Urinary Tract Infection Caused by Gardnerella vaginalis in a Male Patient With Renal Allograft Transplant
Wei-Shin Lu, Michael Kleman, Vaishnavi Aradhyula, Dinkar Kaw, Caleb T Spencer

TL;DR
A male kidney transplant patient developed a urinary tract infection caused by Gardnerella vaginalis, which was successfully treated with metronidazole.
Contribution
This case report adds to the limited literature on Gardnerella vaginalis infections in renal transplant patients.
Findings
Urine cultures confirmed Gardnerella vaginalis as the causative agent of the infection.
The patient improved with metronidazole monotherapy after initial broad-spectrum antibiotic use.
This case emphasizes the need to consider G. vaginalis in renal transplant patients with urinary symptoms.
Abstract
We present a case of a male patient with a history of renal allograft transplant four years prior to admission who presented with acute kidney injury. There were initial concerns for acute transplant rejection due to elevated creatinine. Urine cultures were positive for Gardnerella vaginalis. Renal biopsy results were concerning for chronic pyelonephritis. The patient developed hypertension, fever, and hematuria during the hospital course. He was initially treated with metronidazole, vancomycin, and cefepime. Broad-spectrum antibiotics were quickly discontinued, and the patient improved with metronidazole monotherapy. Patients with a history of renal transplants are often immunocompromised and at risk of infection. The few reported cases primarily involve urinary tract infections. There are scarce reports in the literature of G. vaginalis infection in patients with renal allograft…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
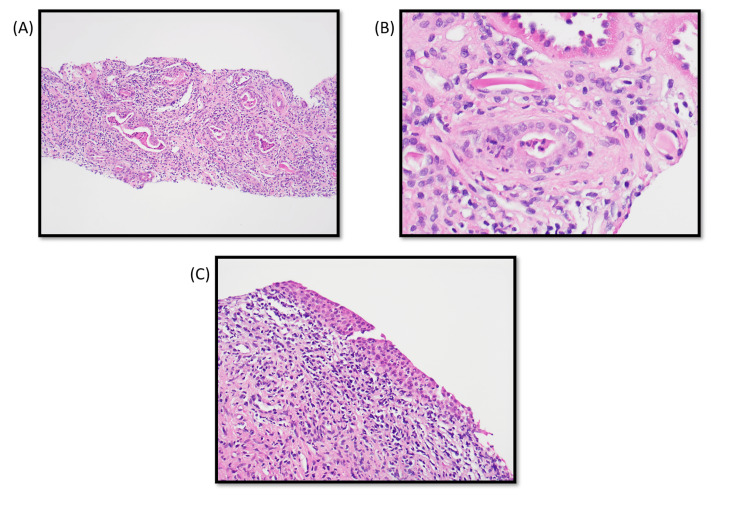 Figure 1
Figure 1| Parameters | Patient values | Reference ranges |
| Urine culture | 50,000-100,000 CFU/mL | - |
| BK virus | Not detected | - |
| Cytomegalovirus | Not detected | - |
| Donor-specific antibody | Not detected | - |
| Donor-derived cell-free DNA | 19 cp/mL | <78 cp/mL: decreased risk for rejection |
| Blood urea nitrogen | 109 mg/dL | 7-25 mg/dL |
| Creatinine | 10.64 mg/dL | 0.7-1.3 mg/dL |
| Aspartate aminotransferase | 5 U/L | 13-39 U/L |
| Alanine aminotransferase | 13 U/L | 7-52 U/L |
| Alkaline phosphatase | 47 U/L | 34-104 U/L |
| Bilirubin | 0.3 mg/dL | 0.3-1 mg/dL |
| eGFR | 5.5 mL/min/1.73 m2 | >60.0 mL/min/1.73 m2 |
| Variables | Values | Reference ranges |
| Red blood cells, urine | >100 | None seen/HPF |
| White blood cells, urine | 11-20 | None seen/HPF |
| Absolute neutrophil count | 26.5 103/µL | 1.6-7.6 103/µL |
| Blood urea nitrogen | 100 mg/dL | 7-25 mg/dL |
| Creatinine | 11.37 mg/dL | 0.7-1.3 mg/dL |
| Aspartate aminotransferase | 6 U/L | 13-39 U/L |
| Alanine aminotransferase | 9 U/L | 7-52 U/L |
| Alkaline phosphatase | 46 U/L | 34-104 U/L |
| eGFR | 5.1 mL/min/1.73 m2 | >60.0 mL/min/1.73 m2 |
| Lactate | 1.1 mmol/L | 0.5-2.2 mmol/L |
| Variables | Values | Reference ranges |
| Blood urea nitrogen | 99 mg/dL | 7-25 mg/dL |
| Creatinine | 12.37 mg/dL | 0.7-1.3 mg/dL |
| eGFR | 4.6 mL/min/1.73 m2 | >60.0 mL/min/1.73 m2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive tract infections research · Syphilis Diagnosis and Treatment · Reproductive System and Pregnancy
Introduction
Gardnerella vaginalis is an anaerobic, Gram-variable bacillus commonly present within the normal vaginal flora in women [1,2]. Clinically, G. vaginalis is associated with polymicrobial infections as well as a common cause of bacterial vaginosis in women, a frequently described and easily treated condition [3]. However, reports have also described G. vaginalis causing severe infections beyond the genitourinary tract, namely bacteremia, septic arthritis, and pulmonary and brain abscesses [4]. Most of these cases occur in women following surgical instrumentation of the genitourinary tract [4]. However, a much rare presentation of G. vaginalis is as an infection in the urinary tract of men, with disseminated infection being even more unlikely. In most men, the presence of G. vaginalis in the urethra is insufficient to cause symptoms [1]. Complications may arise once the bacteria invade further to the prostate or bladder, which may be facilitated by urological procedures such as cystoscopy or transurethral resection of the prostate. Furthermore, in patients who are immunocompromised, such as renal transplant patients, the likelihood of dissemination and severe G. vaginalis infection becomes more likely. There is scarce literature on G. vaginalis bacteremia or bacteriuria in immunocompromised men and no clear consensus on treatment options for male patients with G. vaginalis infection. In this study, we seek to highlight the importance of screening and prompt treatment of G. vaginalis infection in immunocompromised renal transplant patients.
Case presentation
A 45-year-old male was admitted for acute kidney injury found on labs from a routine transplant follow-up. His creatinine was 10.6 mg/dL on admission compared to 4.6 mg/dL six months prior to admission. He has a medical history significant for hypertension, type 1 diabetes mellitus, obstructive sleep apnea, and end-stage renal disease secondary to diabetes mellitus, status post renal allograft transplant four years prior to admission from a deceased donor. The patient endorsed that over the past month, he had been more swollen in his bilateral extremities as well as experiencing fatigue, weakness, and decreased energy. Transplant rejection was suspected based on clinical signs and elevated creatinine. Serology labs for the BK virus, Cytomegalovirus (CMV), donor-specific antibody, donor-derived cell-free DNA (Natera Prospera), and urine studies were ordered (Table 1). Labs returned negative except for urine cultures that grew 50,000-100,000 CFU/mL Gardnerella vaginalis and confirmed through matrix-assisted laser desorption/ionization-time of flight (MALDI-TOF) mass spectrometry. The patient states that he has not been sexually active with his wife for several months due to erectile dysfunction. He denies dysuria or increased urinary frequency. His diabetes mellitus is well-controlled with insulin.
A renal biopsy was performed and showed abundant chronic inflammation in the fibrotic areas of the interstitium (Figures 1A-1C). Rare areas also showed neutrophilic interstitial inflammation and tubular neutrophilic casts. Moreover, there was acute inflammation involving a calyceal urothelial lining. The findings were concerning for chronic pyelonephritis.
Histopathology images of renal biopsy.(A) Low power view showing interstitial fibrosis with inflammation and dilated tubules containing granular and neutrophilic casts. (B) Neutrophilic tubular cast and neutrophilic tubulitis. (C) Acutely inflamed urothelial lining of a calyx.
Following the renal biopsy procedure, the patient developed hypertension, tachycardia, fever, and hematuria. The patient also reported dysuria and difficulty urinating. Labs showed elevated creatinine and an increased absolute neutrophil count (Table 2).
Due to suspicion of an infectious process and concern for prostatitis, he received a dose of vancomycin 2000 mg and was started on intravenous (IV) cefepime 1 g every 12 hours as well as metronidazole 500 mg two times a day. The patient's symptomatic episode resolved the next day, and he remained hemodynamically stable. Subsequent blood cultures were negative for infection. Therefore, broad-spectrum antibiotics were discontinued, and the patient continued to improve with metronidazole monotherapy with a total planned duration of four weeks. Repeat urine culture tests were negative. The patient requested to be discharged from the facility. The patient's creatinine level remained high at 12.37 mg/dL (Table 3).
After consultation for future permanent catheter placement, follow-up for renal function test, follow-up for dialysis, and continued metronidazole therapy for G. vaginalis, the patient was discharged home.
Discussion
Gardnerella vaginalis infection is rarely found in men. The prevalence of G. vaginalis in both asymptomatic and symptomatic men is debatable, with many studies ranging between 7% and 14% [5]. It is unclear whether colonization is mostly transient or persistent. It is likely that one method for acquiring infection in men is through sexual transmission. Dawson et al. evaluated 430 urethral cultures in men (288 heterosexual, 133 homosexual, and nine bisexual) and found that heterosexual men had a 3.2-fold higher prevalence compared to homosexual men, indicating the likelihood of transmission from female partners [6]. However, there have also been reports of G. vaginalis infection in patients who are immunocompromised, have urologic complications such as nephrolithiasis/urolithiasis or stricture, or have undergone urologic procedures such as transurethral prostatectomy and urethral stenting [7-9].
Alfraji et al. describe a man who presented with altered mental status and was subsequently found to have G. vaginalis in blood cultures [7]. They were initially treated with ceftriaxone, but after G. vaginalis was identified, ceftriaxone was discontinued, and the patient remained stable on metronidazole 500 mg three times a day for 10 days. Lagacé-Wiens et al. describes a previously healthy man who presented with flank pain [10]. Renal stones were discovered, and urine culture was identified and confirmed to reveal G. vaginalis. This patient was treated with lithotripsy and improved on ciprofloxacin. Bhatia et al. describes an immunocompromised man due to acquired immunodeficiency syndrome (AIDS) who was found to have G. vaginalis on blood cultures [4]. The patient was initially treated with ceftriaxone. However, shortly after G. vaginalis identification, management was changed to metronidazole treatment for two weeks.
Commonly, in non-pregnant females, both metronidazole and clindamycin have been shown as effective and are considered first-line antibiotic treatments against symptomatic G. vaginalis infection [11]. There are currently no treatment guidelines for G. vaginalis infection in males. In addition to treatment methods described previously, other cases of G. vaginalis infection were successfully treated with cephalosporins, fluoroquinolones, tetracyclines, and often metronidazole either alone or with combination therapy [10]. In the present case, significant bacteriuria was observed. The patient subsequently developed hypertension, tachycardia, and fever, and there was concern for sepsis. It is possible that the patient’s symptoms were due to a post-biopsy inflammatory response. However, it is worth noting that the patient symptoms immediately improved after prompt treatment with antibiotics. It is also unclear whether the symptoms of sepsis were directly caused by G. vaginalis. Notably, blood cultures returned negative for infection. However, no other organism was identified to have likely caused these symptoms on blood or urine culture. It is possible that additional molecular testing would detect an organism that was not identified by standard culture. The patient was initially treated with broad-spectrum antibiotics following this episode, but after no other organisms were identified on blood cultures, antibiotic treatment was narrowed down to only metronidazole. Treatment for this immunocompromised patient was considered based on previous reports of G. vaginalis infection in men. Metronidazole was chosen as an appropriate therapy option based on prior case reports and empirical broad-spectrum coverage. The patient's condition continued to improve with metronidazole monotherapy, and subsequent urine and blood cultures were negative for organism growth. This indicates the likely importance of prompt treatment of G. vaginalis in immunocompromised men even if asymptomatic to prevent progression to potentially life-threatening complications.
Conclusions
Gardnerella vaginalis in men is rarely reported in clinical practice but is often revealed as an incidental finding or associated with clinical signs of urinary tract infection. Failure to treat infection when discovered in immunocompromised patients can lead to further complications, such as sepsis. As seen in the present case, a patient with a past medical history of renal transplant had findings of G. vaginalis bacteriuria. The present case supports the use of metronidazole, which was chosen based on prior case reports as well as being an empirical choice against G. vaginalis. While there are no treatment guidelines for G. vaginalis bacteriuria in men, our case highlights the importance of prompt treatment of G. vaginalis in immunocompromised patients to prevent further complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gardnerella vaginalis: characteristics, clinical considerations, and controversies Clin Microbiol Rev Catlin BW 21323751992149876510.1128/cmr.5.3.213PMC 358241 · doi ↗ · pubmed ↗
- 2Prevalence and distribution of Gardnerella vaginalis subgroups in women with and without bacterial vaginosis BMC Infect Dis Janulaitiene M Paliulyte V Grinceviciene S Zakareviciene J Vladisauskiene A Marcinkute A Pleckaityte M 17201710.1186/s 12879-017-2501-y PMC 546042328583109 · doi ↗ · pubmed ↗
- 3Identification, quantification and subtyping of Gardnerella vaginalis in noncultured clinical vaginal samples by quantitative PCRJ Med Microbiol Balashov SV Mordechai E Adelson ME Gygax SE 1621756320142420064010.1099/jmm.0.066407-0 · doi ↗ · pubmed ↗
- 4Not your garden-variety bacteremia: Gardnerella in an immunocompromised man Clin Infect Dis Bhatia P Temple J Kantor M 145814596620182919449310.1093/cid/cix 1054 · doi ↗ · pubmed ↗
- 5Gardnerella vaginalis in urinary tract infections, are men spared?Anaerobe Boyanova L Marteva-Proevska Y Gergova R Markovska R 72202110.1016/j.anaerobe.2021.10243834530110 · doi ↗ · pubmed ↗
- 6Male carriage of Gardnerella vaginalis Br J Vener Dis Dawson SG Ison CA Csonka G Easmon CS 243245581982698068310.1136/sti.58.4.243PMC 1046058 · doi ↗ · pubmed ↗
- 7Gardnerella vaginalis bacteremia in an elderly healthy male ID Cases Alfraji N Douedi S Akoluk A Dattadeen J Fune L Liu E 21202010.1016/j.idcr.2020.e 00807 PMC 724285932461907 · doi ↗ · pubmed ↗
- 8Gardnerella vaginalis bacteremia in an adult male Eur J Clin Microbiol Infect Dis ViláMT Onrubia P Lledos J Martinez JA Aguilera M 400401161997922848610.1007/BF 01726374 · doi ↗ · pubmed ↗