A Case of Diffuse B-Cell Lymphoma Presenting as a Rash on the Chest and Abdomen
Saurabh Dubey, Ashraf Sliem, Mohamed Akil, Nasir Gondal, Anjali Bakshi

TL;DR
A rare case of lymphoma presented as a rash on the chest and abdomen, complicating the diagnosis during sepsis treatment.
Contribution
Highlights a rare presentation of DLBCL as a rash in unusual locations during sepsis treatment.
Findings
DLBCL presented as a rash on the upper chest, shoulder, and abdomen.
The rash developed while the patient was being treated for sepsis.
The case was complicated by the possibility of a drug-induced rash.
Abstract
Diffuse large B-cell lymphoma (DLBCL) can present with skin manifestations either as a primary cutaneous DLBCL or as systemic DLBCL with cutaneous manifestations. The majority of cutaneous cases present with erythematous nodules on the legs, most commonly the lower legs. DLBCL presenting at a cutaneous site can be mistaken for cellulitis, a chronic venous ulcer, or psoriasis. Here, we present a case of DLBCL manifesting as a rash on the upper chest, shoulder, and abdomen. The case is notable in the fact that the rash developed while the patient was hospitalized and being treated for sepsis, with a drug-induced rash being a confounding diagnosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
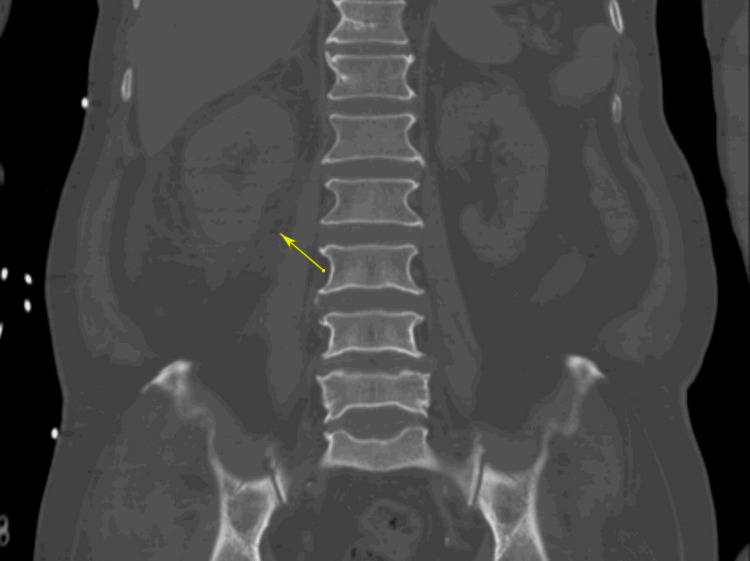 Figure 1
Figure 1 Figure 2
Figure 2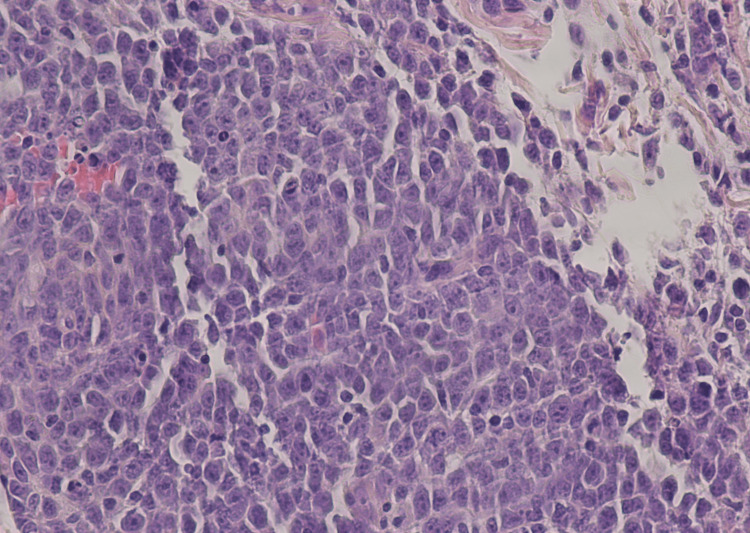 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphoma Diagnosis and Treatment · CNS Lymphoma Diagnosis and Treatment · Cutaneous lymphoproliferative disorders research
Introduction
Diffuse large B-cell lymphoma (DLBCL) is a malignant neoplasm arising from mature B cells. DLBCL accounts for 28% of all lymphoid neoplasms, with 27,000 cases occurring in the United States every year [1].
Patients typically present with rapidly expanding nodal masses; however, approximately 40% of cases present with extranodal involvement, of which approximately half present with Stage 1 disease [1]. Primary cutaneous B-cell lymphomas are defined as malignant B-cell proliferations presenting with cutaneous involvement alone and no evidence of extracutaneous manifestations when complete staging has been performed [1].
The most common extranodal site of DLBCL is the gastrointestinal tract, with the skin being the second most common [1-3]. Skin involvement at presentation can be in the form of plaques, papules, nodules, or ulcers [4]. Cases of DLBCL presenting on sites such as the trunk, shoulder, neck, or scalp are rare, and few have been described in the literature [3-5].
Case presentation
The patient was a 72-year-old male of South Asian descent who presented from home with respiratory distress and hypotension to the emergency room (ER) of Flushing Hospital Medical Center. The patient had to be intubated in the ER due to respiratory distress and was then admitted to the Medical Intensive Care Unit. Investigative workup was also remarkable for a computed axial tomography (CAT) scan of the abdomen without contrast that showed perinephric inflammation near the right kidney suggestive of pyelonephritis (Figure 1), and he was treated with cefepime empirically for sepsis thought to be secondary to pyelonephritis. The diagnosis of sepsis was made as the patient met systemic inflammatory response syndrome (SIRS) criteria with an elevated leukocyte count of 22,000 and a temperature of 102.1°F on admission. Blood cultures grew extended-spectrum beta-lactamase-producing (ESBL) Escherichia coli, so the patient was switched from cefepime to meropenem. A CAT scan of the chest was also done, which showed shotty mediastinal lymphadenopathy but did not show any masses or otherwise clinically significant findings. The patient later had a drop in his hemoglobin, for which a CT angiogram of the abdomen and pelvis was done to rule out gastrointestinal bleeding, which was significant only for urinary bladder wall thickening suggestive of cystitis. This scan did not show any signs of bleeding or any masses or lymph nodes suspicious of malignancy.
Coronal section of patient's CT scan of the abdomen and pelvis showing fat stranding around the right kidney (yellow arrow)
Ten days after he initially presented to the ER, the patient began to develop erythematous nodular skin lesions on the upper chest, shoulder, and abdomen. At the time, the most likely cause of the skin lesions was thought to be an atypical drug reaction. A photograph of the rash is included in Figure 2.
Rash (upper right chest)
However, because of the characteristics of the rash, which was atypical for a drug reaction, a skin punch biopsy was done to confirm the diagnosis. By this time, the patient had considerably improved and was discharged to follow-up on an outpatient basis regarding the results of the skin biopsy.
Histology of the skin punch biopsy was done and showed a skin specimen with highly atypical large cell infiltrate, with lymphocytes having a blastic appearance in the 15- to 20-micron range (Figure 3). The lymphocytic cells show scant basophilic cytoplasm, increased nucleus/cytoplasmic ratio, open chromatin, and prominent nucleoli. Large cells with immunoblastic features predominating over centroblasts were seen. Immunohistochemistry was done and was read as showing lymphomatous cells positive for CD20, MUM1, Ki-67, CD43, and BCL2. Interpretation based on histology and immunohistochemistry was determined as diffuse large B-cell lymphoma, immunoblastic (ABC-like). Fluorescence in situ hybridization (FISH) hybridization was done, which showed no evidence of myelocytomatosis oncogene (MYC) rearrangement, BCL2-IGH gene rearrangement, or BCL6 breakpoint translocation. The patient passed away before further workup or treatment could be done.
Histopathology of the skin punch biopsy from the patient's chest, H&E stain, showing highly atypical large cell infiltrate, with lymphocytes having a blastic appearanceH&E: Hematoxylin and eosin
Discussion
Cutaneous manifestations of diffuse large B-cell lymphomas are rare, and they are initially frequently confused with other possible etiologies, including cellulitis or venous stasis ulcers. Our patient presented with a nodular erythematous rash, which is not typical for DLBCL.
Initially, the rash was suspected to be possibly drug-induced or infectious in etiology, given it was closely associated with antibiotic use and sepsis. However, the erythematous nodular nature of the rash was not consistent with a typical drug-induced rash, so further workup via skin biopsy was done, revealing the diagnosis. Differentials other than atypical drug rash at the time included atypical bug bites and cutaneous pseudolymphoma.
Computed tomography (CT) head, CT angiogram of the abdomen, and CT chest without contrast showed no signs of systemic disease or alternative primary lesion; as such, the diagnosis of primary cutaneous DBCL was made in this case.
Conclusions
Our patient presented with a rash that was initially thought to be a side effect of antibiotic therapy (the patient had very recently received cefepime and meropenem), and because the patient had no primary lesions seen on radiological imaging prior to this, the possibility of the rash being due to a lymphoma was not considered at the time. However, because the features of the rash were not typical of that of a usual drug-induced rash, the decision was made to request a skin biopsy. This case demonstrates the need to keep a broad differential in patients who present with atypical rash and the importance of histological diagnosis via skin biopsy in confirming the diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001 Blood Morton LM Wang SS Devesa SS 2652761072006 https://ashpublications.org/blood/article/107/1/265/21762/Lymphoma-incidence-patterns-by-WHO-subtype-in-the 1615094010.1182/blood-2005-06-2508 PMC 1895348 · doi ↗ · pubmed ↗
- 2Primary subcutaneous B-cell lymphoma: case report and literature review Acta Derm Venereol Alaibac M Bordignon M Pennelli N 1511542008 https://openurl.ebsco.com/EPDB%3Agcd%3A 3%3A 7563331/detailv 2?sid=ebsco%3Aplink%3Ascholar&id=ebsco%3Agcd%3A 31967570&crl=c&link_origin=scholar.google.com 10.2340/00015555-037318311443 · doi ↗ · pubmed ↗
- 3Diffuse large B-cell lymphoma: clinical implications of extranodal versus nodal presentation--a population-based study of 1575 cases Br J Haematol Møller MB Pedersen NT Christensen BE 1511591242004 https://openurl.ebsco.com/EPDB%3Agcd%3A 3%3A 7563331/detailv 2?sid=ebsco%3Aplink%3Ascholar&id=ebsco%3Agcd%3A 31967570&crl=c&link_origin=scholar.google.com 1468702410.1046/j.1365-2141.2003.04749.x · doi ↗ · pubmed ↗
- 4Cutaneous involvement in diffuse large B cell lymphoma at presentation: report of two rare cases and literature review J Egypt Natl Canc Inst Kilaru S Panda SS Mishra S 25332021 https://doi.org/10.1186/s 43046-021-00085-13451454410.1186/s 43046-021-00085-1 · doi ↗ · pubmed ↗
- 5Primary cutaneous B-cell lymphomas: case report of two cases Indian J Dermatol Mishra S Shelly D Vinu BKV Bharadwaj R 6622017 https://journals.lww.com/ijd/Pages/default.aspx 10.4103/ijd.IJD_83_17PMC 572432729263552 · doi ↗ · pubmed ↗