of tooth erosion.Dugmore and Rock17 1753268133115879458.959.70.89OR=1.05There is no association between asthma and the presence of dental erosion. Medications are not potentially erosiveDomenzain et al. ^(^20 22876152283436.822.40.02OR=2.018 (1.05-3.85)Significant association between asthma and the presence of dental erosionRezende et al. ^(199^228112116364432.1437.90.36-There is no association between the presence or absence of tooth erosion and the types of asthma medicationBairappan et al. ^(^6 100505022944180.043-Significant association between asthma and the presence of dental erosionArafa et al. ^(^22 180120604884013.3≤0.001-Significant association between asthma and the presence of dental erosionCA, children with asthma; CWA, children without asthma; OR, odds ratio
DISCUSSION
The present systematic review evaluated the association between asthma medication and the presence of dental erosion in asthmatic children aged 3 to 17 years in articles published in the databases. Three studies supported the association of drug use and the presence of tooth erosion in children with asthma. ^(^6^,^20^,^22 Of the three articles in favor, two studies follow a cohort design6^,^22 and one case-control design. 20 The overall sample size of the studies evaluated is very heterogeneous. In the study by Dugmore and Rock17 the sample size was 1753; while in the studies by Bairappan et al. ^(^6 and Alazmah ^(^18 the sample size was 100 children. The observed differences in sample size mean that the association between the variables is not consistent. Likewise, the distribution of children with asthma and healthy children was not homogeneous, unlike the studies by Bairappan et al. ^(^6 and Alazmah18 who considered an equitable distribution of the population. Despite having an equitable distribution, the study by Bairappan et al. ^(^6 found a significant association between drug consumption and the presence of erosive lesions, while Alazmah's study18 found no association between the variables.
One of the reasons for the inconsistency of the association between the variables studied is that most of the studies6^,^17^,^18^,^20 used different diagnostic methods for dental erosion except for the studies by Arafa et al. ^(^18 and Alazmah 22 who used the same diagnostic index of Smith and Knight. In addition, the studies by Dugmore and Rock, and Rezende et al. ^(^17^,^19 agreed on the use of the index from the 1993 Children's Dental Health Survey in the United Kingdom. The difference is that the Smith and Knight index provides a score from 0 to 4 on the 4 surfaces of all teeth, while the BEWE index rates each tooth with a score from 0 to 3 based on the highest score of each sextant and then adds them together to obtain a final score that indicates the severity of tooth erosion. ^(^33^,^34 The index of the 1993 Children's Dental Health Survey in the United Kingdom is similar to the dental erosion index from WHO oral health assessment form for children of the year 2013, because they assess tooth erosion according to the depth of the lesion, whether it encompasses enamel, dentin or pulp. ^(^6^,^17^)^ However, they differ in that the first index from 1993 compiles the area of the tooth affected by erosion. ^(^17 In this sense, these tools are a source of heterogeneity between studies. Although the studies by Alazmah and Arafa et al. ^(^18^,^22 were conducted in the same country, they differ in relation to the association of the variables studied. The study by Arafa et al. ^(^22 found a significant association between asthma medication consumption and the development of dental erosion, while Alazmah's study18 found no association. Another difference found in the analysis is that some of the studies18^,^20^,^22 do not specify the type of medication used in the patients, as well as the time of application. However, they report that asthma medication has a reducing effect on pH and salivary flow, which suggests that it is a factor for the development of alterations in tooth structure such as dental erosion. ^(^6^,^17^,^22^,^35^,^36 In relation to the dental surfaces most affected by dental erosion, the literature shows a higher incidence at the level of the palatal surfaces of the upper incisors and the occlusal surfaces of the lower molars. ^(^1^,^37 In the review, only the studies by Dugmore and Rock, and Domenzain et al. ^(^17^,^20 observed that the palatal and occlusal surfaces were the most affected.
The erosive effect of asthma control medications has been evaluated by several studies. ^(^5^,^38 The pH of these drugs is less than 5,5, and they chemically dissolve tooth enamel if daily administration is frequent. ^(^39 If the medication is administered on a long-term basis, it is associated with a greater possibility of developing alterations at the level of the dental structure, such as dental erosion. ^(^38 However, in the available evidence, not all studies had much information about the medications, such as the time of exposure and the doses administered. Therefore, it is recommended in future research to detail more information about asthma medication to determine its influence.
Dental erosion is influenced by many factors, and asthma medication can contribute to its onset, especially in children who are the most susceptible population to asthma.40^)^ It is therefore important to carry out adequate follow-up in these patients, both in general and oral health. The initial anamnesis will help us determine if the presence of dental erosion is caused by factors such as the consumption of asthma medications, diet, the patient's hygiene or another associated factor.41 It is also suggested to rinse with water after taking asthma medication to control pH levels.39
Limitations
Due to the observational nature of the studies, there is a high risk of bias, which means that the results should be interpreted cautiously, as they do not allow for conclusions about causality. Studies that found a significant association between the variables are particularly vulnerable to bias. In contrast, authors who oppose the association tend to have a lower risk of bias, suggesting that this discrepancy could indicate a reason to question the association between the variables in light of potential biases. Moreover, the studies assessed confounding factors such as brushing frequency 18^,^19, salivary characteristics 6^,^22, and parental education level. ^(^18^,^19 Only two studies did not specify whether confounding factors were considered. ^(^17^,^20 These factors can significantly influence the outcomes, aligning with a systematic review that indicates the intervention group cannot be directly compared to the control group at baseline. ^(^42 Additionally, the studies could not be included in a meta-analysis due to heterogeneity from various issues, such as the lack of standardization in the diagnostic criteria for dental erosion, the studies conducted in different countries, the absence of association measures, and insufficient information regarding asthma medications. This variability suggests that the findings concerning the possible relationship between dental erosion and asthma medication are compromised, representing a limitation in drawing any accurate conclusions.
CONCLUSION
The consumption of asthma medications is not a determining factor for the occurrence of dental erosive lesions in paediatric patients with this systemic condition. Both variables do not present a significant association due to the heterogeneity of the studies. Although the consumption of these medications influences the appearance of erosive lesions, there are other factors that play an important role in this oral condition. Therefore, future research is required to provide more information to clarify the relationship asthma medication has with tooth erosion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Donovan T Nguyen-Ngoc C Abd Alraheam I Irusa K Contemporary diagnosis and management of dental erosion J Esthet Restor Dent 2021331788710.1111/jerd.1270633410255 · doi ↗ · pubmed ↗
- 2Passos VF Melo MAS Park J Strassler HE Current Concepts and Best Evidence on Strategies to Prevent Dental Erosion Compend Contin Educ Dent 2019402808630767547 · pubmed ↗
- 3Chan AS Tran TTK Hsu YH Liu SYS Kroon J A systematic review of dietary acids and habits on dental erosion in adolescents Int J Paediatr Dent 202030671373310.1111/ipd.1264332246790 · doi ↗ · pubmed ↗
- 4Marques Martínez L Leyda Menéndez AM Ribelles Llop M Segarra Ortells C Aiuto R Garcovich D Dental erosion Etiologic factors in a sample of Valencian children and adolescents. Cross-sectional study Eur J Paediatr Dent 201920318919310.23804/ejpd.2019.20.03.0431489816 · doi ↗ · pubmed ↗
- 5Scatena C de Mesquita-Guimarães KSF Galafassi D Palma-Dibb RG Borsatto MC Serra MC Effects of a potentially erosive antiasthmatic medicine on the enamel and dentin of primary teeth An in situ study Microsc Res Tech 20188191077108310.1002/jemt.2307430351522 · doi ↗ · pubmed ↗
- 6Bairappan S Puranik MP RSK Impact of asthma and its medication on salivary characteristics and oral health in adolescents A cross-sectional comparative study Spec Care Dentist 202040322723710.1111/scd.1246232357265 · doi ↗ · pubmed ↗
- 7Papi A Brightling C Pedersen SE Reddel HK Asthma Lancet 20183911012278380010.1016/S 0140-6736(17)33311-129273246 · doi ↗ · pubmed ↗
- 8Dharmage SC Perret JL Custovic A Epidemiology of Asthma in Children and Adults Front Pediatr 2019724624610.3389/fped.2019.0024631275909 PMC 6591438 · doi ↗ · pubmed ↗