Rapid Differentiation of False Positives of Galactomannan Related to Contaminated Intravenous Fluids via a Pharmacokinetics Model and Innovative Web-Based Tool
Raeseok Lee, Suein Choi, Hwajun Cha, Dukhee Nho, Sung-Yeon Cho, Seunghoon Han, Dong-Gun Lee

TL;DR
A new tool helps doctors quickly tell the difference between real fungal infections and false test results from contaminated IV fluids.
Contribution
A pharmacokinetic model and web-based tool were developed to rapidly identify false positives in galactomannan testing.
Findings
False positives were identified within 24 hours using galactomannan kinetics.
The tool improves diagnostic accuracy and supports early clinical decisions.
It reduces unnecessary interventions for patients.
Abstract
This study developed a pharmacokinetic model and web-based tool to distinguish true invasive aspergillosis from false positives caused by contaminated fluids. By analyzing galactomannan kinetics, false positives were identified within 24 hours, improving diagnostic accuracy and aiding clinicians in early decision making while minimizing unnecessary interventions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
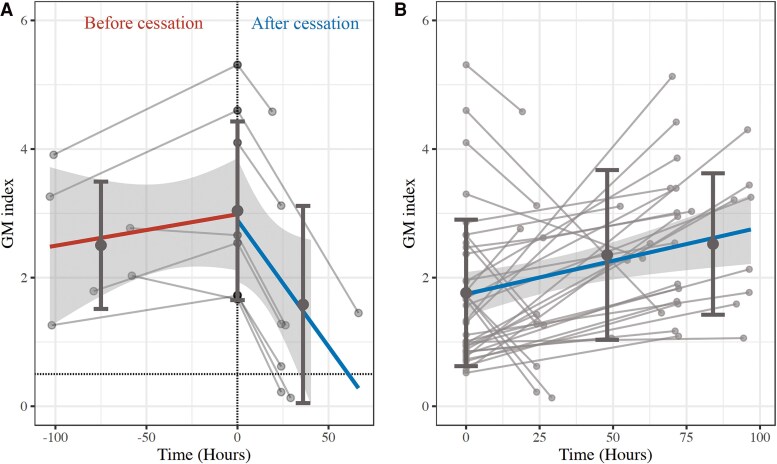 Figure 1
Figure 1| False Positive (n = 8) | True IA (n = 30) | Total (n = 38) |
| |
|---|---|---|---|---|
| Age, y | 42.5 (28.5–61.0) | 62.0 (53.0–67.0) | 61.0 (48.0–66.0) | .031 |
| Sex: male | 4 (50.0) | 16 (53.3) | 20 (52.6) | >.99 |
| Diagnosis | .742 | |||
| ALL | 2 (25.0) | 5 (16.7) | 7 (18.4) | |
| AML | 5 (62.5) | 14 (46.7) | 19 (50.0) | |
| Lymphoma | 1 (12.5) | 3 (10.0) | 4 (10.5) | |
| MDS | 0 (0.0) | 1 (3.3) | 1 (2.6) | |
| Myelofibrosis | 0 (0.0) | 1 (3.3) | 1 (2.6) | |
| Multiple myeloma | 0 (0.0) | 6 (20.0) | 6 (15.8) | |
| eGFR | 133.5 (102.5–164.5) | 136.0 (101.0–152.0) | 136.0 (101.0–154.0) | .839 |
| Severe hepatic dysfunction | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| GM index | ||||
| Initial | 2.6 (1.7–4.3) | 1.6 (0.8–1.9) | 1.6 (0.9–2.4) | .003 |
| Follow-up | 1.3 (0.4–2.3) | 2.5 (1.6–3.2) | 2.3 (1.4–3.1) | .047 |
| Time difference, h | 24.0 (24.0–27.8) | 71.7 (62.6–91.2) | 71.1 (29.2–72.3) | .001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPolysaccharides and Plant Cell Walls · Polysaccharides Composition and Applications · Phytochemistry and Biological Activities
The Aspergillus antigen galactomannan (GM) assay is a key diagnostic tool for invasive aspergillosis (IA) due to the challenges of culturing Aspergillus and the limitations of histologic diagnostics [1, 2]. However, its diagnostic accuracy is often undermined by false-positive results, complicating clinical interpretation [3–5].
False positives have been identified from GM-contaminated fluids and successfully intervened by modifying the manufacturing process [3]. Yet, this problem persists, particularly with the ongoing use of mold in the production of fluids and β-lactam antibiotics, which significantly increase the risk of recurrent false positives [3, 6–8].
This study aimed to differentiate GM false positives from true IA by analyzing GM kinetics. We also developed and evaluated a software tool designed to assist clinicians in accurately interpreting GM results when false positives are suspected.
METHODS
Study Design and Setting
The case group (false-positive GM) included patients confirmed to have GM false positivity between July and August 2023 [3]. We selected patients whose GM index of contaminated fluid and subsequent changes in serum GM index were measured at 0 (pretest), 24, and 48 hours after discontinuing contaminated fluids. For GM kinetics modeling, a control group (true-positive GM) was included from patients diagnosed with proven or probable IA between January 2022 and June 2023, a period with a low probability of false positives [3]. Control cases were selected when the GM index was measured at least twice before antimold active agents were administered. Classification followed established criteria and was determined via consensus of 2 infectious disease specialists [1, 9].
The Platelia Aspergillus GM assay (Bio-Rad) was used to quantify GM index. The study protocol was approved by the institutional review board of Seoul St Mary's Hospital (KC23WISI0594), and the requirement for written informed consent was waived.
Definitions of Covariates
We reviewed electronic medical records and collected covariates potentially affecting GM kinetics, including age, sex, glomerular filtration rate (GFR), and hepatic function based on the Child-Pugh classification [10]. In the model, GFR values >100 mL/min/1.73 m^2^ were capped at 100 mL/min/1.73 m^2^. Additionally, Child-Pugh class A and B were defined as mild to moderate hepatic dysfunction, whereas class C was defined as severe dysfunction.
Population Pharmacokinetic Modeling
GM kinetics were analyzed by nonlinear mixed effects modeling, with all concentration-time data modeled simultaneously. The final model was selected according to the bayesian information criterion, maximizing the likelihood. Baseline characteristics (GFR, age, and major comorbidities) were evaluated as potential covariates. Detailed methods are described in the supplementary methods.
Software Development
A web-based application was developed with R Shiny and the mrgsolve package to model the GM index profile based on the final pharmacokinetic model. The application was designed to predict false-positive GM results and recommend the minimum monitoring duration required to distinguish outcomes based on the initial GM index.
RESULTS
Baseline Patient Characteristics
Of 97 patients confirmed to have GM false positivity, 8 were selected for the case group. These patients had initial serum and fluid GM results, as well as follow-up GM assay results after contaminated fluids were discontinued. The control group consisted of 30 patients with proven or probable IA, each having a GM index measured at least twice prior to antifungal therapy. Patients in the case group were younger but had a higher initial GM index as compared with the control group (Table 1).
GM Pharmacokinetic Modeling
Following the discontinuation of contaminated fluids, GM index levels rapidly decreased in the false-positive group but significantly increased in the true IA group (P < .05; Table 1, Figure 1). The false-positive group had a higher initial GM index (median, 2.6; IQR, 1.7–4.3) as compared with the true IA group (median, 1.6; IQR, 0.8–1.9). GM concentrations in contaminated dextrose-containing fluids ranged from 8 to 4320 ng/mL, with a median 4.2 ng/mL (range, 3.2–6.6).
Time-concentration change of the galactomannan index: A, following the discontinuation of the galactomannan-contaminated solution; B, from the time when it turned positive until just before the initiation of antifungal therapy in patients with confirmed invasive aspergillosis. Solid line, median change; gray circle, individual observation; dashed line, 0.5 threshold for positive indices. Dark gray circle, mean value at each binned time frame; dark gray vertical line, ± standard deviation (SD) around the mean; gray shading, 95% CI interval of regression line. GM, galactomannan.
Pharmacokinetic modeling indicated a GM synthesis rate of 0.127 and an elimination rate constant of 0.030, with no significant covariates (Supplementary Table 1). The model predicted that, for an initial GM index of 3.0, levels would typically become negative (GM index <0.5) within a median of 2.3 days (95% CI, 1.51–3.8 days), with an estimated half-life of 23.6 hours (95% CI, 12.2–43.4 hours), indicating complete clearance within approximately 4.8 days. Simulations suggested that most false positives can be confirmed within 18 hours of stopping exposure, though lower initial GM indices require longer monitoring (Supplementary Table 2).
Performance of Developed Web-Based Software
The developed web-based application, available at https://mychloe00.shinyapps.io/galactomannan/, accurately predicted the likelihood of true IA vs false positivity based on GM indices and the time intervals between measurements (area under the receiver operating characteristic curve, 0.93). The tool also recommended the optimal time to discontinue a suspected source of contamination (Supplementary Figures 1 and 2).
DISCUSSION
This study demonstrated that GM false positives can be reliably distinguished from true IA cases within 24 hours by analyzing GM kinetics. The newly developed web-based tool provides clinicians with a practical, accessible means to simulate GM trends, significantly improving diagnostic accuracy for IA and reducing the risk of misinterpretation due to false positives.
False positives from GM contamination by Aspergillus used in carbohydrate fermentation have been consistently reported [3–8]. However, previous studies validating GM kinetics have primarily been conducted in animal models, with limited data available on human false-positive cases [10]. A previous study indicated a GM half-life of 2.4 days and a clearance time of 5.5 days after discontinuation of penicillin antibiotics [11]. Yet, as early diagnosis and treatment within 48.0 hours of infection are critical for therapeutic prognosis, waiting 5 days to determine false positivity is impractical [11].
Our findings show that the GM half-life in false-positive cases is much shorter—approximately 23.6 hours—allowing for false positivity to be differentiated within 18.0 hours. This early detection ability enables clinicians to diagnose IA accurately while minimizing the risk of misdiagnosing false positives. Since the GM index in true IA does not significantly decrease within 4 to 6 days of azole treatment, our model may offer a reliable approach for distinguishing false positives even up to a week after initiation of mold-active therapy [10]. However, consideration of parameters such as host factors, clinical findings, and radiologic features are crucial in diagnosis of IA.
The web-based software developed in this study is the first clinical application designed to distinguish false positives within 24 hours. This tool improves early diagnosis and therapeutic decision making for true IA while reducing unnecessary interventions triggered by false positives. Additionally, the tool detects contamination from other intravenous sources that exhibit similar GM elevation patterns, such as piperacillin/tazobactam [11]. In addition, even when GM patterns differ, clinicians can use the software to compare observed GM changes after discontinuing the suspected false-positive sources against simulated reference values, thereby enhancing their diagnostic decision making. Further research and modeling are needed to extend its application to false positivity arising from gastrointestinal absorption of contaminated materials. The software is freely available on the provided website.
Despite its strengths, this study has some limitations. First, the GM kinetics model could not be validated with external data due to a lack of additional suspected false-positive cases at our institution [3]. Second, the rate of GM increase varied by Aspergillus species. However, among the 30 true IA cases, only 3 were culture positive, and all were identified as Aspergillus fumigatus, thus preventing species-specific modeling [12]. Third, the applicability of the model to other sources of false positivity remains uncertain, and further validation studies are required for this. Finally, although we included a control group during the period of low probability of using contaminated fluids, the possibility of GM-contaminated dextrose fluid infused to the control group was not completely ruled out.
In conclusion, GM false positives can be effectively differentiated from true IA cases within 24 hours by analyzing GM kinetics after discontinuation of contaminated sources. The web-based tool developed from this model offers clinicians a valuable resource for accurately diagnosing IA and reducing false positives.
Supplementary Material
ofaf088_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Donnelly JP, Chen SC, Kauffman CA, et al Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis 2020; 71:1367–76.31802125 10.1093/cid/ciz 1008 PMC 7486838 · doi ↗ · pubmed ↗
- 2Lee S-O. Diagnosis and treatment of invasive mold diseases. Infect Chemother 2023; 55:10–21.36603818 10.3947/ic.2022.0151 PMC 10079437 · doi ↗ · pubmed ↗
- 3Lee R, Yoo IY, Oh EJ, et al Dextrose-containing fluids causing false-positive serum galactomannan: a case-control study and interrupted time series analysis. Clin Microbiol Infect 2024; 30:682.e 1–4.10.1016/j.cmi.2024.01.01938309324 · doi ↗ · pubmed ↗
- 4Martín-Rabadán P, Gijón P, Fernández RA, Ballesteros M, Anguita J, Bouza E. False-positive Aspergillus antigenemia due to blood product conditioning fluids. Clin Infect Dis 2012; 55:e 22–7.22610929 10.1093/cid/cis 493 · doi ↗ · pubmed ↗
- 5Racil Z, Kocmanova I, Lengerova M, Winterova J, Mayer J. Intravenous PLASMA-LYTE as a major cause of false-positive results of Platelia Aspergillus test for galactomannan detection in serum. J Clin Microbiol 2007; 45:3141–2.17670932 10.1128/JCM.00974-07PMC 2045287 · doi ↗ · pubmed ↗
- 6Shin DW, Cho J, Choi KS, et al False-positive results of galactomannan assays in patients administered glucose-containing solutions. Sci Rep 2024; 14:2552.38291146 10.1038/s 41598-024-53116-x PMC 10827775 · doi ↗ · pubmed ↗
- 7Chong E, Ko JH, Kim DR, et al False-positive Aspergillus galactomannan immunoassay in the glucose component of total parenteral nutrition products. Microbiol Spectr 2023; 11:e 0167323.37800931 10.1128/spectrum.01673-23PMC 10715174 · doi ↗ · pubmed ↗
- 8Chang E, Kang SW, Huh JW, et al False positive Aspergillus galactomannan assay results caused by specific parenteral nutrition. Med Mycol 2023; 61:myad 094.37656877 10.1093/mmy/myad 094 · doi ↗ · pubmed ↗