Transmantle heterotopia associated with agenesis of the corpus callosum in a patient with Parkinson: A case report
Mattia Russel Pantalone, Stanislav Beniaminov, Daniel Martin Munoz, Francesca De Luca

TL;DR
This case report describes a patient with brain malformations and Parkinson's disease, highlighting diagnostic challenges.
Contribution
The novelty lies in presenting a rare case linking agenesis of the corpus callosum and Parkinson's in an elderly patient.
Findings
The patient exhibited agenesis of the corpus callosum and transmantle heterotopia.
The case highlights diagnostic difficulties in elderly patients with neurodegenerative diseases.
Such brain malformations may coexist with Parkinson's disease, requiring careful evaluation.
Abstract
Congenital malformations of the brain that can manifest at different ages with a wide spectrum of neurological symptoms. Although they have been described in adults, their relevance in the elderly in relation to other neurodegenerative disease is not well defined. Here we described the case of a man with the agenesis of the corpus callosum and transmantle heterotopia being diagnosed with Parkinson and we analyze the diagnostic challenges this case presented.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
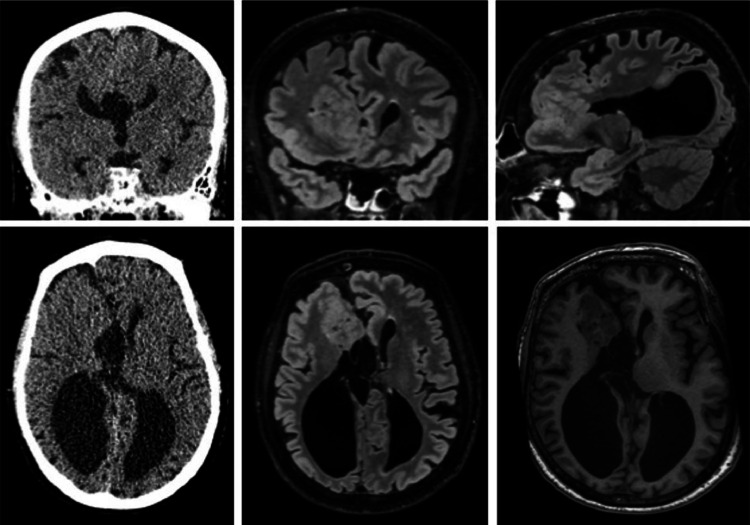 Figure 1
Figure 1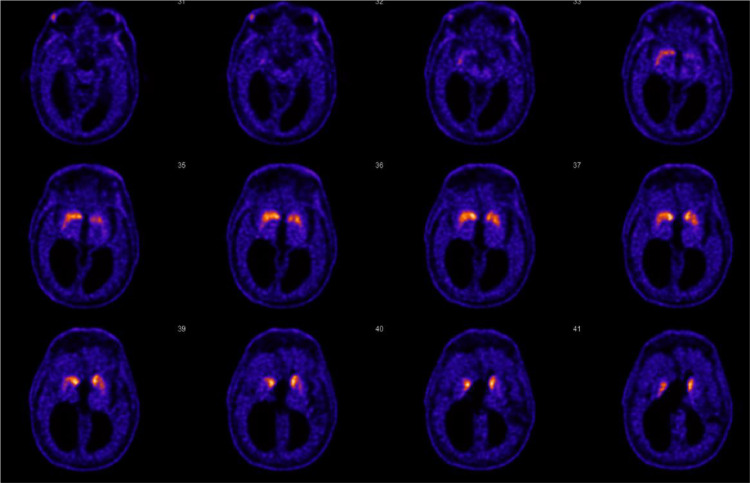 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFetal and Pediatric Neurological Disorders · Spinal Dysraphism and Malformations · Cerebrospinal fluid and hydrocephalus
Introduction
We present here the case of a 66 year old. Caucasian man referred by a family medicine doctor to the outpatient neurological clinic at Karolinska University Hospital in April 2023 with gait disturbances, back pain, and cognitive deterioration that had progressed in the previous 5 years. The patient was a retired taxi driver with a medical history of former smoking, moderate alcohol consumption, surgery for a bulging disc in the lumbar spine in the 90 s, ischemic heart disease, hypertension, hyperlipidemia, hereditary hemochromatosis with ongoing apheresis treatment, and minimal change glomerulopathy in remission.
Medications at the time of the first visit included acetylsalicylic acid, omeprazole, isosorbide mononitrate, atorvastatin, bisoprolol, chlorzoxazone, paracetamol, nitroglycerin spray. The patient´s father had been diagnosed with Parkinson's disease. No other neurological diseases were known in family history.
Current medical history
The patient had always been physically active, and according to him, his main symptom was pain in the lower back, which had become significantly worse after he played intensive golf in the autumn of 2021. His gait and balance had also gotten worse over time. He had received NSAID via a primary care physician and had been to a physiotherapist without symptomatic improvement. A magnetic resonance imaging (MRI) of the lumbar spine showed disc bulging at multiple levels with associated foraminal stenosis at the level L4-S1, and the spine surgeon had already recommended conservative treatment. According to his wife, the patient had also deteriorated in memory over time, and cognition had become quieter and less active in recent years. For that, he underwent a cognitive test in 2019, and 2 brain CT scans in 2018 and 2019, revealing GCA grade 1, MTA grade 2 bilaterally, no white matter lesions (Fazekas grade 0), and agenesis of the corpus callosum (ACC). No specific radiological signs for dementia were diagnosed at the time.
Neurological examination
The neurological examination at our hospital in 2023 revealed normal cognitive function and an appropriate fund of knowledge. No cranial nerve impairment was observed, normal facial motor skills, and no hypomimia. Grip strength was adequate bilaterally, but fine motor skills were impaired in the left hand, with reduced amplitude when moving the thumb and index finger. Normal grasset was found with good strength in both legs. No gear phenomena were observed in any of the extremities, although the foot tapping test showed reduced movement amplitude and slight start-up difficulties. The patient's gait was characterized by short steps and forward head posture. Impaired balance was observed, as the patient could not follow a straight line and showed a tendency to fall backward at the Romberg test. The patient experienced back pain while walking and lifting both legs, especially on the left side. Nontriggerable reflexes were found bilaterally in the lower extremities and no difficult-to-trigger reflexes in the arms. Babinski was negative.
Clinical management
Given the patient's neurological status, the neurological consultation at our hospital posed clinical suspicion of Parkinson's disease. The patient was offered Levodopa treatment based on his clinical symptoms, but he preferred to await further radiological investigation before initiating medical therapy.
The elective brain MRI performed in February 2023 (Fig. 1) revealed additional findings in addition to the known ACC. Indeed, transmantle heterotopia was found in the right frontal lobe, as well as pronounced atrophy of right precentral gyrus, colpocephalia, and smaller right cerebellar hemisphere compared to the normal left side. Given the overall atypical radiological picture, no specific radiological diagnosis was suggested.Fig. 1. Brain CT from 2019, soft-tissue coronal and axial images (top right and bottom right); Brain MRI from 2023, T2-FLAIR coronal, sagittal and axial images (middle and top left), and T1 axial image (bottom left), showing continuous layer of gray matter in antero-medial aspect of the right frontal lobe extending from the ventricular wall to cortex and causing bulge on the ventricular wall without intervening CSF cleft or white matter suggesting transmantle heterotopia. Colpocephaly and agenesis of the corpus callosum agenesis are also present.Fig 1
Lumbar puncture revealed no cells, no signs of blood-brain barrier damage (normal albumin) or intrathecal antibody production, negative Borrelia serology, normal neurofilament, and normal neurodegeneration markers (Bamylo 40/20, beta-Amyloid 42, Fosfo-tau, and Tau protein).
A preliminary assessment made in a collegium of neurologists at our hospital suggested that malformations in an aging person, more pronounced in the right brain hemisphere, could explain the left-sided motor symptoms. However, the gait disturbance and pain in the lower extremities could also have a polyneuropathic component. For this reason, a neurophysiological examination was performed and revealed decreased amplitudes in the left nervus tibialis but no sign of peripheral neuropathy.
A follow-up visit 6 months later revealed substantial progress in hypomimia, hypokinesia, and a clearly identifiable gear phenomenon in the right arm and right leg. Therefore, a PET-CT exam was requested to confirm the suspicion of Parkinson´s disease.
The F18-FE-PE2I striatum brain PET-CT (Fig. 2) revealed decreased uptake of the tracer bilaterally in the putamina and caudate nuclei, more pronounced on the left side. The scan confirmed signs of degeneration of the presynaptic nigrostriatal dopaminergic pathways, as in idiopathic Parkinson's disease or Parkinson-plus syndrome with left-sided predominance.Fig. 2F18-FE-PE2I striatum brain PET-CT with signs of degeneration of the presynaptic nigrostriatal dopaminergic pathways were described, as in idiopathic Parkinson's disease or Parkinson-plus syndrome with left-sided predominance.Fig 2
Based on the clinical and radiological image, therapy with Levodopa and dopamine agonist pramipexole was initiated, and the patient experienced an improvement in initiative and motor function but even some side effects such as minor hallucinations.
Discussion and conclusion
ACC is characterized by complete or partial absent corpus callosum resulting from an insult during the gestation [1]. ACC may be isolated or associated with hundreds of other genetic anomalies, but also environmental factors, such as infections, maternal alcohol consumption or phenylketonuria [2,3]. ACC in children can be asymptomatic or manifest with intellectual disability, seizures [4], poor sleep quality [5], communication impairment [6].
In adults ACC has been linked to significant deficiencies in the conceptual, social, and practical aspects of adaptive behavior [7]. The relevance of ACC in the elderly is not defined but studies have shown that callosal tissue loss is implicated in the development of global cognitive as well as motor impairment [8].
Radiologically, transmantle heterotopia is a rare MRI finding where the cerebral mantle extends from the cortical surface to the ventricular wall without intervening white matter or cerebrospinal fluid cleft [9]. This type of heterotopia can be asymptomatic or associated to seizure disorders, loss of motor skills, and intellectual disability [10].
Combination findings of corpus callosum agenesis and heterotopia have been described in different genetic abnormalities but their clinical relevance is yet not well defined [11].
In the case presented in this report, the patient conducted a normal and well-functioning life until his 60 s, when he started to develop gait disturbances and cognitive impairment and, finally, was diagnosed with Parkinson's disease. Interestingly, the brain malformations were more pronounced in the right brain and cerebellum hemispheres. The reduced fine motor ability in the left hand could be clinically correlated to the right-sided atrophy of the precentral gyrus although it had not been described in previous neurological examinations or noted by the patient himself.
The reduced balance and gait disturbance may have also been associated partly with the right cerebellum atrophy and back pain. During the initial clinical neurological examination in 2023, strong clinical suspicion of Parkinson's disease was posed. The anatomical malformations found by CT and MRI examinations arguably made it more difficult to exclude a role of these malformations as responsible to patient´s symptoms as differential diagnosis and pose the diagnosis of Parkinson's and contributed to the delay in Levodopa therapy.
A take-home message may be to follow the clinical presentation when deciding to begin treatment despite accidental anatomical findings. However, it is not possible to exclude a contribution of the ACC and the heterotopia in the clinical manifestation and these brain malformations possibly contributed to the relatively quick progression of symptoms despite normal dementia markers and may be relevant in the long-term prognosis and adaptive capability of the brain to a strained situation caused by diminished dopamine production.
Patient consent
Complete written informed consent was obtained from the patient for the publication of this study and accompanying images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schell-Apacik C.C.Wagner K.Bihler M.Ertl-Wagner B.Heinrich U.Klopocki E.Agenesis and dysgenesis of the corpus callosum: clinical, genetic and neuroimaging findings in a series of 41 patients Am J Med Genet A 146a 192008250125111879298410.1002/ajmg.a.32476 PMC 2774850 · doi ↗ · pubmed ↗
- 2Stoll C.Dott B.Roth M.P.Associated anomalies in cases with agenesis of the corpus callosum Am J Med Genet A 179102019210121113144490010.1002/ajmg.a.61330 · doi ↗ · pubmed ↗
- 3Hofman J.Hutny M.Sztuba K.Paprocka J.Corpus callosum agenesis: an insight into the etiology and spectrum of symptoms Brain Sci 10920206253291697810.3390/brainsci 10090625 PMC 7565833 · doi ↗ · pubmed ↗
- 4Margari L.Palumbi R.Campa M.G.Operto F.F.Buttiglione M.Craig F.Clinical manifestations in children and adolescents with corpus callosum abnormalities J Neurol 263102016193919452738364110.1007/s 00415-016-8225-x · doi ↗ · pubmed ↗
- 5Kwon A.Gu P.K.Zhang C.Davidson Ward S.L.Perez I.A.Sleep disorders in pediatric patients with agenesis of the corpus callosum J Clin Sleep Med 20102024166316673891336210.5664/jcsm.11234 PMC 11446115 · doi ↗ · pubmed ↗
- 6Moser C.Spencer-Smith M.M.Anderson P.J.Mc Ilroy A.Wood A.G.Leventer R.J.Language and communication functioning in children and adolescents with agenesis of the corpus callosum Brain Lang 255202410544810.1016/j.bandl.2024.10544839083998 · doi ↗ · pubmed ↗
- 7Miller J.S.Brown W.S.Mangum R.W.Nolty A.A.T.Paul L.K.Adaptive behavior in primary agenesis of the corpus callosum Res Dev Disabil 154202410486210.1016/j.ridd.2024.10486239454245 · doi ↗ · pubmed ↗
- 8Frederiksen K.S.Garde E.Skimminge A.Barkhof F.Scheltens P.van Straaten E.C.Corpus callosum tissue loss and development of motor and global cognitive impairment: the LADIS study Dement Geriatr Cogn Disord 32420112792862226201710.1159/000334949 · doi ↗ · pubmed ↗