Primary Intracranial Adenoid Cystic Carcinoma: A Case Report
Pralisha Maharjan, Gopi Aryal, Reena Rana

TL;DR
A rare case of primary intracranial adenoid cystic carcinoma in a 61-year-old man is reported, highlighting its presentation and treatment.
Contribution
This case report adds to the limited literature on primary intracranial adenoid cystic carcinoma, a rare and aggressive tumor.
Findings
A 61-year-old male presented with neurological symptoms due to a cerebellopontine angle mass.
Histopathological analysis confirmed the tumor as primary intracranial adenoid cystic carcinoma.
Surgical excision was performed, but the rarity of the tumor emphasizes the need for further research.
Abstract
Adenoid cystic carcinoma (ACC) is a rare slow-growing but aggressive malignant tumor arising from the epithelial cells of mucous-secreting glands. Primary intracranial ACC is one of the rarest entity. We report a case of a 61 years old male presenting with difficulty in swallowing, slurring of speech, generalized body weakness. Patient had residual right cerebellopontine angle (CPA) mass causing midline shift and fourth ventricular obstruction on MRI. Patient underwent right retrosigmoid craniotomy with excision of CPA mass. Histopathological examination confirmed the case as primary intracranial ACC.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
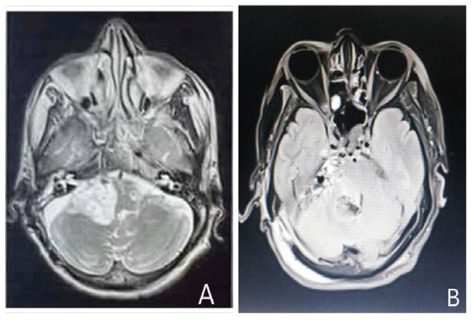 Figure 1
Figure 1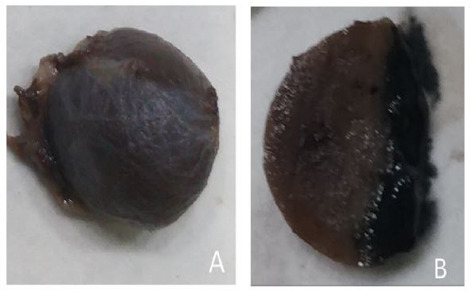 Figure 2
Figure 2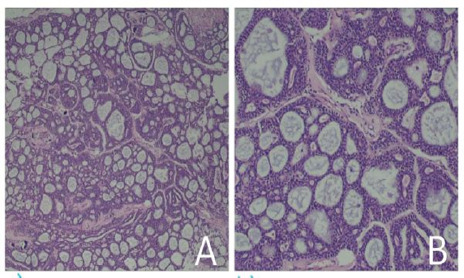 Figure 3
Figure 3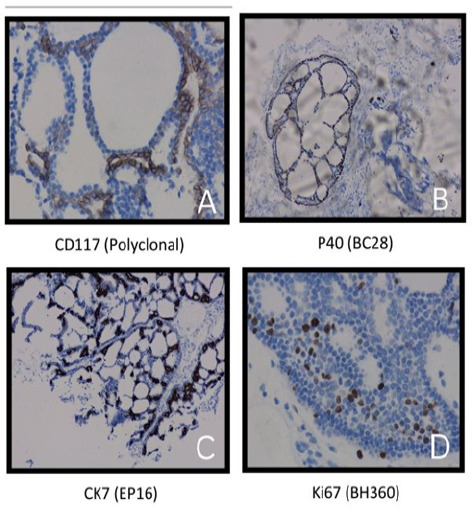 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Head and Neck Surgical Oncology · Ear and Head Tumors
INTRODUCTION
Adenoid cystic carcinoma (ACC) is a rare slow-growing but aggressive malignant tumor with potential of perineural invasion. It accounts for less than 1% of all head and neck malignancies and approximately 10% of all salivary gland neoplasms. ^1^ Primary intracranial ACC is one of the rarest entity. ACC has three main histological patterns : solid, tubular, and cribriform. Only eight cases of primary intracranial ACC have been reported till date (1990-2022). ^2,3^ Here we report a case of 61 years male diagnosed with primary intracranial ACC.
CASE
A 61 years man presented with dysphagia, slurring of speech, generalized body weakness for three months. On clinical examination, he was conscious and oriented, his vitals were stable and on other systemic examinations no abnormalities were detected . On neurological examination, higher motor function was intact but patient had right sided lower motor neuron facial palsy of grade III and right sided sensorineural hearing loss, cerebellar signs were positive on right side and had gait ataxia, gag reflex was absent and there was no motor and sensory deficits. Hematological and biochemical parameters were within normal limits. The patient had significant past history of right CPA mass for which he was operated at other medical center and histological report was suggestive of neuroenteric cyst. Repeated Magnetic Resonance Imaging (MRI) showed tumor infiltrating the nerve sheath of cranial nerves 9th , 10th and 12th on right side extending into exocranial aspect and inferiorly along pterygoid muscle, lateral wall of nasopharynx and right medial temporal region for which intervention was not done.
A. Preoperative MRI brain revealing a hyperintense lesion on T2-weighted image on axial plane measuring 4.2 cm × 4.0cm × 1.4cm. B. Postoperative MRI brain revealing heterogenous collection at tumor resection bed in right lateral aspect of posterior fossa where central component of the collection displays mixed signal.
The MRI done on 15th April, 2024 revealed right CPA mass causing midline shift and fourth ventricular obstruction (Figure 1). He underwent right retrosigmoid craniotomy with excision of CPA mass on 23th April, 2024. Peroperatively, the lesion was greyish white to greyish brown and firm.
On gross examination, the specimen appeared greyish brown with largest nodular tissue measuring 1.5cm×1.2cm (Figure 2A). Cut sections showed solid to cystic area. (Figure 2B). Remaining fragmented tissue altogether measures 2.5×2.2cm. Entire tissue submitted.
A. Gross image appeared greyish white to greyish brown nodular tissue. B. Cut section showed solid to cystic area.
Microscopic examination revealed tumor tissue predominantly composed of cribriform growth pattern with nest of tumor cells with discrete, rounded punched out gland like spaces filled with eosinophilic to basophilic material (Figure 3A). Area of tubular pattern with multiple ducts and tubules like structure are lined by small uniform cuboidal epithelium (Figure 3B). A focus of solid sheets of tumor cells (<30% solid component) noted. Infiltrating tumor nests are identified within fibrous stroma. Perineural invasion is evident. Focal areas of reactive gliosis with dilated and congested blood vessels are noted.
The tumor cells expressed CD117 positivity in luminal layer and P40 and CK7 in myoepithelial layer but was negative for S100 and Ki-67 was nearly 12% (Figure 4). With all these histological features and immunohistochemical reports, the case was finally diagnosed as intracranial ACC.
To look for the primary site of the lesion, further evaluation like chest X-ray, ultrasonography of abdomen, and whole-body MRI was performed but the primary site remained unknown so we concluded the tumor to be intracranial in origin and diagnosed it as primary intracranial ACC. Patient was managed conservatively with intravenous antibiotics and all other supportive measures. However, the patient didn't receive postoperative radiotherapy and he passed away on 18th post operative day (POD).
A. Tumor tissue predominantly composed of cribriform growth pattern with nest of tumor cells with discrete, rounded punched out gland like spaces filled with eosinophilic to basophilic material (Hematoxylin and Eosin stain x10). B. Area of tubular pattern with multiple ducts and tubules like structure are lined by small uniform cuboidal epithelium (Hematoxylin and Eosin stain x40).
A. The tumor cells expressed CD117 positivity in luminal layer. B and C. The tumor cells expressed P40 and CK7 in myoepithelial layer. D. Ki-67 was nearly 12%
DISCUSSION
ACC is a rare slow-growing but aggressive malignant tumor. More than half of ACC arises from the minor salivary glands but it can also affect the major salivary glands, paranasal sinuses, larynx, and trachea and hard palate is most commonly affected intraoral site.^4^ Though direct extension of the tumor or invasion along cranial nerves is common but primary intracranial ACC is extremely rare. Only eight cases of primary intracranial ACC have been reported till date (1990-2022) ^2,3^ where the youngest case was 34 years and the eldest was 71 years, clinical features varied from headache, epistaxis to hemianopia and left facial region numbness and most common location was cavernous sinus. Cases underwent operation, radiosurgery and radiotherapy. Among them 3 cases died after management while 2 cases were alive with disease and 3 were alive without disease.
In our case, the mass was seen in right CPA causing midline shift and fourth ventricular obstruction. Literatures have shown that the tumors arising close to the skull base may cause ocular dysmotility, and cranial nerve (CN) palsies involving IX, X, XI, and XII.^5,6^ It is thought to arise from existing bucconasal cell rests.^7^ Among the primary intracranial ACCs reported in the literature, Gasserian ganglion, middle cranial fossa, frontal lobe, cavernous sinus and posterior fossa comprise majority of locations.^8^ Similar to findings of these literatures, our case also had multiple nerve sheath tumors (right IX CN, X CN, XII CN), extending into exocranial aspect and inferiorly along pterygoid muscle, lateral wall of nasopharynx and right medial temporal region as seen on MRI.
Age of the patient, tumour site, clinical stage, histological type with or without nerve involvement are the important factors influencing prognosis however the survival at 5,10, and 20 years around 68%, 52% and 28% respectively after decompression surgery and postoperative radiotherapy.^9^ The need for early diagnosis and radical tumor resection, if possible , coupled with postoperative radiation should be emphasized so that local disease control and better long-term survival will be achieved.^10^ However, the patient didn't receive postoperative radiotherapy and he passed away on 18^th^ POD .
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chummun S Mc Lean NR Kelly CG Dawes PJ Meikle D Fellows S et al Adenoid cystic carcinoma of the head and neck.Br J Plast Surg.2001 Sep 5464768010.1054/bjps.2001.363611513507 · doi ↗ · pubmed ↗
- 2Sakata K Ono T Koga M Kikuchi J Komaki S Akiba J Primary Pituitary Adenoid Cystic Carcinoma: A Rare Salivary Gland-Like Tumor in the Sella.Head Neck Pathol.2021 Dec 1541289129810.1007/s 12105-020-01256-733398687 PMC 8633198 · doi ↗ · pubmed ↗
- 3Tsetsos N Poutoglidis A Terzakis D Epitropou I Oostra A Georgalas C Primary Intracranial Adenoid Cystic Carcinoma: Report of Three Cases.J Neurol Surg B Skull Base.2022 Jun 784432933510.1055/a-1837-682537405240 PMC 10317558 · doi ↗ · pubmed ↗
- 4Lee RH Wai KC Chan JW Ha PK Kang H Approaches to the Management of Metastatic Adenoid Cystic Carcinoma.Cancers (Basel).2022 Nov 201422569810.3390/cancers 1422569836428790 PMC 9688467 · doi ↗ · pubmed ↗
- 5Tsuyuguchi N Ohata K Goto T Haque M Hara M Intracranial Adenoid Cystic Carcinoma of Suprasellar Region.Acta Neurochir (Wien).200114377293210.1007/s 00701017005311534695 · doi ↗ · pubmed ↗
- 6Ammad Ud Din M Shaikh H Adenoid Cystic Cancer.2023 Apr 14Stat Pearls [Internet]Treasure Island (FL)Stat Pearls Publishing 2024 Jan 32491778 · pubmed ↗
- 7Jayalakshmi S Agarwal S Nachiappan PL Prasad RR Bhuthra S Sharma MC et al Intracranial Adenoid Cystic Carcinoma-- A Case Report.J Neurooncol.2000 Mar 471475010.1023/A:100615172486010930099 · doi ↗ · pubmed ↗
- 8Huang M Ma D Sun K Factors Influencing Survival Rate in Adenoid Cystic Carcinoma of the Salivary Glands.Zhonghua Kou Qiang Yi Xue Za Zhi.2000 Nov 3564303 Chinese 11780525 · pubmed ↗