Pediatric epididymal schistosomiasis, challenging diagnosis, and implications
Juliana Arenas Hoyos, Jeff Lawrence Pugach, Lynne M. Eger, Sandy Cope-Yokoyama, Shane F. Batie

TL;DR
This paper reports the first case of epididymal schistosomiasis in a U.S. pediatric patient, highlighting diagnostic challenges and the need for histology and thorough patient history.
Contribution
The first documented case of pediatric epididymal schistosomiasis in the United States.
Findings
Pediatric epididymal schistosomiasis is rare and requires histologic confirmation for diagnosis.
A detailed patient history is crucial to identify potential exposure to endemic regions.
Follow-up data on systemic sequelae in such cases remains limited.
Abstract
Schistosomiasis is a parasitic infection that may be difficult to diagnose in non-endemic regions and may manifest with epididymal involvement. Testicular schistosomiasis remains a rare disease. The diagnosis is based on clinical suspicion due to a low degree of specificity when it comes to laboratory tests and imaging studies. Treatment mainstays are anthelminthic medication and excision. We present the first report of epididymal schistosomiasis in a pediatric patient in the United States. Patients require a definitive histologic diagnosis. It is helpful to obtain a thorough history to elucidate exposure to endemic areas as part of assessment and treatment. •Schistosomiasis (SM) is rare parasitic infection that can present rarely as a pseudotumor of the testes or epididymis.•Histology is needed for diagnosis.•Organ sparing surgery may be considered if no involvement is clinically…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1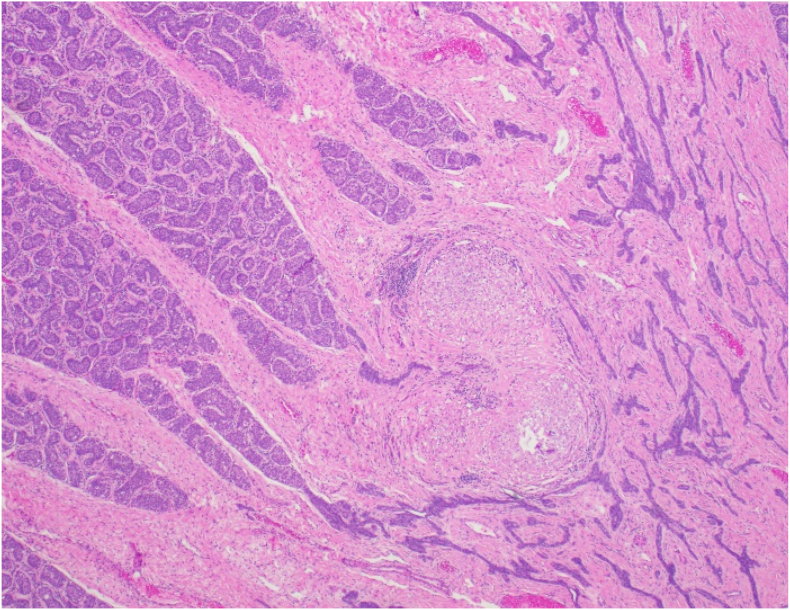 Figure 2
Figure 2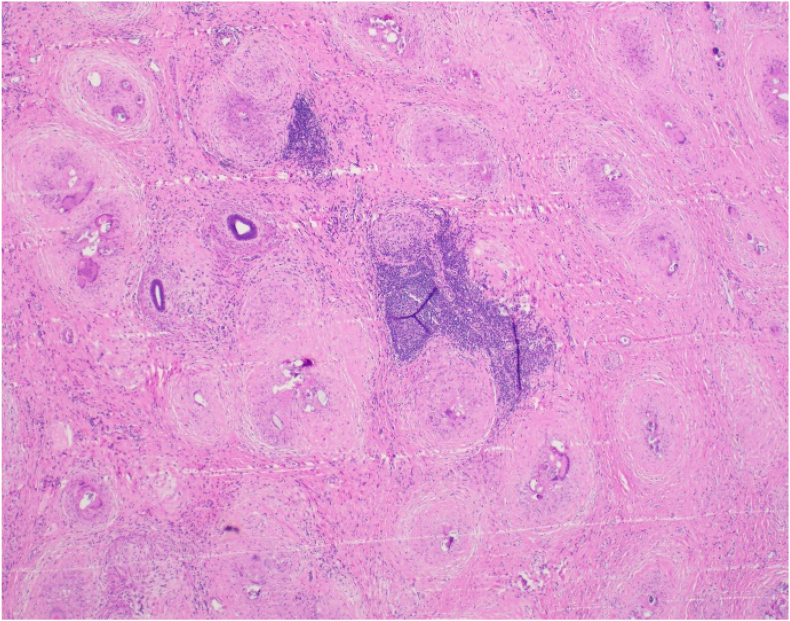 Figure 3
Figure 3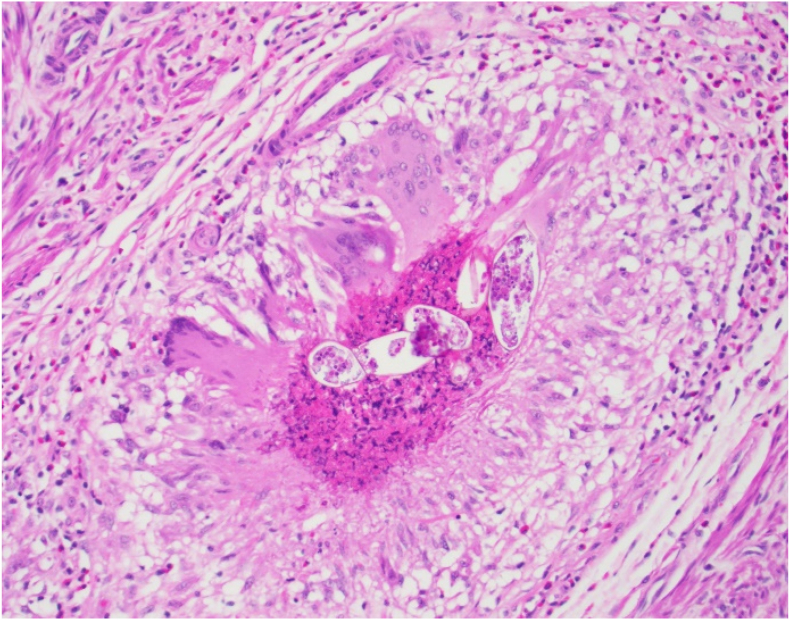 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Helminth infection and control · Parasite Biology and Host Interactions
Introduction
1
Schistosomiasis (SM) is a parasitic infection that occurs primarily in endemic areas, in communities with inadequate sanitation and limited access to clean water. Genitourinary and bladder SM has been reported in the literature as a risk factor for squamous cell bladder cancer.1 As a chronic immune-mediated disease, urogenital SM can result in symptoms such as hematuria, although not all cases exhibit this symptom.
Few cases of epididymal SM have been reported in the pediatric population.2 This case is the first reported case of pediatric schistosomiasis involving the epididymis in North America.
Case presentation
2
A 10-year-old boy, with no past medical history, was noted by mother to have a right testicular mass. The family denied having noticed the swelling before that time. He was brought to the Emergency department for evaluation 10 days later. He denied pain, fever or urinary tract symptoms. He had no history of hematuria.
On physical examination, there was an enlarged right hemiscrotum and the right epididymis had a hard mass. The right testicle was palpable separate from this mass, slightly larger than left testicle and minimally tender to palpation. There were no skin changes. The left testicle was normal in the scrotum.
While in the ED, testicular ultrasound showed a hypervascular right 2.9 x 1.8 × 3.4 cm epididymal mass and mild thickening of the right hemiscrotal wall. (Fig. 1).Fig. 1. Ultrasound Findings, Epididymal mass with mixed echogenicity and hypervascularity on Doppler.Fig. 1
Laboratory investigations indicated leukocytosis (Total white blood cell count:17 × 103/ml) with normal eosinophilic count, while urinalysis revealed hematuria (3–6 red blood cells (RBCs)/high-power field) and pyuria (20–25 white blood cells (WBCs)/high-power field). In addition to supportive care, intravenous antibiotics (Cefepime 1 g every 12 hours) were administered. Tumoral serum markers (AFP, BHCG) were obtained and resulted normal, mildly elevated LDH (279 U/L, Normal range 114–237 U/L).
He underwent radical right inguinal orchiectomy. Findings were remarkable for an enlarged firm testicle and epididymis. Scrotal wall was intact. Frozen section was sent, documenting a diffuse granulomatous inflammation of the epididymis, with organisms worrisome for parasite infection.
The radical orchiectomy specimen showed granulomatous inflammation diffusely involving the epididymis, other excretory ducts, paratesticular fibrovascular tissue, cross sections of the connective tissue of the spermatic cord (including the cord margin section), and focally the rete testis. (Fig. 2). Some of the granulomas contained central necrosis, and there were patchy areas of dense eosinophilic inflammation (Fig. 3). There were abundant parasitic organisms (Eggs/Viable eggs) with morphology consistent with Schistosoma species (Fig. 4). The organisms do not involve seminiferous tubules in the examined sections; the tubules demonstrate typical prepubertal morphology with germ cells present. GMS and AFB special stains are negative. With this pathology there was a confirmed diagnosis of Active Schistosomiasis, likely S. haematobium, and was confined to the specimen.Fig. 2. Microscopic examination, Low power view of the seminiferous tubules and rete testis. Granulomatous inflammation and organisms in center, focal involvement of rete testis. H&E, 40xFig. 2Fig. 3Low power view of epididymis, showing few residual ducts; most are obliterated by granulomatous inflammation and organisms.Fig. 3. Fig. 4High power view of organisms (including terminal spine), and surrounding granulomatous inflammation. H&E, 200xFig. 4
He was referred to Pediatric Infectious Diseases clinic, history confirmed that family had lived in Sudan for 2 years, while there, the family spent one month in Malawi in 2022. Parents and their four children also visited the tourist area of Salima, and swam in a river adjacent to Salima The nearby Lake Malawi and the rivers in the vicinity are known to harbor Schistosomiasis.
Further testing included negative urine ova and parasite screen, and normal urinalysis with no hematuria. Sonographic evaluation of the kidneys and bladder was performed, with no abnormalities. Schistosoma antibody was positive.
The patient was then prescribed praziquantel 20 mg/kg BID x 1 day (900 mg po BID). Centers for Disease Control and Prevention (CDC) Parasitology was consulted and recommended treatment with praziquantel, and that the other family members all be evaluated, since all swam in Malawi. He was seen for follow up 3 months later and was doing well without extratesticular pathology. His two brothers also had positive Schistosoma antibodies, negative urine O&P, and normal urinalyses. They were also treated with praziquantel. A younger sister had negative screening and was not treated. Parents were encouraged to see their physicians for testing for Schistosomiasis.
Discussion
3
The Schistosoma genus contains five species that infect humans, of which S. mansoni and S. haematobium are the most common.3 Consensus on the definitions of clinical aspects of schistosomiasis in migrants and travelers, including acute or chronic; possible, probable, or confirmed; active; and complicated schistosomiasis was described in 2024.3 Recent reports had described and specified the current endemic areas for Schistosomiasis in Sub-Saharan Africa, and initiatives to eradication.4 The World Health Organization reported that 229 million people were affected by schistosomiasis in 2015, with more than 90 % of them living in sub-Saharan Africa.5
The urinary bladder and the intestines are the most frequently affected organs. The diagnosis of schistosomiasis is often made by incidental histological findings. Radiological and clinical characteristics resemble the changes caused by tuberculosis in the urinary tract.6 As part of the differential diagnoses, prepubertal epididymal masses as epididymal rhabdomyosarcoma should be considered.
Primary schistosomiasis of the testis and epididymis is believed to be caused by the migration of pulmonary larvae into the venous system. As Schistosoma matures in the genitourinary venous plexus, it excretes eggs that cause granulomatous inflammation, resulting in the development of the disease.7 The rarity of the primary testicular and epididymal SM is attributed to the narrowness of the veins of the rete testis8
The pathologic changes in the urinary tract caused by schistosomiasis are more common in chronic infections than in acute infections. The development of these changes results from the deposition of perivascular eggs, which induces chronic inflammatory lesions, granulomas, and fibrosis as a result.9
The prostate and seminal vesicles have been found to have Schistosomal infection at autopsy of male cadavers in endemic regions. Schistosomiasis should be considered when there are calcifications in those organs, and in the setting of chronic prostatitis and vesiculitis, particularly in the appropriate epidemiologic setting.4
Schistosomiasis should be considered as a possible cause of acute epididymo-orchitis in patients living in or with recent travel history to endemic areas. There have been few published reports of primary acute testicular or epididymal Schistosomiasis (Table 1). There has been no publication of cases in North America.2^,^10, 11, 12, 13, 14, 15, 16Table 1. Cases published in the literature.Table 1. Author, YearCountryNAge at presentation (years)SymptomsAssessmentManagementJoshi, 196710Sierra Leone110Painless right testicular massUA: + SM haematobium eggsRadical Orchiectomy and treatment for SMRambau, 201111Tanzania19Left scrotal pain and swellingUA: (−)Orchiectomy + PraziquantelEkenze, 201512Nigeria113Left scrotal swelling and hematuriaUA: + SM haematobium eggs USRadical orchiectomy + PraziquantelAlves,201613Brazil1NSRight scrotal swellingNegative tumoral markers, US, MRIOrchiectomyOguntunde,202014Nigeria19Painless right scrotal swellingPhysical Exam.Inguinal exploration, biopsy and PraziquantelAhmed, 202215Yemen115Left testicular swellingUSScrotal orchiectomy + Praziquantel.Ukekwe, 20232Nigeria37–14Scrotal swellingPhysical exam, UA (−)Orchiectomy or biopsy + PraziquantelOur caseNorth America18Progressive right scrotal swellingUA: (−), Tumoral markers, USRadical orchiectomy + Praziquantel, Extension to contacts.Total–10Me: 10, Ave: 10.–––
A comprehensive review published in 2022,10 addressed all the cases to that date of testicular and paratesticular involvement. There was a total of 21 reports for the adult and pediatric population. The median age at presentation was 27 years (IQR 14.5–37.5), however some cases of pediatric presentation are included.
Considering the extent of involvement in most of the cases, including extension to the spermatic cord, inguinal radical orchiectomy is the most suitable approach. Testicular sparing surgery and epididymectomy could be considered, however there are no publications regarding these approaches.
Specific bladder cancer and squamous genitourinary malignancies screening should be considered in these cases. In the absence of hematuria, the evidence regarding screenings squamous bladder cancer, is uncertain.
The presence of a small number of cases in non-endemic areas suggests a need to improve understanding of the presentation and management of this disease, considering the increase in cases due to migration.
Conclusions
4
Epididymal schistosomiasis is a rare manifestation of this parasitic disease. We should consider further clinical suspicion in the event of epidemiological contact. In this report, we present a rare presentation of a disease that was considered anecdotic, because of efforts to eradicate contamination of waters and to improve sanitation.
CRediT authorship contribution statement
Juliana Arenas Hoyos: Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. Jeff Lawrence Pugach: Data curation, Formal analysis, Resources, Writing – original draft, Writing – review & editing. Lynne M. Eger: Data curation, Writing – review & editing. Sandy Cope-Yokoyama: Data curation, Formal analysis, Validation, Visualization, Writing – review & editing. Shane F. Batie: Conceptualization, Data curation, Formal analysis, Investigation, Resources, Writing – review & editing.
Ethical approval
Not required. Informed consent was obtained from all individual participants included in the study.
Disclosures
None.
Funding
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jubber I.Ong S.Bukavina L.Epidemiology of bladder cancer in 2023: a systematic review of risk factors Eur Urol 842202317619010.1016/j.eururo.2023.03.029Elsevier B.V 37198015 · doi ↗ · pubmed ↗
- 2Ukekwe F.Testicular Schistomiasis: A Clinico-Pathological Presentation of Three Pediatric Cases and Review of Literature 2023 Anals of Clinical and Biomedical Research
- 3Tamarozzi F.Mazzi C.Antinori S.Consensus definitions in imported human schistosomiasis: a Geo Sentinel and Trop Net Delphi study The Lancet Infectious Diseases 2024 Elsevier Ltd 10.1016/S 1473-3099(24)00080-X 38467128 · doi ↗ · pubmed ↗
- 4Kokaliaris C.Garba A.Matuska M.Effect of preventive chemotherapy with praziquantel on schistosomiasis among school-aged children in sub-Saharan Africa: a spatiotemporal modelling study Lancet Infect Dis 221202213614910.1016/S 1473-3099(21)00090-634863336 PMC 8695385 · doi ↗ · pubmed ↗
- 5WHO Schistosomiasis and soil-transmitted helminthiases: numbers of people treated in 2018 Wkly Epidemiol Rec 942018601612
- 6Shebel H.M.Elsayes K.M.Abou El Atta H.M.Elguindy Y.M.El-Diasty T.A.Genitourinary schistosomiasis: life cycle and radiologic-pathologic findings Radiographics 32420121031104610.1148/rg.32411516222786992 · doi ↗ · pubmed ↗
- 7Osakunor D.Paediatric schistosomiasis: what we know and what we need to know P Lo S Neglected Trop Dis 1222018 e 000614410.1371/journal.pntd.0006144 PMC 580516229420537 · doi ↗ · pubmed ↗
- 8Osakunor D.Paediatric schistosomiasis: what we know and what we need to know P Lo S Neglected Trop Dis 201810.1371/journal.pntd.0006144 PMC 580516229420537 · doi ↗ · pubmed ↗