Systemic sarcoidosis presenting as acute rapidly progressive proptosis
Maria Valeria da Silva, Yael Chavez, Maria Laura Di Nicola, Jan M. A. Delabie, Kalpana Rose, Hatem Krema

TL;DR
A patient with sudden eye swelling was diagnosed with sarcoidosis, a chronic inflammatory disease, which responded well to corticosteroid treatment.
Contribution
This case highlights an unusual acute presentation of sarcoidosis as a rapidly progressive orbital mass.
Findings
A biopsy confirmed sarcoidosis as the cause of acute proptosis.
The patient's symptoms and systemic sarcoidosis resolved with corticosteroid therapy.
Abstract
Sarcoidosis is a generalized systemic chronic inflammation that rarely involves the orbit. As a chronic inflammation, sarcoidosis typically manifests with an insidious onset and slowly progressive course. We report a case of acute-onset proptosis resulting from a rapidly growing diffuse orbital mass that simulated malignant growth, which was biopsy proven to be the first manifestation of systemic sarcoidosis. The patient demonstrated complete resolution of proptosis and systemic involvement with long-term corticosteroid treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
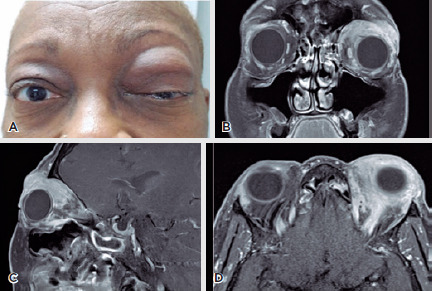 Figure 1
Figure 1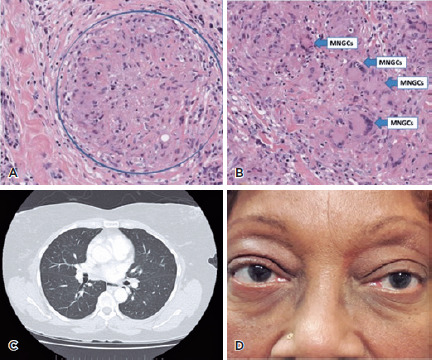 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · IgG4-Related and Inflammatory Diseases · Autoimmune and Inflammatory Disorders
INTRODUCTION
Orbital involvement with sarcoidosis is rare^(1)^. The ophthalmic literature tends to confuse isolated orbital granulomatous disease with sarcoidosis. Several authorities believe that orbital sarcoid should not be diagnosed in the absence of systemic disease^(2)^. We report a patient with an atypical clinical presentation of orbital sarcoidosis that was the first manifestation of a systemic disease.
CASE REPORT
A 63-year-old Afro-descendant woman presented with a rapidly progressive large swelling and fullness of the upper left eyelid and anterior orbit that evolved within 6 weeks. Proptosis was associated with limited painful eye movements. Her visual acuity was 20/20 in the right eye and 20/30 in the left eye. The intraocular pressure was 12 mmHg in the right eye and 18 mmHg in the left. External examination of the left eye revealed a mechanical ptosis occurring secondary to a large mass involving the superior anterior orbit (Figure 1A). On palpation, it was firm, ill-defined, and non-tender, with no redness or edema in the overlying skin. On forcible opening of the eyelids, moderate proptosis with inferior displacement of the left eye was detected. The exophthalmometry measurements were 23 mm in the right eye and 27 mm in the left eye. The eye motility was completely full in the right eye, but significant vertical and mild horizontal limitations were observed in the left eye. The result of the bilateral ocular examination was otherwise normal.
Figure 1.(A) Clinical picture at first presentation. A 63-year-old Afro-descendant woman presented with a 2-month history of progressive swelling of the upper left eyelid associated with painful eye movement. (B) Coronal- and (C) sagittal-, and (D) axial-view orbital magnetic resonance images showing an extensive orbital mass occupying the superior aspect of the left anterior orbit that involved the lacrimal gland, superior rectus muscle, levator muscle complex, and portion of the lateral rectus. The orbital apex was clear.
The patient consented to the publication of this case report and its related images.
Differential diagnosis
On the basis of the absence of signs of acute inflammation and the rapidly progressive course, the provisional differential diagnosis included an acute lymphoproliferative process or a malignant infiltrative neoplasm of either primary or metastatic origin.
Investigations
Magnetic resonance imaging revealed an extensive orbital mass occupying the superior aspect of the left anterior orbit that involved the lacrimal gland, superior rectus muscle, levator muscle complex, and part of the lateral rectus. The orbital apex was clear (Figure 1 B,C,D).
Histopathological examination of an incisional biopsy revealed many “naked” non-necrotizing granulomas (Figure 2A). The stroma was composed of epithelioid cells, scattered small lymphocytes, histiocytes, and numerous multinucleated giant cells (Figure 2B). Special staining for acid-fast bacilli and fungal organisms did not reveal any microorganisms. The non-necrotizing granulomatous inflammation was most consistent with sarcoidosis. Consequently, the patient submitted to systemic screening for sarcoidosis. On thoracic computed tomography (CT), prominent and enlarged mediastinal and bilateral hilar lymph nodes with no parenchymal manifestations were detected (Figure 2C).
Figure 2.Histopathology of an incisional biopsy showing (A) many “naked” non-necrotizing granulomas. (B) As shown, the stroma was composed of epithelioid cells, scattered small lymphocytes, histiocytes, and numerous multinucleated giant cells (MNGCs). (C) The thoracic computed tomography scan shows prominent and enlarged mediastinal and bilateral hilar lymph nodes with no parenchymal manifestation. (D) The clinical picture of the patient after 2 years of diagnosis without signs of relapse of the disease in the orbit.
Treatment
The patient was treated initially with 50 mg of prednisone, and the dose was tapered slowly over a few months to a maintenance dose of 5 mg every other day.
Outcome and follow-up
The patient demonstrated rapid regression of proptosis and ptosis with full restoration of ocular motility. The CT scan performed 2 months after the treatment revealed a significant interval decrease in the size of the infiltrative soft tissue mass in the left orbit, ruling out the provisional differential diagnosis. No signs of relapse of the disease were found in the orbit or thorax 4 years after diagnosis (Figure 2D).
DISCUSSION
Sarcoidosis is a generalized chronic multi-systemic inflammation. It has a predilection for females in their fifth to seventh decades of life and patients of African descent^(3)^. Ophthalmic involvement occurs in almost 25% of patients with sarcoidosis, manifesting mostly as chronic uveitis, with orbital involvement representing <1% of the ophthalmic manifestations^(1^, ^4)^. However, orbital involvement frequently occurs without prior history of systemic sarcoidosis^(1)^.
In a large series of orbital lesions, it represented <0.2% of all lesions and 2% of the orbital inflammatory lesions^(5)^. Our patient has the typical demographics of a patient with sarcoidosis; however, the acute rapidly progressive course of few weeks for such an extensive orbital lesion is atypical for a chronic inflammatory process. In a series of orbital and adnexal sarcoidosis, the most common complaint was a slowly progressive mass in 88.5% of the cases, with discomfort in 30%^(1)^. The rapidly progressive clinical presentation in our patient was suggestive of a malignant process, which was refuted by the orbital biopsy findings, presence mediastinal lymph node enlargement in the subsequent thoracic imaging, and the prompt response to steroid treatment. Albeit rare, our case emphasizes the importance of including sarcoidosis in the differential diagnosis of acute rapidly progressive orbital lesions and considering systemic surveillance of the disease if biopsy revealed orbital sarcoidosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prabhakaran VC Saeed P Esmaeli B Sullivan TJ Mc Nab A Davis G Orbital and adnexal sarcoidosis Arch Ophthalmol 200712512165716621807111810.1001/archopht.125.12.1657 · doi ↗ · pubmed ↗
- 2Mombaerts I Schlingemann RO Goldschmeding R Koornneef L Idiopathic granulomatous orbital inflammation Ophthalmology 19961031221352141900334910.1016/s 0161-6420(96)30378-3 · doi ↗ · pubmed ↗
- 3Petrarolha SM Rodrigues BS Filho FD Dedivitis RA Petrarolha SB Morais PM Unilateral eyelid edema as initial sign of orbital sarcoidosis Case Rep Ophthalmol Med 20162016691292769129272729874610.1155/2016/6912927 PMC 4889789 · doi ↗ · pubmed ↗
- 4Obenauf CD Shaw HE Sydnor CF Klintworth GK Sarcoidosis and its ophthalmic manifestations Am J Ophthalmol 197886564865556888610.1016/0002-9394(78)90184-8 · doi ↗ · pubmed ↗
- 5Shields JA Shields CL Scartozzi R Survey of 1264 patients with orbital tumors and simulating lesions: The 2002 Montgomery Lecture, part 1Ophthalmology 2004111599710081512138010.1016/j.ophtha.2003.01.002 · doi ↗ · pubmed ↗