Comparison of pegaspargase with concurrent radiation vs. P-GEMOX with sequential radiation in early-stage NK/T-cell lymphoma
DEMEI FENG, SHENRUI BAI, GUANJUN CHEN, BIBO FU, CAILU SONG, HAILIN TANG, LIANG WANG, HUA WANG

TL;DR
This study compares two treatment regimens for early-stage NKTCL and finds that both are similarly effective, though one offers a shorter treatment cycle.
Contribution
The study provides a direct comparison of two treatment strategies for NKTCL using propensity score matching to balance patient characteristics.
Findings
P+CCRT achieved 100% overall response rate and 100% complete response rate, compared to 88.5% and 76.9% for P-GEMOX + SERT.
Both regimens showed similar 3-year overall survival rates (92.3%), but P+CCRT had better progression-free survival (92.3% vs. 80.8%).
Adverse events were comparable between the two treatment groups.
Abstract
The optimal treatment strategy for early-stage natural killer/T-cell lymphoma (NKTCL) remains unclear. This study aimed to evaluate and compare the clinical outcomes and adverse events (AEs) associated with two treatment regimens for early-stage NKTCL: pegaspargase with concurrent radiation therapy (P+CCRT) and pegaspargase, gemcitabine, and oxaliplatin (P-GEMOX) with sequential radiation therapy (SERT). Propensity score matching (PSM) was employed to ensure balanced comparison between these regimens. We assessed the efficacy of P+CCRT from a phase II trial and P-GEMOX combined with SERT using real-world data. PSM was conducted at a 1:1 ratio with a caliper of 0.18 to align baseline characteristics between the treatment groups. Key outcomes analyzed included overall response rate (ORR), complete response rate (CR), progression-free survival (PFS), overall survival (OS), and AEs.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
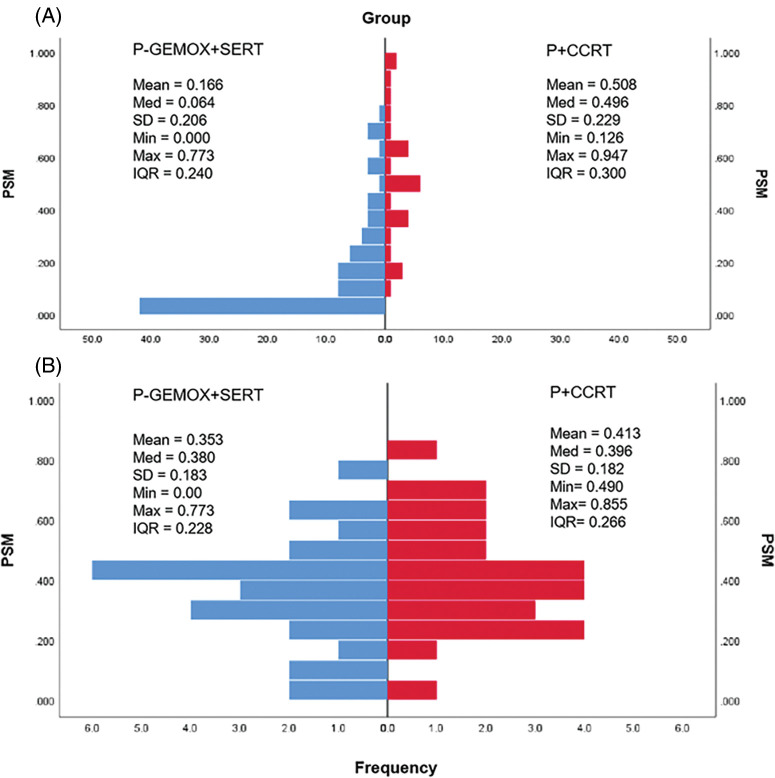 Figure 1
Figure 1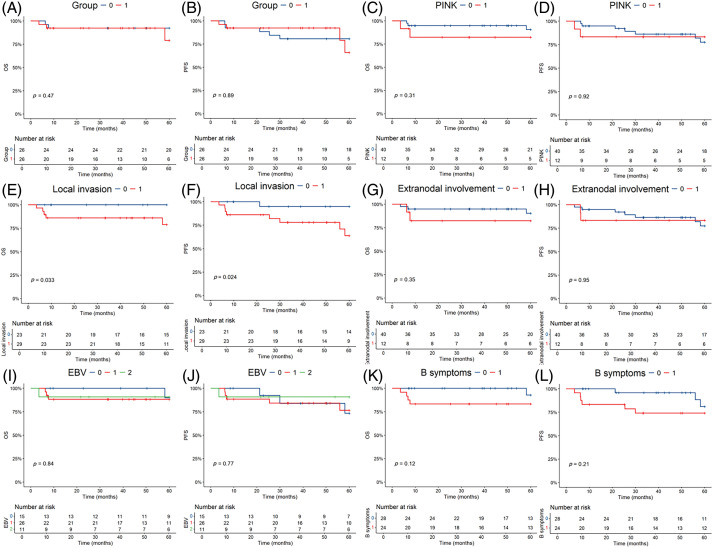 Figure 2
Figure 2| Characteristics | P-GEMOX+SERT (n = 83, %) | P+CCRT (n = 28, %) |
|
|---|---|---|---|
| Age | 1.000 | ||
| ≤60 | 71 (85.5%) | 24 (85.7%) | |
| >60 | 12 (14.5%) | 4 (14.3%) | |
| Sex | 0.500 | ||
| Male | 53 (63.9%) | 20 (71.4%) | |
| Female | 30 (36.1%) | 8 (28.6%) | |
| B symptoms | 0.375 | ||
| Absence | 47 (56.6%) | 19 (67.9%) | |
| Presence | 36 (43.4%) | 9 (32.1%) | |
| ECOG performance status | 0.404 | ||
| 0/1 | 69 (83.1%) | 21 (75.0%) | |
| ≥2 | 14 (16.9%) | 7 (25.0%) | |
| Ann arbor stage | 0.062 | ||
| I/II | 72 (86.7%) | 28 (100%) | |
| III/IV | 11 (13.3%) | 0 (0%) | |
| Primary site | 0.006 | ||
| Nasal | 65 (78.3%) | 28 (100%) | |
| Non-nasal | 18 (21.7%) | 0 (0%) | |
| Local invasion | 0.650 | ||
| No | 28 (33.7%) | 11 (39.3%) | |
| Yes | 55 (66.3%) | 17 (60.7%) | |
| Lymph-node involvement | 0.144 | ||
| None | 38 (45.8%) | 16 (57.1%) | |
| Regional | 29 (34.9%) | 11 (39.3%) | |
| Distant | 16 (19.3%) | 1 (3.6%) | |
| Extranodal involvement | 0.795 | ||
| 0 or 1 | 65 (78.3%) | 21 (75.0%) | |
| ≥2 | 18 (21.7%) | 7 (25.0%) | |
| Bone-marrow involvement | 0.570 | ||
| No | 80 (96.4%) | 28 (100%) | |
| Yes | 3 (3.6%) | 0 (0%) | |
| Initial SUVmax | 0.346 | ||
| ≤12.1 | 25 (30.1%) | 6 (21.4%) | |
| >12.1 | 30 (36.1%) | 8 (28.6%) | |
| Unknown | 28 (33.7%) | 14 (50.0%) | |
| Epstein-Barr virus DNA in blood | 0.553 | ||
| Detectable | 49 (59.0%) | 13 (46.4%) | |
| Non-detectable | 20 (24.1%) | 9 (32.1%) | |
| Unknown | 14 (16.9%) | 6 (21.4%) | |
| Serum lactate dehydrogenase | 0.795 | ||
| Normal | 65 (78.3%) | 21 (75.0%) | |
| Increased | 18 (21.7%) | 7 (25.0%) | |
| Serum albumin concentration | 0.457 | ||
| ≤35 g/L | 21 (25.3%) | 5 (17.9%) | |
| >35 g/L | 62 (74.7%) | 23 (82.1%) | |
| Lymphocyte count | 0.426 | ||
| ≤1000 per mm3 | 16 (19.3%) | 8 (28.6%) | |
| >1000 per mm3 | 67 (80.7%) | 20 (71.4%) | |
| Haemoglobin concentration | 0.297 | ||
| ≤100 g/L | 9 (10.8%) | 1 (3.6%) | |
| >100 g/L | 74 (89.2%) | 27 (96.4%) | |
| Platelet count | 0.328 | ||
| ≤75,000 per mm3 | 5 (6.0%) | 0 (0%) | |
| >75,000 per mm3 | 78 (94.0%) | 28 (100%) |
| Characteristics | P-GEMOX+SERT (n = 26, %) | P+CCRT (n = 26, %) |
|
|---|---|---|---|
| Age | 0.668 | ||
| ≤60 | 24 (92.3%) | 23 (88.5%) | |
| >60 | 2 (7.7%) | 3 (11.5%) | |
| Sex | 0.548 | ||
| Male | 17 (65.4%) | 19 (73.1%) | |
| Female | 9 (34.6%) | 7 (26.9%) | |
| B symptoms | 0.095 | ||
| Absence | 12 (46.2%) | 18 (69.2%) | |
| Presence | 14 (53.8%) | 8 (30.8%) | |
| ECOG performance status | 0.726 | ||
| 0/1 | 22 (84.6%) | 20 (76.9%) | |
| ≥2 | 4 (15.4%) | 6 (23.1%) | |
| Ann arbor stage | |||
| I | 21 (80.8%) | 16 (61.5%) | 0.126 |
| II | 5 (19.2%) | 10 (38.5%) | |
| Primary site | 1.000 | ||
| Nasal | 25 (96.2%) | 26 (100%) | |
| Non-nasal | 1 (3.8%) | 0 (0%) | |
| Local invasion | 0.404 | ||
| No | 14 (53.8%) | 11 (42.3%) | |
| Yes | 12 (46.2%) | 15 (57.7%) | |
| Lymph-node involvement | 0.664 | ||
| None | 16 (61.5%) | 15 (57.7%) | |
| Regional | 8 (30.8%) | 10 (38.5%) | |
| Distant | 2 (7.7%) | 1 (3.8%) | |
| Extranodal involvement (n) | 1.000 | ||
| 0 or 1 | 20 (76.9%) | 20 (76.9%) | |
| ≥2 | 6 (23.1%) | 6 (23.1%) | |
| Bone-marrow involvement | |||
| No | 26 (100%) | 26 (100%) | |
| Yes | 0 (0%) | 0 (0%) | |
| Serum lactate dehydrogenase | 1.000 | ||
| Normal | 20 (76.9%) | 20 (76.9%) | |
| Increased | 6 (23.1%) | 6 (23.1%) | |
| Serum albumin concentration | 0.726 | ||
| ≤35 g/L | 5 (19.2%) | 4 (15.4%) | |
| >35 g/L | 21 (80.8%) | 22 (84.6%) | |
| Lymphocyte count | 0.743 | ||
| ≤1000 per mm3 | 5 (19.2%) | 7 (26.9%) | |
| >1000 per mm3 | 21 (80.8%) | 19 (73.1%) | |
| Haemoglobin concentration | 1.000 | ||
| ≤100 g/L | 0 (0%) | 0 (0%) | |
| >100 g/L | 26 (100%) | 26 (100%) | |
| Platelet count | |||
| ≤75,000 per mm3 | 0 (0%) | 0 (0%) | |
| >75,000 per mm3 | 26 (100%) | 26 (100%) |
| Response | Number of patients (%) | ||
|---|---|---|---|
| P-GEMOX+SERT | P+CCRT |
| |
| CR | 20 (76.9) | 26 (100) | 0.648 |
| PR | 3 (11.5) | 0 (0.0) | |
| SD | 0 (0.0) | 0 (0.0) | |
| PD | 3 (11.5) | 0 (0.0) | |
| ORR | 23 (88.5) | 26 (100) | |
| Group | Follow-up time, Median (IQR, months) | 3-y OS rate (%) | 95% CI | 3-y PFS rate (%) | 95% CI |
|---|---|---|---|---|---|
| GEMOX+SERT (N = 26) | 60 (58–60) | 92.3 | 82.6–100 | 80.8 | 65.7–95.8 |
| P+CCRT (N = 26) | 41 (10–59) | 92.3 | 82.6–100 | 92.3 | 82.6–100 |
| Toxicity | P-GEMOX+SERT (n = 26) | P+CCRT (n = 26) |
| ||
|---|---|---|---|---|---|
| Grades 1–2 | Grades 3–4 | Grades 1–2 | Grades 3–4 | ||
| Hematologic | |||||
| Leukopenia | 13 (50.0) | 4 (15.4) | 16 (61.5) | 3 (11.5) | 0.542 |
| Neutropenia | 9 (34.6) | 6 (23.1) | 12 (46.2) | 6 (23.1) | 0.618 |
| Anemia | 10 (38.5) | 3 (11.5) | 9 (34.6) | 0 (0.0) | 0.135 |
| Thrombocytopenia | 5 (19.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1.000 |
| Non-hematological adverse events | |||||
| Hypofibrinogenemia | 4 (15.4) | 2 (7.7) | 10 (38.5) | 4 (15.4) | 0.204 |
| Hypoalbuminemia | 7 (26.9) | 3 (11.5) | 17 (65.4) | 3 (11.5) | 0.046 |
| Prolonged APTT | 15 (57.7) | 1 (3.8) | 18 (69.2) | 1 (3.8) | 0.685 |
| Hyperbilirubinemia | 4 (15.4) | 0 (0.0) | 5 (19.2) | 0 (0.0) | 1.000 |
| ALT elevation | 13 (50.0) | 3 (11.5) | 18 (69.2) | 1 (3.8) | 0.309 |
| AST elevation | 12 (46.2) | 1 (3.8) | 8 (30.8) | 0 (0.0) | 0.275 |
| Nausea | 15 (57.7) | 1 (3.8) | 17 (65.4) | 0 (0.0) | 0.541 |
| Vomiting | 17 (65.4) | 1 (3.8) | 10 (38.5) | 0 (0.0) | 0.077 |
| Anorexia | 13 (50.0) | 1 (3.8) | 14 (53.8) | 0 (0.0) | 0.702 |
| Mucositis | 17 (65.4) | 0 (0.0) | 13 (50.0) | 0 (0.0) | 0.278 |
- —National Natural Science Foundation of China
- —Natural Science Foundation of Guangdong Province
- —National Natural Science Foundation of China
- —Basic and Applied Basic Research Foundation of Guangdong Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · Cancer Immunotherapy and Biomarkers · Lung Cancer Treatments and Mutations
Introduction
Natural killer/T cell lymphoma (NKTCL) arises from the mature natural killer cells and T cells. NKTCL is a pathogenic subtype of the malignant aggressive lymphoma that predominantly affects Asian and South American populations [1]. The pathophysiology of NKTCL is complex and not fully understood, though it is closely associated with Epstein-Barr virus (EBV) infection [2]. NKTCL is classified into nodal (nNKTCL) and extra-nodal (eNKTCL) forms, with eNKTCL being the more common [3].
Conventional treatments, such as anthracycline-based regimens like CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone), are often insufficient in NKTCL due to the presence of a multidrug-resistant glycoprotein that is solely produced by tumor cells [4]. Consequently, the 5-year overall survival rate of NKTCL patients is less than 50% [5]. Current treatment options for NKTCL include local radiotherapy for early-stage local lesions [5,6], as well as combinations like GELOX (gemcitabine, L-asparaginase, and oxaliplatin) [7], SMILE (dexamethasone, methotrexate, ifosfamide, L-asparaginase, and etoposide), and DDPG (pegaspargase, gemcitabine, cisplatin, and dexamethasone) [8]. These regimens may be used in conjunction with sequential or concurrent chemotherapy and radiotherapy. While these combinatorial therapies have improved patient outcomes, they often come with frequent and severe adverse effects [9,10].
Recent studies have shown that P-GEMOX followed by sequential radiation therapy is effective for early-stage NKTCL [11]. However, the high doses of chemotherapy involved can lead to significant hematological and liver function side effects [12]. Additionally, there is evidence suggesting initiating radiation therapy earlier may enhance treatment efficacy for early-stage NKTCL patients [13]. To investigate the potential benefits of earlier radiation therapy combined with chemotherapy, we conducted a phase two clinical trial assessing pegaspargase monotherapy in conjunction with concurrent radiation therapy (P+CCRT). This approach aimed to provide a simpler and more effective treatment option for patients with early-stage NKTCL. This trial demonstrated that the P+CCRT regimen was highly effective, with all patients achieving complete remission upon completion of the therapy and experiencing relatively few treatment-related side effects [14].
In our study, combined with SERT served as the control group, while P+CCRT was the experimental group. We employed a 1:1 propensity score matching method, creating 26 matched pairs for a total of 52 patients. The primary objective was to compare the response rates and adverse events of these two regimens, aiming to provide insights for optimizing treatment strategies for patients with NKTCL.
Method and Materials
Subjects and interventions
The study is a retrospective analysis based on a previously conducted phase two clinical trial, which included 30 untreated patients with early stage NKTCL between January 2016 and August 2019 [14]. For this analysis, we matched these patients 1:1 with individuals who received the P-GEMOX regimen followed by sequential radiotherapy at our facility, with diagnoses ranging from June 2007 to October 2020. To ensure comparability between the two groups, we applied identical inclusion and exclusion criteria. Inclusion criteria were as follows: biopsy-confirmed early-stage NKTCL (Ann Arbor stage IE or IIE) ENKTL, untreated, age 18 years or older, with an expected survival time >3 months, Eastern Cooperative Oncology Group (ECOG) performance status score of 0 to 2, and adequate hematological (absolute neutrophil count >1.5 × 10^9^/L, platelet count > 80 × 10^9^/L), renal (serum creatinine ≤1.5 mg/dL, creatinine clearance ≥50 mL/min), and liver function (aminotransferase ≤2.5 × upper limit of normal [ULN], total bilirubin ≤1.5 × ULN). Exclusion criteria included any history or concurrent malignancies and medical conditions that could affect compliance with the study protocol. The research received approval from the Ethics Committee of Sun Yat-sen University Cancer Center (Approval number: B2018-053-01), and all participants provided written informed consent in accordance with the principles of the Declaration of Helsinki.
For the P-GEMOX +SERT treatment, pegaspargase 2000 IU/m^2^ was given intramuscularly on day 1; gemcitabine 1000 mg/m^2^ was administered intravenously on days 1 and 8; and oxaliplatin 130 mg/m^2^ was infused on day 1, with cycles lasting 21 days. The number of cycles was determined by the physician based on patient characteristics and response. Radiation therapy followed chemotherapy, with a total dose of 50.0 Gy. For the P+CCRT treatment, patients received radiation concurrently with two cycles of pegaspargase (2500 units/m^2^ every three weeks), followed by four additional cycles, totaling six cycles, with the radiation dose also at 50 Gy. Details of the comparison of the two regimens are presented in Table A1. Adverse events were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0.
Propensity score matching and Endpoints
Due to the limitations of randomizing participants in this retrospective observational study, we employed propensity score matching (PSM) to create 1:1 pairs of patients, aiming to eliminate statistical differences between the two treatment groups. A caliper of 0.18 was applied for this matching process [15,16]. To enhance comparability, we only included 28 patients from our center and excluded 2 patients from other centers. The baseline characteristics used for matching include age, sex, B symptoms, ECOG performance status, Ann Arbor stage, primary site, local infiltration, lymph node involvement, extranodal involvement, bone marrow involvement, serum lactate dehydrogenase, serum albumin concentration, lymphocyte count, hemoglobin concentration, and platelet count. The primary endpoints include ORR, CRR, and secondary endpoints include OS, PFS, the assessment of AEs associated with each treatment regimen. The Lugano criteria from 2014 were used to evaluate the response rate [17].
Statistical analysis
We utilized the chi-square test to examine differences in dichotomous variables between the groups. PFS was calculated from the date of diagnosis to the date of disease progression, relapse, death, or last follow-up, whichever occurred first. OS was measured from the date of diagnosis to the date of death due to any causes. PFS and OS were analyzed by using the Kaplan-Meier method to plot survival curves and employed the log-rank test to compare survival differences between different groups. We used SPSS software version 25.0 (IBM Corp., Armonk, NY, USA) for statistical analysis and R version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria) for propensity score matching and data visualization. A p-value of less than 0.05 was considered statistically significant.
Results
Basic clinical characteristics of the patients
Fig. 1 illustrates the distribution of propensity score for both the P-GEMOX and P+CCRT groups before and after matching. Tables 1–2 present the baseline clinical features of the patients before and after PSM. After applying PSM, 52 patients were included, with 26 in each group. In the P-GEMOX+SERT and P+CCRT groups, there were 2 and 3 patients over 60 years old, 12 and 18 with B symptoms, 5 and 10 at Ann Arbor stage II, and 21 and 16 at Stage I, respectively. Additionally, in the P-GEMOX+SERT group, 1 patient had a primary site was outside the nasal cavity, while all patients in the P+CCRT group had their primary site in the nasal cavity. Post-matching analysis using the chi-square test showed no statistically significant differences in the initial clinical features between the two groups. The characteristics of 83 patients from the real-world are presented in Table A2.
Histograms of the propensity score distribution in two groups. (A) the distribution before matching; (B) the distribution after matching. P-GEMOX, pegaspargase, gemcitabine, oxaliplatin; SERT, sequential radiation therapy; P+CCRT, pegaspargase with concurrent radiation therapy; PSM, propensity score matching; Med, median; SD, standard deviation; Min, minimum; Max, maximum; IQR, interquartile range.
Treatment outcomes and prognostic factors
Table 3 details the treatment outcomes for both groups. In the P-GEMOX+SERT group, 20 patients (76.9%) achieved CR and 3 patients (11.5%) had a partial response (PR), resulting in an ORR of 88.5%. In contrast, all 26 patients in the P+CCRT group achieved complete response (CR) by the end of treatment. The median follow-up time was 126 months (95% CI: 99–152 months) for the P-GEMOX+SERT group and 54 months (95% CI: 46–62 months) for the P+CCRT group. To account for the differences in follow-up duration, Kaplan-Meier (K–M) curves were standardized to 60 months. The 3-year OS and PFS rates in the P+CCRT group were both 92.3% (95% CI: 82.6%–100%), compared to 92.3% (95%CI: 82.6%–100%) and 80.8% (95% CI: 67.0%–97.4%) in the P-GEMOX+SERT group, the *p-*values for OS and PFS comparisons were 0.893 and 0.473, respectively (Table 4).
OS (Fig. 2A) and PFS (Fig. 2B) K–M survival curves revealed no statistically significant difference in the prognosis between the two groups. Among the prognostic factors, local invasion (Fig. 2E,F) was identified as a significant factor in early-stage patients. However, the prognostic index of natural killer lymphoma (PINK) score (Fig. 2C,D), extranodal involvement (Fig. 2G,H), detectable EBV DNA (Fig. 2I,J) and the presence of B-cell malignancy associated symptoms (Fig. 2K,L) did not show statistically significant prognostic value.
Kaplan-Meier survival analysis of the overall survival (OS) and progression-free survival (PFS) in all patients. The p-value reported in the figure is the result of the log-rank test. (A, B) OS and PFS stratified by the two different regimens. 0 = P-GEMOX, 1 = P+CCRT. (C, D) OS and PFS stratified by the Prognostic index for natural kill lymphoma (PINK). 0 = PINK Score is 0, 1 = PINK Score is 1. (E, F) OS and PFS stratified by the local invasion. 0 = No, 1 = Yes. (G, H) OS and PFS stratified by the extranodal involvement. 0 = No, 1 = Yes. (I, J) OS and PFS stratified by EBV DNA. 0 = Undetectable, 1 = Detectable, 2 = Unknown. (K, L) OS and PFS stratified by the B symptoms. 0 = No, 1 = Yes.
Adverse reactions
Adverse reactions in both the P-GEMOX+SERT and P+CCRT groups were predominantly mild (Grades 1–2). Severe adverse reactions (Grades 3–4) were mostly related to the hematologic system, including leukopenia (15.4% vs. 11.5%) and neutropenia (23.1% vs. 23.1%), with no significant differences observed. Additionally, 11.5% of patients in the P-GEMOX+SERT group experienced Grades 3–4 anemia, whereas no such cases were reported in the P+CCRT group. Neither group experienced severe thrombocytopenia. For non-hematologic adverse reactions, most were Grades 1–2, with the P+CCRT regimen showing a higher incidence of hypoalbuminemia (p = 0.046). Detailed data on common chemotherapy-related toxicities for both groups are summarized in Table 5.
Discussion
In this study, we have examined the potential effectiveness and adverse effects of two radiation and chemotherapy regimens in patients with early stage NKTCL. While our findings indicate that pegaspargase combined with concurrent radiation therapy may offer comparable clinical outcomes, no significant differences were observed in efficacy parameters between the two treatment groups.
Historically, basic local radiation was considered the most effective treatment for early-stage NKTCL [18]. Although some patients still experienced recurrence [19]. Similarly, anthracycline-based therapy, while commonly used, often led to relapse and low CR rates [20]. The addition of chemotherapy to radiation has markedly improved clinical outcomes for NKTCL patients [21]. For instance, earlier studies demonstrated relatively higher expression of P-glycoprotein as well as its associated mRNA in T-cell lymphoma [22]. Pegaspargase, a member of the ATP-binding cassette (ABC) transporter superfamily, has been identified as a significant factor in drug resistance for NK/T-cell lymphoma cells [23]. Its role in minimal residual lesions (MRD) also contribute to the risk of disease recurrence [24].
Pegaspargase can hydrolyze asparagine in the lymphoma cells that are unable to synthesize this essential amino acid to achieve its anti-tumor effect and was not affected by multidrug resistance of NKTCL as mentioned above, and has been reported to be effective against the NKTCL [25,26]. The polyethylene glycol covalent linkage form of pegaspargase can not only significantly prolong the half-life of the drug in the body but can also effectively reduce the chance of allergic reactions in the body [27].
We employed propensity score matching to account for baseline differences between the groups, ensuring a more accurate comparison. Our analysis demonstrated that P+CCRT achieved a significantly higher CRR of 100% compared to 76.9% in the P-GEMOX+SERT group, and ORR of 100% vs. 88.5%, respectively. Both regimens showed similar 3-year OS rates of 92.3%, but P+CCRT demonstrated a higher 3-year PFS rate at 92.3%, compared to 80.8% for P-GEMOX+SERT. The shorter treatment cycle and simpler administration of P+CCRT, involving intramuscular pegaspargase injections every three weeks and concurrent radiation, contributed to these improved outcomes. However, despite all patients achieving CR at the end of treatment, 1 patient (3.8%) in the P+CCRT group experienced local recurrence nine months later. This recurrence was associated with localized lesion invasion at initial diagnosis and a high Ki67 index.
In our phase II study, designed based on Simon’s optimal two-stage design, we aim to reject a 70% CR rate and support a target CR rate of 90% for early-stage ENKTL Our results surpassed this target, achieving a 100% CR rate [28]. To explore these findings, we compared the results from the phase II trial with real-world case series data.
The P+CCRT regimen, which did not involve intravenous chemotherapy, showed minimal hematology toxicity, with no grade 4 myelosuppression reported. Although pegaspargase is associated with several adverse effects such as altered coagulation function and pancreatitis [29,30]. The most severe adverse reactions in our study were grade 3 hypofibrinemia in 3 patients and grade 4 APTT prolongation in 1 patient. These were managed successfully with symptomatic treatment. No cases of pancreatitis were observed, and there was no therapy-related mortality. Both the prolonged APTT and grade four hypoalbuminemia found in the control group were not observed in the P+CCRT group.
Our study has limitations. The small sample size may affect the robustness and generalizability of our findings. Additionally, despite using propensity scores to control for observed variables, unmeasured confounding factors might still bias the results. Future research should aim to identify and mitigate the impact of these unmeasured variables to enhance the validity of the findings.
Conclusion
In conclusion, our trial indicates that pegaspargase combined with concurrent radiation therapy may offer comparable outcomes for patients with early-stage NKTCL. While the results are encouraging, the study’s limitations highlight the need for further large-scale, multi-center studies to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang H, Fu B-B, Gale RP, Liang Y. NK-/T-cell lymphomas. Leukemia. 2021;35(9):2460–8. doi:10.1038/s 41375-021-01313-2; 34117356 PMC 8410593 · doi ↗ · pubmed ↗
- 2Xiong J, Cui B-W, Wang N, Dai Y-T, Zhang H, Wang C, et al. Genomic and transcriptomic characterization of natural killer T Cell lymphoma. Cancer Cell. 2020;37(3):403–9.e 6. doi:10.1016/j.ccell.2020.02.005; 32183952 · doi ↗ · pubmed ↗
- 3Xiong J, Zhao W-L. Advances in multiple omics of natural-killer/T cell lymphoma. J Hematol Oncol. 2018;11(1):134. doi:10.1186/s 13045-018-0678-1; 30514323 PMC 6280527 · doi ↗ · pubmed ↗
- 4Fox CP, Civallero M, Ko Y-H, Manni M, Skrypets T, Pileri S, et al. Survival outcomes of patients with extranodal natural-killer T-cell lymphoma: a prospective cohort study from the international T-cell Project. Lancet Haematol. 2020;7(4):e 284–94. doi:10.1016/S 2352-3026(19)30283-2; 32105608 · doi ↗ · pubmed ↗
- 5Yan Z, Yao S, Wang Z, Zhou W, Yao Z, Liu Y. Treatment of extranodal NK/T-cell lymphoma: from past to future. Front Immunol. 2023;14:1088685. doi:10.3389/fimmu.2023.1088685; 36825002 PMC 9941192 · doi ↗ · pubmed ↗
- 6Zhong H, Cheng S, Zhang X, Xu B, Chen J, Jiang X, et al. Etoposide, dexamethasone, and pegaspargase with sandwiched radiotherapy in early-stage natural killer/T-cell lymphoma: a randomized phase III study. Innovation. 2023;4(3):100426. doi:10.1016/j.xinn.2023.100426; 37181228 PMC 10173773 · doi ↗ · pubmed ↗
- 7Yamaguchi M, Suzuki R, Oguchi M. Advances in the treatment of extranodal NK/T-cell lymphoma, nasal type. Blood. 2018;131(23):2528–40. doi:10.1182/blood-2017-12-791418; 29602763 · doi ↗ · pubmed ↗
- 8Li X, Cui Y, Sun Z, Zhang L, Li L, Wang X, et al. DDGP versus SMILE in newly diagnosed advanced natural killer/T-cell lymphoma: a randomized controlled, multicenter, open-label study in China. Clin Cancer Res. 2016;22(21):5223–8. doi:10.1158/1078-0432.CCR-16-0153; 27060152 · doi ↗ · pubmed ↗