Clinical aspects of human mpox cases in the global scenario: an integrative review
Ana Clara Dantas, Cyntia Leenara Bezerra-da Silva, Dase Luyza Barbosa-de Sousa Alves, Amanda Barbosa-da Silva, Hanna Priscilla da Silva-Medeiros, Allyne Fortes-Vitor

TL;DR
This paper reviews clinical aspects of human mpox cases globally, highlighting gaps in care guidance for healthcare teams.
Contribution
The study compiles scientific evidence to guide multidisciplinary and nursing care for human mpox patients.
Findings
The review identified 58 studies focusing on signs, symptoms, transmission, diagnosis, and prevention of mpox.
Few studies specifically addressed care for multidisciplinary and nursing teams.
The findings aim to improve patient management and prevent complications of MPXV infection.
Abstract
In recent years, human-to-human transmission of MPXV has been frequently reported. Despite this, there is a lack of studies with strong evidence to guide the care practice focused on cases of human mpox. To analyze scientific evidence in the literature that addresses clinical aspects related to cases of human mpox on the global scenario. Integrative review conducted using five databases: SCOPUS, Web of Science, ScienceDirect, MEDLINE/PubMed and CINAHL. The last date of database access was October 3, 2024. The selection of studies and review report followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. With a sample of 58 studies, the main findings were aspects related to signs and symptoms, transmission, diagnosis, prevention and care for the multidisciplinary and nursing teams. No studies were found that frequently…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
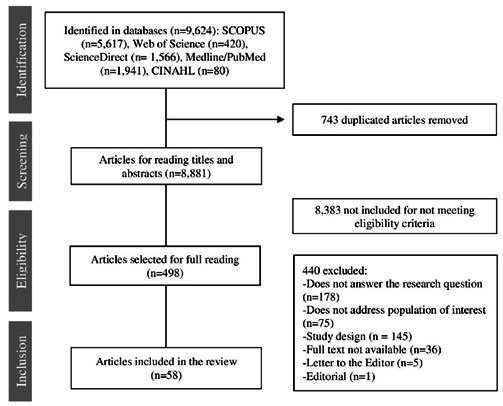 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · Bacillus and Francisella bacterial research · Rabies epidemiology and control
Introduction
Human mpox, formerly known as monkeypox, is a zoonotic disease caused by the mpox virus (MPXV). In recent years, human-to-human transmission has become more frequently reported, raising global concern about its potential for spreading1^, ^4.
The first case of human mpox in the most recent multinational outbreak was confirmed in the UK on May 6, 2022, in a man travelling from Nigeria. New cases were quickly detected in several other countries, leading the World Health Organization (WHO) to declare a Public Health Emergency of International Concern (PHEIC) on July 23, 20225^, ^6.
According to the latest report published on September 28, 2024, a total of 106,310 confirmed cases of human mpox had been reported in 123 locations worldwide, including 234 deaths. The highest number of cases was reported in the United States of America (USA) (33,812 cases), followed by Brazil (12,206 cases) and Spain (8,240 cases) 7.
Despite its current relevance, there is a lack of studies with strong evidence to guide care practice focused on cases of human mpox. This study is justified by the importance of compiling information that supports evidence-based practice on the clinical aspects of human mpox.
This study aims to analyze scientific evidence in the literature that addresses clinical aspects related to cases of human mpox in the global scenario.
Materials and Methods
Design
This is an integrative review conducted through the following stages: formulation of the research question, identification of relevant studies, selection of studies and extraction of data and, finally, presentation of a synthesis of the evidence8^, ^9. This study followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 10 guidelines. The dataset of this study was stored in the Mendeley Data11 public repository.
Formulation of the research question
The research question was formulated based on the PICO strategy (P: population - general population; I: interest - clinical aspects related to human mpox cases; C: context - world scenario). Thus, the following guiding question was delimited: What is the existing scientific evidence on the clinical aspects related to human mpox cases in the global scenario?
Identification of relevant studies
Five databases were accessed: SCOPUS, Web of Science, ScienceDirect, MEDLINE and PubMed from the National Library of Medicine and the National Institutes of Health, and Cumulative Index to Nursing and Allied Health Literature (CINAHL). The last database access was on October 3, 2024.
Regarding the inclusion criteria, we considered studies that addressed evidence on cases of human mpox in the world scenario and available in full text. In order to achieve a comprehensive survey of the literature and considering that human mpox is an old infection, whose repercussions are the focus of study worldwide, no time frame was set for publications. Editorials, letters to the editor, abstracts, case reports, case series, experience reports, non-systematic reviews and reflection articles were excluded.
For the search strategy, the descriptors indexed in the Medical Subject Headings (MeSH) were used: "Monkeypox," "Monkeypox virus" "Delivery of Health Care," "Epidemiology," and "Signs and Symptoms". Three search strategies were developed for the SCOPUS database, and were adapted to the other databases, considering their particularities (Table 1).
Table 1. Search strategies developed for SCOPUS databaseSearch strategiesALL(“Monkeypox" OR “Monkeypox virus”) AND (“Delivery of Health Care")ALL(“Monkeypox” OR “Monkeypox virus”) AND (“Epidemiology”)ALL (“Monkeypox" OR “Monkeypox virus") AND (“Signs and Symptoms")
Selection of studies and data extraction
The search was performed independently by two researchers, finding the same number of studies in each database. The publications found were stored and exported to the software Rayyan - Intelligent Systematic Review (https://rayyan.ai/). Duplicates were removed and studies were selected. The organization of the citations and reference list of this review were managed by the Mendeley reference management software.
After this process, the title and abstract of the studies found were read to analyze whether they answered ourguidingresearch question.The articlesincluded after theinitial readingweresubmitted for full reading. In order to reduce possible biases, two researchers independently performed a selection stage of studies for analysis, with a third researcher to resolve any discrepancies.
For data mapping and data extraction procedure, a structured tool was developed in Microsoft Excel 2019®, containing the following items: identification of studies, methodological aspects, items related to the clinical aspects of human mpox cases, and main conclusions of the studies.
Synthesis of evidence
An analytical framework was built for data analysis by compiling selected studies, allowing for gathering and synthesizing the main information of the articles. The results were analyzed and later synthesized descriptively with the characterization of the studies.
Regarding the level of evidence for analyzing the studies, we chose to follow the JBI guidelines, which present five levels of evidence, namely: level 1 - experimental studies; level 2 - quasi experimental studies; level 3 - analytical observational studies; level 4 - descriptive observational studies; and level 5 - expert opinions12.
Results
The database search stage yielded a total of 9,624 identified studies. After the selection process, 58 studies composed the final sample, as outlined in the flowchart shown in Figure 1.
Figure 1. Study selection diagram, according to PRISMA flowchart
Most studies were published in 2023, representing 60.34% (35) of the sample; 34.48% (20) were from Europe; 34.48% (20) had a methodological design characterized by systematic review; and 100% (56) were written in English. Table 2 shows the characteristics of the studies included in the sample detailing authors, year of publication, country, journal of publication, study design, and level of evidence. The main findings are presented in Table 3.
Table 2. Characterization of selected studiesAuthors (year)CountryJournalStudy design/LERamirez-Soto et al. (2024)13 PeruJournal of Infection and Public HealthObservational study/3.e.Ribeiro et al. (2024) 14 BrazilEpidemiology and Health Services.Descriptive study/4.bMalone et al.(2023) 15 USAInternational Journal of Environmental Research and Public Health.Systematic review, with meta- analysis/1.bHeukelom et al. (2023) 16 The NetherlandsJournal of the European Academy of Dermatology and VenereologyQuasi-experimental study/2.cWieder-Feinsod et al. (2023) 17 IsraelInternational Journal of Infectious Diseases.Retrospective Study/2.dPassini et al. (2023) 18 ItalyPathogensRetrospective Study/2.dAssiri et al. (2023) 19 Saudi ArabiaJournal of Infection and Public HealthObservational study/2.dMaldonado et al. (2023) 20 PeruInternational Society for Infectious DiseasesObservational study/2.dBrosnan et al. (2023) 21 USAEmerging Infectious DiseasesObservational study/2.dNúñez et al. (2023) 22 MexicoThe Lancet Regional Health.Observational study/2.dDeb et al. (2023) 23 IndiaJournal Pre-proofSystematic Review/3.aAbdelaal et al. (2023) 24 EgyptAsia-Pacific Journal of OphthalmologySystematic review and meta- analysis/3.bZaqout et al. (2023) 25 QatarJournal of Infection and Public HealthCohort study/3.cFink et al. (2023) 26 United KingdomThe Lancet infectious diseases.Retrospective cohort study/3.cSobral-Costas et al. (2023) 27 SpainJournal of the American Academy of DermatologyProspective cohort study/3.cMazzotta et al. (2023) 28 ItalyJournal of Medical VirologyProspective cohort study/3.cMorales et al. (2023) 29 SpainEurosurveillanceProspective cohort study/3.cZucker et al. (2023) 30 IsraelClinical Microbiology and InfectionRetrospective cohort study/3.cHerrán-Arita et al. (2023) 31 MexicoMicroorganismsCase-control study/3.dRimmer et al. (2023) 32 United KingdomInternational Journal of Infectious Diseases.Case-control study/3.dSahin Y, et al. (2023) 33 TürkiyeAnnals of the Brazilian Academy of SciencesSystematic Review/4.aChenchula et al. (2023) 34 IndiaArchives of Virology.Systematic Review/4.aHatami et al. (2023) 35 IranBiomedicines.Systematic review, with meta- analysis/4.aJaffer et al. (2023) 36 USAAmerican Journal of OtolaryngologySystematic review, with meta- analysis/4.aSharma et al. (2023) 37 IndiaInternational Journal of Emergency MedicineSystematic Review/4.aDu et al. (2023) 38 ChinaInternational Journal of Public HealthSystematic Review/4.aSimadibrata et al. (2023) 39 IndonesiaJournal of Medical VirologySystematic Review/4.aJaiswal et al. (2023) 40 USACurrent Problems in CardiologySystematic Review/4.aPourriyahi et al. (2023) 41 IranJournal of Medical VirologySystematic Review/4.aLiu et al. (2023) 42 ChinaPathogensSystematic review, with meta- analysis/4.aVelázquez-Cervantes et al. (2023) 43 MexicoClinical Journal SpanishSystematic Review/4.aKhan et al. (2023) 44 NepalMedicineSystematic Review/4.aGandhi P A, et al. (2023) 45 IndiaEClinicalMedicine.Systematic Review/4.aChaudhari S, et al. (2023) 46 USACureusSystematic Review/4.aLi et al. (2023) 47 ChinaSignal Transduction and Targeted TherapyCross-sectional study/4.bAngelo et al. (2023) 48 MulticenterThe Lancet infectious diseases.Cross-sectional study/4.bEser-Karlidag et al. (2023) 49 MulticenterNew Microbes and New InfectionsCross-sectional study/4.bWebb et al. (2022) 50 United KingdomBMJ Global HealthSystematic Review/2.aNórz et al. (2022) 51 GermanyEurosurveillanceExperimental trial/2.cHoffmann et al. (2022) 52 GermanyHIV MedicineRetrospective Study/2.dSilva et al. (2022) 53 BrazilThe Lancet Regional Health.Prospective cohort study/3.cTarín-Vicente et al. (2022) 54 SpainThe LancetCohort study/3.cAcevedo et al. (2022) 55 ChileSSRN eLibraryCase- control study/3.dMailhe M et al. (2022) 56 FranceClinical Microbiology and InfectionObservational study/3.eGarcía-Hernández L, et al. (2022) 57 SpainSpanish Journal of Public HealthRetrospective Study/3.eBunge et al. (2022) 58 USAPLOS Neglected Tropical DiseasesSystematic Review/4.aJairoun et al. (2022) 59 United Arab EmiratesJournal of Infection and Public Health.Cross-sectional study/4.bAmao et al. (2022) 60 NigeriaJournal of Public HealthCross-sectional study/4.bMartínez et al. (2022) 61 SpainEurosurveillanceCross-sectional study/4.bAntinori et al. (2022) 62 ItalyEurosurveillanceCross-sectional study/4.bPeiró-Mestres et al. (2022) 63 SpainEurosurveillanceCross-sectional study/4.bPerez Duque et al. (2022) 64 PortugalEurosurveillanceCross-sectional study/4.bRicco et al. (2022) 65 ItalyTropical Medicine and Infectious DiseaseCross-sectional study/4.bBeer et al. (2019) 66 United KingdomPlos Neglected Tropical DiseasesSystematic Review/2.aLi et al. (2017) 67 USAThe American Journal of Tropical Medicine and HygieneExperimental study/2.bNolen et al. (2015) 68 Democratic Republic of the CongoThe American Journal of Tropical Medicine and HygieneRetrospective cohort study/3.cFormenty et al. (2010) 69 USACenters for Disease Control and Prevention (CDC)Retrospective Study/4.bHuhn et al. (2005) 70 USAClinical Infectious DiseasesCase-control study/3.d**Level of evidence according to global JBI*12
Table 3. Main findings regarding the aspects of human mpox casesAspectsMain findingsSigns and symptoms•The incubation period of the MPXV is from 4 to 21 days, with a mean period of 8.5 days34^,^37^, ^49^, ^56. •Symptoms such as fever, lymphadenopathy, proctitis, oral and/or anogenital lesions, rash, headache, asthenia, myalgia, chills, malaise, fatigue and ocular complications were presented14^, ^51^, ^60^, ^61, while odynophagia and cough are less common20. •Rashes begin in the macular phase and then progress to the papular, vesicular, pustular, and crustal phases 33^, ^41^, ^51^, ^56 Transmission•It occurs mostly in males, ranging from 18 to 67 years of age, with a mean age of 35 years19^, ^20^, ^25^, ^55. •Human-to-human transmission: associated through respiratory droplets, contact with bodily fluids, environment or belongings of a contaminated patient, skin lesion of an infected person and with sexual transmission of an infected individual with lesions in the groin and genitals35^, ^58. •Animal-human transmission: direct contact with natural viral hosts or consumption of hosts, or direct contact with blood of an infected animal, body fluids or inoculation through skin mucus lesions35^, ^58. •The virus is particularly dangerous for pregnant women, children under eight years of age, and people with compromised immune systems13^, ^43^, ^66.Diagnosis•Diagnosis is preferably by reverse transcription followed by polymerase chain reaction (RT-PCR) 19^, ^52^, ^53^, ^56^, ^61. •Optimal diagnostic samples come from rash, fluid, scabs or, in some cases, a biopsy of the lesions46. •Inquire about travel and sexual history or any close contact with people exhibiting a similar rash or with suspected or confirmed varicella infection19^, ^38^, ^41. •Samples can also be tested for varicella-zoster virus (VZV) 41.Prevention•There are no vaccines specifically designed to protect against infection and disease of human mpox20. •The smallpox vaccines ACAM-2000 and MVA-BN are prophylactically recommended for people at risk of MPXV exposure33^, ^41. •The use of the smallpox vaccine Imvanex is recommended for prevention after close contact or exposure to patient with the virus33. •For all cases, including suspects, recommendations are made for home isolation under clinical and epidemiological surveillance, use of surgical masks when sharing the same location and avoiding contact with domestic animals. These measures should be maintained until the skin lesions become crusty and all crusts fall off21^, ^45^, ^57. •Healthcare professionals must wear specific Personal Protective Equipment (PPE) for droplet and contact isolation62. •Contact screening to control the spread of mpox should be done61.Treatment•There is no clinically proven specific therapy for mpox disease37^, ^62. •Treatment is primarily for symptomatic control56^, ^62. For skin lesions, topical cidofovir is a potentially relevant therapy, but with mild systemic involvement25^, ^27. •For severe cases, especially in pregnant patients, children under eight years of age or immunocompromised individuals, the use of antiviral drugs to treat smallpox was approved, such as Tecovirimat (TPOXX) 21^, ^25^, ^33.Care for the multidisciplinary team and the nursing team•Recognize early cases of MPXV infection through appropriate alert screening, isolation, and infection control protocols21^, ^45^, ^57. •Carry out case screening through active case-finding in health units20^, ^21. •Monitor possible symptoms such as fever, chills, rash and lymphadenopathy for 21 days after the last exposure37^, ^49^, ^56. •Treat symptoms according to the needs of each patient56^, ^62. •Provide support to maintain adequate water balance37. •Offer hemodynamic support, such as supplemental oxygen or other respiratory support, if necessary37. •Treat secondary bacterial infections of skin lesions, when indicated26. •Identify and treat eye infections and complications resulting from MPXV infection34^, ^56. •Offer psychosocial support to the patient and family60.
Discussion
Signs and symptoms
Regarding the MPXV incubation period, that is, the interval from infection to the onset of symptoms, most studies reported a period of 4 to 21 days, with a mean period of 8.5 days34^, ^37^, ^49^, ^55. Before the 2022 outbreak, the mean incubation period of the infection was 5 to 13 days70.
Patients typically present with symptoms such as fever, lymphadenopathy, proctitis, oral and/ or anogenital lesions, rash, headache, asthenia, myalgia, chills, malaise, fatigue and ocular complications51^, ^60^, ^61, while odynophagia and cough are less common20. Systemic symptoms are followed by the development of characteristic rashes. Generally, the rashes appear in the mouth and soon spread to the face and extremities, involving the palms of the hands and soles of the feet45. Lesions in the anogenital region, present in the anus, perianal region, scrotum and penis, were also reported in the studies16^, ^37^, ^42.
Due to the systemic symptoms that occur initially, resembling those of flu-like syndrome, the initial diagnosis may be ignored. With the manifestation of rashes near the genitals, MPXV is often diagnosed as another Sexually Transmitted Infection (STI) 70. There is a need to identify and monitor symptoms for differential diagnosis by health professionals.
Furthermore, the findings show the possibility of complications resulting from MPXV infection, such as subsequent skin infections, pneumonia, sepsis, encephalitis and corneal infection leading to potential vision loss37^, ^46. Immunocompromised individuals, pregnant women and children under eight years of age are more likely to have severe complications of the disease, with mortality rates ranging from 1 to 11%66.
Transmission
The MPXV can be transmitted from person to person, animal to animal, and animal to human. Human- to-human transmission has been associated with respiratory droplet transmission, contact with bodily fluids, contact with skin lesions of an infected person, and sexual transmission of an infected individual with groin and genital lesions. Furthermore, studies indicate that the environment or belongings of a contaminated patient, such as clothing and bed/bath linens, are capable of transmitting the virus35^, ^58.
An interesting finding in this study was the transplacental passage of the virus, which may cross the placenta of the infected mother and contaminate the fetus. According to the guidelines, it is recommended that the monitoring of infected pregnant women include fetal monitoring through ultrasound in order to detect possible abnormalities, such as fetal hepatomegaly or dropsy43.
Most studies indicate that males are the most frequently reported cases. In men, the observed age was between 20 and 67 years old, with a mean age of 35 years19^, ^20^, ^25^, ^55. In the current mpox outbreak, men often self-identify as men who have sex with men, homosexuals and bisexuals32^, ^48. Research confirms this finding, and this population requires greater attention71^, ^72.
Another relevant finding relates to the frequent report of the occurrence of MPXV in patients with human immunodeficiency virus (HIV) 48. This may be related to the incidence rate in men, who are the main group affected by HIV infection.
A study points out that in relation to exposure rates, heterosexual men account for 49% of cases and homosexuals 38%. In specific populations, such as men who have sex with men, studies indicate a high prevalence of HIV, estimated at about 18.4%73. In addition, risk factors were identified among young men, including engaging in risky behaviors and activities, such as condomless sex and being HIV positive48^, ^74.
Diagnosis
The diagnosis of MPXV infection was identified in the studies, preferably by reverse transcription followed by polymerase chain reaction (RT-PCR). Samples for RT-PCR tests are taken from blood, throat, anal region, skin vesicles and urine19^, ^52^, ^53^, ^56^, ^61. However, optimal diagnostic samples come from rash, fluids, crusts, or, in some cases, a biopsy of the lesions46.
When clinically suspecting an MPXV infection, health professionals should inquire about the patient’s travel and sexual history, as well as any close contact with people exhibiting a similar rash or with suspected or confirmed virus infection19^, ^38^, ^41.
Prevention
There are no vaccines specifically designed to protect against MPXV infection. However, numerous studies report that prior smallpox vaccination provides protection against human mpox and mitigates the severity of its clinical presentation, even though vaccine-induced immunity has progressively declined in older individuals20^, ^33^, ^41. The smallpox vaccine is estimated to provide about 85% efficacy against human mpox66.
For all cases, including suspected and confirmed contaminated patients, control measures should be implemented for patients and their contacts. It is recommended that patients be isolated at home and that surgical masks be worn by the affected patient and by the contact when sharing the same room. Personal objects, including clothes, towels and sheets should not be shared, and contact with domestic animals should be avoided. These measures should be maintained until the skin lesions have crusted over and all scabs have fallen off21^, ^45^, ^57^, ^61.
Healthcare workers should wear specific Personal Protective Equipment (PPE) for droplet and contact isolation, such as an apron, gloves, eye protection and N95/PFF2 masks62.
Treatment
The findings indicate that there is no clinically proven specific therapy for mpox. Treatment is based on symptoms and necessary clinical support, including the use of antipyretics and analgesics, maintenance of hydroelectrolytic balance, nutrition, early identification of secondary infections with prompt treatment with available antimicrobial agents37^, ^62.
A medication called Tecovirimat, also known as TPOXX or ST-246, was approved for MPXV infection in early 2022. It is recommended for use in severe cases, such as pregnant women and children21^, ^25^, ^33. However, it is not yet widely available and further studies are needed to prove its safety and efficacy.
For skin lesions, topical cidofovir at 1% has been identified as a potentially relevant therapy, but with mild systemic involvement. Its use should be evaluated based on a risk-benefit analysis25^, ^27.
Care for the multidisciplinary team and the nursing team
No studies were found that frequently and specifically addressed the care for the multidisciplinary team and, above all, the nursing team. Therefore, the results identified in this review may facilitate the management of patients with MPXV-related infection.
Strategies such as early recognition cases of MPXV infection cases through appropriate alert screening, isolation, and infection control protocols, and active case-finding in health facilities are effective in preventing and controlling widespread outbreaks and should be developed by health professionals. Additionally, possible symptoms such as fever, chills, rash, and lymphadenopathy should be monitored for a period of 21 days after the last exposure to a patient with confirmed infection or cases with characteristic rashes49^, ^56^, ^61.
The interventions adopted by the team that provides care to patients with MPXV infection should be based mainly on treating symptoms, offering support to maintain adequate fluid balance(due to the possibility of increased insensitive fluid losses through the skin, decreased oral intake and vomiting or diarrhea) providing hemodynamic support, such as supplemental oxygen or other respiratory support, if necessary, and treating secondary bacterial infections of skin lesions when indicated26^, ^37^, ^56^, ^62.
An important finding is related to management of eye infections and complications, since MPXV infection can specifically result in corneal scarring and/or vision loss. Approaches such as early ocular evaluation, application of lubricants, topical antibiotics, and possibly topical antivirals, such as trifluridine, can be used to avoid potential risks to the patient's vision35^, ^56. In this context, nursing plays a fundamental role in providing direct care to patients, in order to avoid serious injuries and maintain ocular integrity.
Psychosocial support has also been reported in studies, where professionals must provide assistance according to the needs of the patient and family. Active listening and the transmission of supportive messages can be considered strategies for psychosocial support60. Because mpox is a relatively current infection, with an increase in cases occurring in the last year, people may feel threatened and afraid of it, mainly due to the lack of information. Thus, psychosocial support is an intervention considered relevant for mpox patients care.
Thus, it is the responsibility of health professionals, especially the nursing team, who maintain closer contact with the patients, to establish interventions that promote progression of the patient's condition while considering their human responses resulting from infection with the MPXV.
This study has limitations that may relate to the databases selected identifying the studies, which may have contributed to concealing another relevant research on the topic. Regarding the level of evidence, most studies presented a low level, probably because this is a relatively current subject that has been studied little.
It is recommended that scientific studies with stronger levels of evidence, such as experimental or quasi-experimental studies, be developed to provide safer evidence for the care of these patients. It is important to note that the information contained in the results of this study may change as new studies on the subject are conducted.
Conclusion
Information available in the literature about the main clinical aspects related to human mpox cases was identified, namely: signs and symptoms, transmission, diagnosis, prevention, treatment and care for multidisciplinary team and the nursing team. Based on this, an analysis was conducted, and relevant information was compiled and organized in the results of this review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1. Gessain A Nakoune E Yazdanpanah Y .Monkeypox N Engl J Med 2022387191783179310.1056/NEJ Mra 220886036286263 · doi ↗ · pubmed ↗
- 2. World Health Organization (WHO) .WHO recommends new name for monkeypox disease 2022 https://www.who.int/news/item/28-11-2022-who-recommends-new-name-for-monkeypox-disease
- 3. Titanji BK Tegomoh B Nematollahi S Konomos M Kulkarni PA .Monkeypox: A Contemporary Review for Healthcare Professionals Open Forum Infect Dis 202297 ofac 310https://doi. org/10.1093/ofid/ofac 31010.1093/ofid/ofac 310PMC 930710335891689 · doi ↗ · pubmed ↗
- 4. Ladnyj ID Ziegler P Kima E .A human infection caused by monkeypox virus in Basankusu Territory, Democratic Republic of the Congo Bull World Health Organ 197246593597 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 2480792/pdf/bullwho 00192-0028.pdf 4340218 PMC 2480792 · pubmed ↗
- 5. UK Health Security Agency .Monkeypox cases confirmed in England-latest updates 2023 https://www.gov.uk/government/news/monkeypox-cases-confirmed-in-england-latest-updates
- 6. World Health Organization (WHO) .Multi-country monkeypox outbreak: situation update 2022 https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON 396
- 7. World Health Organization (WHO) .Multi-country outbreak of mpox, External situation report 2024 https://www.who.int/publications/m/item/multi-country-outbreak-of-mpox--external- situation-report--38-28-september-2024
- 8. Hopia H Latvala E Liimatainen L .Reviewing the methodology of an integrative review Scand J Caring Sci 201630466266910.1111/scs.1232727074869 · doi ↗ · pubmed ↗