Successful Repair of Esophageal Atresia with Tracheoesophageal Fistula and Interrupted Inferior Vena Cava: A Rare Case Report
Xiao Long Mu, Junqiu Wang

TL;DR
A rare case of a newborn with esophageal atresia and a tracheoesophageal fistula, along with an interrupted inferior vena cava, was successfully treated with careful surgical planning.
Contribution
Highlights a rare association of EA, TEF, and interrupted IVC, emphasizing the need for imaging to guide safe surgical repair.
Findings
EA with TEF and interrupted IVC can be successfully repaired with thoracotomy.
Prenatal and postnatal imaging is critical to identify vascular anomalies before surgery.
Preserving the azygos vein is essential to avoid life-threatening complications.
Abstract
Esophageal atresia (EA) with tracheoesophageal fistula (TEF) is a congenital anomaly that can present complex surgical challenges, especially when accompanied by rare vascular conditions like an interrupted inferior vena cava (IVC). The division of the azygos vein is a common part of TEF repair, but in the presence of an interrupted IVC, this can lead to life-threatening complications. We report the case of a newborn diagnosed with EA, TEF, and interrupted IVC, successfully treated through thoracotomy. This case underscores the importance of prenatal and postnatal imaging to diagnose vascular anomalies prior to TEF repair, ensuring the preservation of the azygos vein to prevent fatal outcomes. Raising awareness of this rare association is crucial to optimizing surgical planning and outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1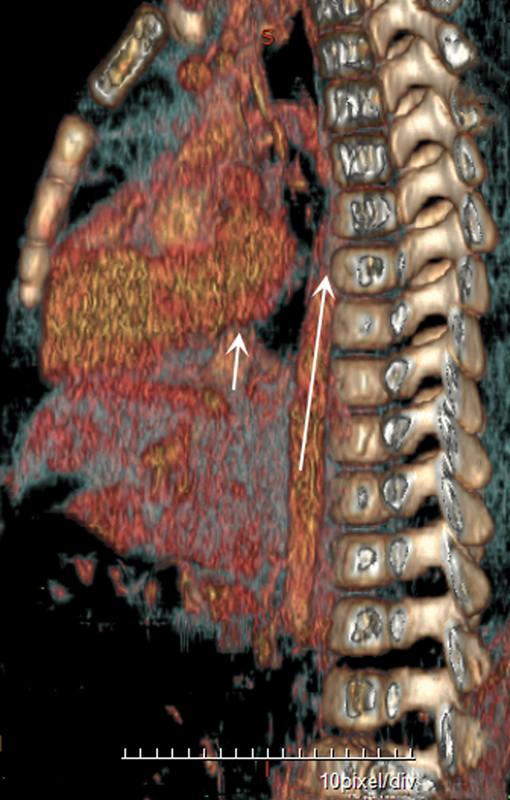 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Tracheal and airway disorders · Congenital Diaphragmatic Hernia Studies
Introduction
Esophageal atresia (EA) is a congenital abnormality of the esophagus that is caused by incomplete embryonic compartmentalization of the foregut. EA commonly occurs with a tracheoesophageal fistula (TEF). 1 The overall worldwide prevalence of EA as calculated from national and international databases for congenital anomalies is 2 to 4 per 100,000 births. 1 Interrupted inferior vena cava (IVC) is a rare disease. According to postnatal series, interrupted IVC with azygos or hemiazygos continuation is a rare disorder occurring in 0.6 to 3% of the population with congenital heart disease. 2 Therefore, the association of interrupted IVC, EA with TEF, is exceedingly rare. EA and TEF accompanied by interrupted IVC that underwent successful repair in a few pediatric cases has been described. 1 3 Before undertaking TEF surgery, most authors advise dividing the azygos vein. 1 4 References do not routinely recommend checking for an interrupted IVC preoperatively. 1 5 However, dividing the azygos vein in the presence of an interrupted IVC may result in death. The aim of this study was to analyze the clinical and radiological features of EA and TEF accompanied by interrupted IVC in newborns. It emphasizes the importance of diagnosing interrupted IVC before undertaking TEF surgery and raises awareness of the importance of diagnosing vascular anomalies prior to EA and TEF repair ( Supplementary Material 1 , available in the online version). 4 5
Case Report
Patient history: A 2.85-kg female infant was delivered at 39 weeks of gestation by natural labor (November 19, 2020), with a 1-minute Apgar score 10 points. Maternal health in good. A fetal echocardiogram performed at 35 weeks demonstrated EA and an interrupted IVC with azygos continuation to the right-sided superior vena cava. A postnatal echocardiogram confirmed the interrupted IVC, which does not involve the hepatic segment of the IVC, and light cardiac anomalies with small atrial septal defect and mildly tricuspid regurgitation.
Diagnosis: The patient was intubated at birth but resistance was noted during orogastric tube insertion. Chest X-ray revealed ( Fig. 1 ) the gastric tube at the upper pouch of the esophagus with the presence of intestinal gas, which is a classic feature of type C EA. Thoracotomy repair of EA was scheduled for the next day following stabilization.
Chest radiograph on lateral view showed the orogastric tube inserted at the proximal esophageal pouch ( short arrow ) with distal bowel gas, esophageal atresia with distal tracheoesophageal fistula ( long arrow ).
Surgical procedure: The patient was positioned in a semi-prone position with the right chest slightly elevated. She was put on conventional ventilation without single lung ventilation. The patient underwent right intrapleural thoracotomy, based on the echocardiographic findings of an interrupted IVC and azygos continuation to the superior vena cava. The pediatric surgeon preserved the azygos vein connection at the time of the TEF repair to prevent obstruction of the venous return from the lower body. Through a right intrapleural thoracotomy, 5–0 Monocryl was used as anastomotic suture material and end-to-end esophageal anastomosis. All operations were performed by three qualified pediatric surgeons. A 10-Fr chest drain was inserted at the end of the procedure. The operation was uneventful and completed in 145 minutes.
Postoperative care: After surgery, the patient was managed in the neonatal intensive care unit according to our usual protocol. The patient was extubated successfully on day 4 after surgery. She was discharged home at the age of 15 days. At 6 months of age, enhanced computed tomography (CT) showed ( Fig. 2 ) the hepatic segment of the IVC draining hepatic veins and not continuing further caudally. Iliac and renal veins drained via the distended azygos vein within the abdomen, entering the thorax and draining into the superior vena cava within the thorax, and by 12 months of age her small atrial septal defect, measured by Doppler echocardiography, was normal. At the follow-up visit until April 5, 2024, she was doing well, she had good weight gain with full oral feeding, and no clinical gastroesophageal reflux.
Contrast-enhanced computed tomography on sagittal view showed a hepatic segment of the inferior vena cava draining hepatic veins ( short arrow ) and not continuing further caudally. Iliac and renal veins drained via the distended azygos vein within the abdomen, entering the thorax and draining into the superior vena cava within the thorax ( long arrow ).
Discussion
Interrupted IVC with azygos or hemiazygos vein continuation is a rare congenital anomaly. 2 It usually involves the hepatic segment of the IVC. According to a postnatal series, its estimated prevalence is 0.15%. 2 EA with or without TEF is the most common anomaly of the esophagus (incidence of 2–4/10,000 births). 1 The infrahepatic interruption of the IVC with azygos and hemiazygos continuation is a rare finding especially when it is associated with EA and TEF. 2 6 Interrupted IVC is associated with congenital heart disease in approximately 85% of cases, and frequently with the polysplenia syndrome. Our patient demonstrated light cardiac anomalies with small atrial septal defect, without polyspenia. 2 3 7 To the best of our knowledge, there has only been one report of this combination in a patient who survived surgery and continues to do well, 8 but there are few studies analyzing the radiological features of EA and TEF accompanied by interrupted IVC. This study analyzed the clinical and radiological features of EA and TEF accompanied by interrupted IVC, reported the successful outcome of the rare presentation of EA with TEF and an interrupted IVC, and emphasized that all EA patients should undergo a detailed evaluation of IVC during preoperative assessment.
The most commonly involved segment of interrupted IVC is the hepatic segment. It is due to the failure of the development of the hepatocardiac canal during the embryo, in its 10 to 15 mm length. 2 This patient's infrahepatic part was atretic; the iliac and renal veins drained via the distended azygos vein within the abdomen, entering the thorax and draining into the superior vena cava. IVC interruption can be diagnosed through prenatal or postnatal imaging. Noninvasive imaging modalities such as contrast-enhanced CT and magnetic resonance imaging are the most reliable methods for identification of these anomalies in an asymptomatic patient, and contrast-enhanced CT scan and venography can be helpful. Note was made of interrupted IVC, which drained only the hepatic veins before entering the right atrium. 9 The infrahepatic IVC continues as the azygos vein. Recognizing this venous anomaly is important for the pediatric surgeon, especially for conditions such as a paracardiac or mediastinal mass on chest radiography.
Although EA can be diagnosed antenatally, most patients (>90%) are diagnosed after birth. EA is prenatally diagnosed in a minority of cases and is usually only suspected on the basis of the presence of indirect or direct signs on ultrasonography. MRI with dynamic sequence and biochemical evaluation of the amniotic fluid have been developed to help in the diagnosis of EA. 5 6 10
Different surgical techniques are available. The optimal approach is dependent on the type of EA. Division of the azygos has been part of the TEF repair since Cameron Haight's report of the first successful procedure. 6 However, references do not routinely recommend checking for an interrupted IVC preoperatively. Dividing the azygos vein in the presence of an interrupted IVC may result in death. 9 10 Some suggest inspecting the size of the azygos vein prior to division, as a large azygos vein may be consistent with an interrupted IVC. 9 10 11 Patients born with EA should ideally be evaluated in a multidisciplinary team consisting of a pediatric surgeon, a gastroenterologist, a pulmonologist, and an otolaryngologist.
For TEF repair, it is important to be aware of the patients' vascular anatomy before surgery. 3 6 12 Accurate diagnosis of an abnormal IVC position and course can help the pediatric surgery expert in surgical planning, avoid unnecessary treatment measures, and prevent accidental injury caused by complications.
In conclusion, this case highlights the complexity of managing EA with TEF in the presence of an interrupted IVC. Early and accurate diagnosis of vascular anomalies through prenatal or postnatal imaging is essential for optimal surgical planning and avoiding potentially fatal complications. The preservation of the azygos vein during repair was critical in ensuring a successful outcome. This report emphasizes the importance of multidisciplinary care and comprehensive imaging in rare congenital cases to improve patient survival and outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Keefe G Culbreath K Edwards E M Current outcomes of infants with esophageal atresia and tracheoesophageal fistula: a multicenter analysis J Pediatr Surg 2022570697097435300859 10.1016/j.jpedsurg.2022.01.060 · doi ↗ · pubmed ↗
- 2Babaoğlu K Doğan Y Başar E Z Usta E Prenatal diagnosis of hepatic interruption of the inferior vena cava with azygos/hemiazygos continuation without structural heart defects: a case series J Clin Ultrasound 2022500679580235355279 10.1002/jcu.23209 · doi ↗ · pubmed ↗
- 3Tie H X Ma B Zhang D C Li T G Prenatal diagnosis of fetal inferior vena cava malformation using H Dlive flow combined with spatiotemporal image correlation Echocardiography 2022390568569035355321 10.1111/echo.15346 · doi ↗ · pubmed ↗
- 4Walk R M Esophageal atresia and tracheoesophageal fistula: overview and considerations for the general surgeon Surg Clin North Am 20221020575977836209744 10.1016/j.suc.2022.07.008 · doi ↗ · pubmed ↗
- 5van Lennep M Singendonk M MJ Dall'Oglio L Oesophageal atresia Nat Rev Dis Primers 20195012631000707 10.1038/s 41572-019-0077-0 · doi ↗ · pubmed ↗
- 6Midwest Pediatric Surgery Consortium Marquart J P Bowder A N Bence C M Thoracoscopy versus thoracotomy for esophageal atresia and tracheoesophageal fistula: outcomes from the Midwest Pediatric Surgery Consortium J Pediatr Surg 20235801273336283849 10.1016/j.jpedsurg.2022.09.015 · doi ↗ · pubmed ↗
- 7Liu Y Guo D Li J Radiological features of azygos and hemiazygos continuation of inferior vena cava: a case report Medicine (Baltimore)20189717 e 054629703035 10.1097/MD.0000000000010546 PMC 5944491 · doi ↗ · pubmed ↗
- 8Evans W N Kogut K Acherman R J Preserving the azygos vein when repairing esophageal atresia and tracheoesophageal fistula accompanied by interrupted inferior vena cava Pediatr Surg Int 2014300334534724122074 10.1007/s 00383-013-3422-5 · doi ↗ · pubmed ↗