Successful Use of Calcium Chloride in Acute Calcium Channel Blocker Overdose With Shock: A Case Report
Shunsuke Nakamura, Natsuyo Shinohara

TL;DR
A 60-year-old woman with severe amlodipine overdose showed rapid improvement after calcium chloride treatment when standard therapies failed.
Contribution
Demonstrates calcium chloride's effectiveness in severe CCB overdose cases unresponsive to conventional treatments.
Findings
Calcium chloride led to rapid hemodynamic improvement in a patient with CCB overdose.
Standard treatments like calcium gluconate and catecholamines were ineffective in this case.
The case suggests calcium chloride could be a first-line antidote for severe CCB overdose.
Abstract
Calcium channel blockers (CCBs) are widely used to treat hypertension and tachyarrhythmias. However, an overdose can lead to severe toxicity, resulting in bradycardia, hypotension, and shock. Standard treatments, including calcium gluconate and catecholamines, may be ineffective in severe cases. This study reports a 60-year-old female with hypotensive shock following an intentional overdose of amlodipine. Despite the initial treatment with calcium gluconate, glucagon, and catecholamines, hemodynamic instability persisted. However, the intravenous administration of calcium chloride resulted in rapid hemodynamic improvement, allowing eventual recovery. This case highlights the potential of calcium chloride as a first-line antidote for severe CCBs overdose refractory to conventional treatments.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
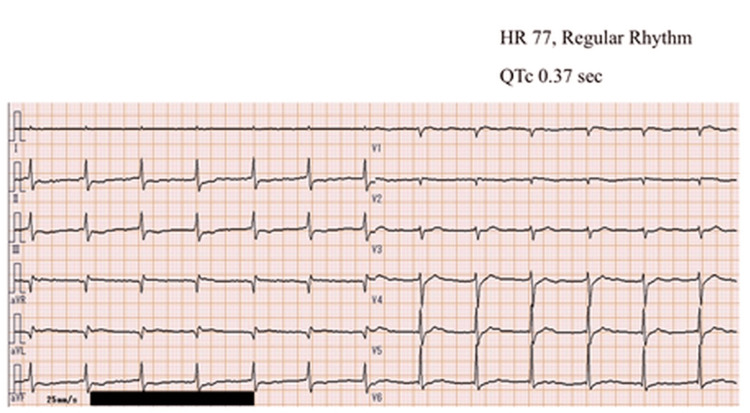 Figure 1
Figure 1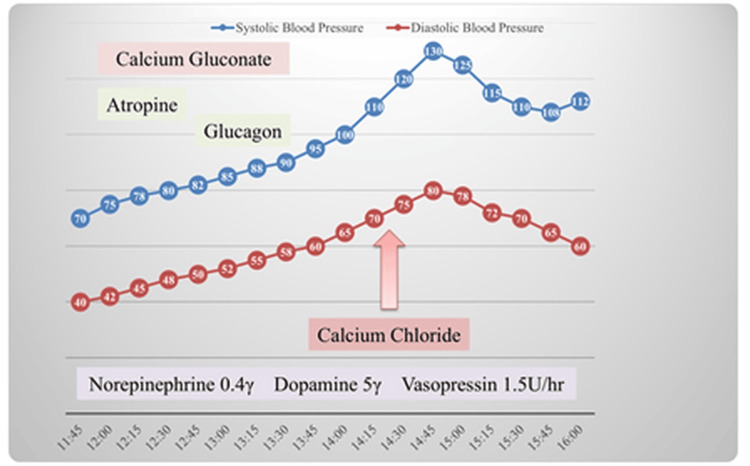 Figure 2
Figure 2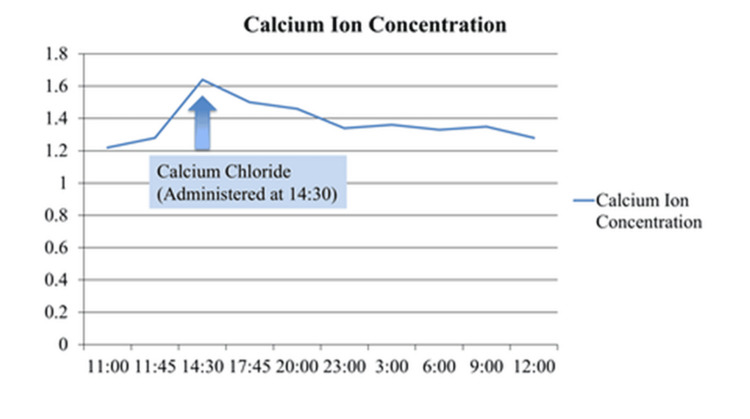 Figure 3
Figure 3| Test | Result | Units | Reference values |
| White blood cell | 11240 | /μL | 3300-8600 |
| Red blood cell | 4.48*106 | /μL | 4.35-5.55*106 |
| Hemoglobin | 12.9 | g/dL | 13.7-16.8 |
| Hematocrit | 39.3 | % | 40.7-50.1 |
| Platelet | 173*103 | /μL | 155-348*103 |
| Aspartate aminotransferase | 869 | U/L | 13-30 |
| Alanine aminotransferase | 551 | U/L | Oct-42 |
| Lactate dehydrogenase | 801 | U/L | 124-222 |
| Urea nitrogen | 31.9 | U/L | 20-Aug |
| Creatinine | 1.71 | mg/dL | 0.65-1.07 |
| Total bilirubin | 0.8 | mg/dL | 0.4-1.5 |
| C-reactive protein | 0.1 | mg/dL | <0.14 |
| Sodium | 140 | mmol/L | 138-145 |
| Potassium | 3.6 | mmol/L | 3.6-4.8 |
| Chlorine | 102 | mmol/L | 101-108 |
| Albumin | 3.5 | g/dL | 4.1-5.1 |
| PT(%) | 134 | % | 80-120 |
| PT-international normalized ratio | 0.86 | 0.9-1.1 | |
| Activated partial thromboplastin time | < 23.0 | second | 25-40 |
| Fibrinogen | 333 | mg/dL | 200-400 |
| D-dimer | 1.1 | μg/mL | <1.0 |
| pH | 7.33 | 7.35-7.45 | |
| FiO2 | 0.21 | - | |
| PaO2 | 113 | mmHg | 80-100 |
| PaCO2 | 30 | mmHg | 35-45 |
| HCO3- | 15.8 | mmol/L | 22-26 |
| Lac | 9.6 | mmol/L | 0.5-2.2 |
| BE | -8.8 | mmol/L | -2 to +2 |
| Glu | 350 | mg/dL | 70-140 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoisoning and overdose treatments · Cardiac Arrest and Resuscitation · Cardiac electrophysiology and arrhythmias
Introduction
Calcium channel blockers (CCBs) are commonly prescribed for hypertension and dysrhythmias, but overdose can cause life-threatening toxicity [1]. The underlying toxicity mechanism involves the inhibition of L-type calcium channels, causing reduced intracellular calcium, impaired myocardial contractility, and vasodilation, ultimately resulting in hypotension and shock [2]. Recent reports have indicated the efficacy of calcium chloride in the treatment of acute drug poisoning caused by CCBs. They exert toxicity by binding to the α1 subunit of the L-type Ca^2+^ channel and inhibiting Ca2+ influx. This results in decreased myocardial contractility, peripheral vascular resistance, and suppression of insulin secretion, leading to acute circulatory failure and metabolic acidosis [3-5].
Conventional treatment includes intravenous fluids, calcium supplementation, glucagon, and high-dose catecholamines; however, these therapies may prove ineffective in severe cases. Recent studies have shown that ionized calcium is directly available via calcium chloride, making it an efficient agent than calcium gluconate in managing acute toxicity [2]. However, calcium chloride is typically administered via a central venous catheter due to its vascular irritancy. Its higher threshold for use compared to calcium gluconate is a disadvantage. Additionally, high-dose insulin euglycemia therapy (HIET) has emerged as a promising adjunctive therapy for patients with CCB overdose who do not respond to conventional treatments [6].
This report presents a case of acute amlodipine overdose in which calcium chloride successfully stabilized circulation after standard treatments failed.
Case presentation
A 60-year-old female with a medical history of hypertension, left cerebral hemorrhage, and prior emergency transport for a suicide attempt ingested 390 mg of amlodipine in a suicide attempt. The following morning, the patient was presented to a local clinic with altered consciousness and hypotension. Thereafter, she was transferred to our emergency department. The preliminary vitals were recorded as follows: Glasgow Coma Scale (GCS): E3V4M5, pulse: 70 bpm, sinus rhythm, respiration rate: 20 breaths/min, SpO_2_: 98% on room air, temperature: 35.9°C, echocardiography: diffuse hypodynamic state. Blood pressure could not be measured, whereas 12-lead electrocardiography (ECG) showed no QT prolongation, with a QTc of 0.37 seconds (Figure 1).
12-lead electrocardiogram at presentation.The electrocardiogram on admission shows sinus rhythm with QTc 0.37 seconds.
As demonstrated in Table 1, the initial laboratory data indicated the presence of severe circulatory failure and liver damage.
Continuous intravenous infusions of norepinephrine (0.4 μg/kg/min), dopamine (5 μg/kg/min), vasopressin (1.5 units/hour), and other medications such as atropine, calcium gluconate, and glucagon were administered intravenously as required. However, the systolic blood pressure remained at 70 mmHg. Owing to persistent hypotension, the patient was initially administered intravenous fluids, calcium gluconate, glucagon, and catecholamines, but these did not achieve the desired hemodynamic stability. Therefore, considering the severity of the circulatory failure, intravenous calcium chloride (2%) administration was initiated at 14:30 (the administration of the 20 ml solution was conducted intravenously over a period of approximately five minutes), which resulted in a significant improvement in blood pressure and perfusion (Figure 2).
The course after admission.Hemodynamic response to calcium chloride administration.
Immediately after the aforementioned treatment, blood calcium ion concentrations increased marginally (Figure 3).
The blood calcium ion concentration.This figure shows the changes in blood calcium ion concentration (mmol/L) over time, highlighting a peak following the administration of calcium chloride at 14:30.
The patient’s hospital course is outlined below. On hospital day (HD) 2, the patient developed paroxysmal atrial fibrillation, which was managed with intermittent calcium chloride administration and electrolyte correction. By HD 5, the patient was transferred from the intensive care unit and finally discharged after the psychiatric evaluation on HD 7. Forensic procedures have not been conducted.
Discussion
Recent reports have indicated the efficacy of calcium chloride in the treatment of acute drug poisoning caused by CCBs. They exert toxicity by binding to the α1 subunit of the L-type Ca^2+^ channel and inhibiting Ca^2+^ influx. This results in decreased myocardial contractility, peripheral vascular resistance, and suppression of insulin secretion, leading to acute circulatory failure and metabolic acidosis [3-5].
While calcium gluconate is frequently employed in the treatment of CCB poisoning, its efficacy is contingent on the time elapsed, as it requires hepatic metabolism to increase the ionized calcium concentration in the blood. Conversely, calcium chloride does not involve hepatic metabolism and can expeditiously augment the ionized calcium concentration in blood. Consequently, calcium chloride has been postulated to be more effective in cases of acute circulatory failure; despite the administration of calcium gluconate, glucagon, and high-dose catecholamines, these interventions were insufficient [2,7-9].
Hence, this case highlighted the potential benefits of calcium chloride as a primary counter-agent for CCB poisoning, especially in case of acute circulatory collapse. In critical situations, such as the present case, where the patient exhibits severe circulatory or hepatic failure, it is preferable to administer the drug either by promptly securing a central venous catheter or by administering it slowly and carefully through a peripheral vein.
Conclusions
In calcium antagonist poisoning where the patient does not respond to calcium gluconate or other treatments, calcium chloride administration is an effective option. However, in acute circulatory failure, such as the aforementioned case, calcium chloride is believed to be the optimal choice because of its rapid increase in ionized calcium concentration in the blood without the need for hepatic metabolism.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Calcium channel blocker toxicity Stat Pearls [Internet] Chakraborty RK Hamilton JR Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 537147/
- 2Two cases of diltiazem poisoning treated with calcium chloride (Article in Japanese)JJAAM Ishikawa E Iseki K Seino K 236242222011 https://www.jstage.jst.go.jp/article/jjaam/22/5/22_5_236/_article/-char/ja/
- 3Management of beta-adrenergic blocker and calcium channel antagonist toxicity Emerg Med Clin North Am Kerns W 2nd 3093312520071748202210.1016/j.emc.2007.02.001 · doi ↗ · pubmed ↗
- 4Treatment of poisoning caused by beta-adrenergic and calcium-channel blockers Am J Health Syst Pharm Shepherd G 182818356320061699062910.2146/ajhp 060041 · doi ↗ · pubmed ↗
- 5Insulin-glucose as adjunctive therapy for severe calcium channel antagonist poisoning J Toxicol Clin Toxicol Yuan TH Kerns WP 2nd Tomaszewski CA Ford MD Kline JA 4634743719991046524310.1081/clt-100102437 · doi ↗ · pubmed ↗
- 6Critical management of severe hypotension caused by amlodipine toxicity managed with hyperinsulinemia/euglycemia therapy supplemented with calcium gluconate, intravenous glucagon and other vasopressor support: review of literature Cardiol Res Kumar K Biyyam M Bajantri B Nayudu S 4649920182947938610.14740/cr 646w PMC 5819629 · doi ↗ · pubmed ↗
- 7A case of calcium antagonist overdose in which the administration of calcium chloride was successful (Article in Japanese)J-STAGE Nohara H Arino S Imamura T 366369392019 https://www.jstage.jst.go.jp/article/jaamkanto/39/3/39_366/_article/-char/ja/
- 8Plasma ionic calcium levels following injection of chloride, gluconate, and gluceptate salts of calcium J Thorac Cardiovasc Surg White RD Goldsmith RS Rodriguez R Moffitt EA Pluth JR 609613711976 https://pubmed.ncbi.nlm.nih.gov/1263543/1263543 · pubmed ↗