Stewarding beyond the 9–5: Implementation of overnight review of rapid blood culture identification panel results by intensive care unit pharmacists
Sarah M. Arduser Sindelar, Jonathan H. Ryder, Jeremy Tigh, Theodore Blum, Jessica Prucha, Paul Fey, Scott J. Bergman, Trevor C. Van Schooneveld, Shawnalyn W. Sunagawa

TL;DR
This study shows that having ICU pharmacists review blood culture results overnight improves how quickly patients get proper antibiotic treatment.
Contribution
The novel contribution is implementing overnight review of blood culture results by ICU pharmacists to improve antimicrobial stewardship outside regular hours.
Findings
Overnight review reduced time to evaluation from 9.3 to 3.6 hours.
The change was statistically significant (P < .01).
Abstract
Rapid blood culture identification is most effective with antimicrobial stewardship feedback, which is limited during non-business hours. We implemented overnight review of Blood Culture Identification 2 panel results by intensive care unit pharmacists and demonstrated reduced time to evaluation (3.6 vs 9.3 hours, P < .01).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
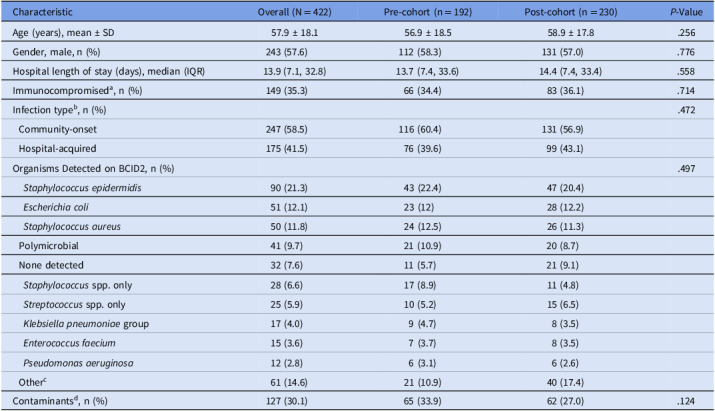 Figure 1
Figure 1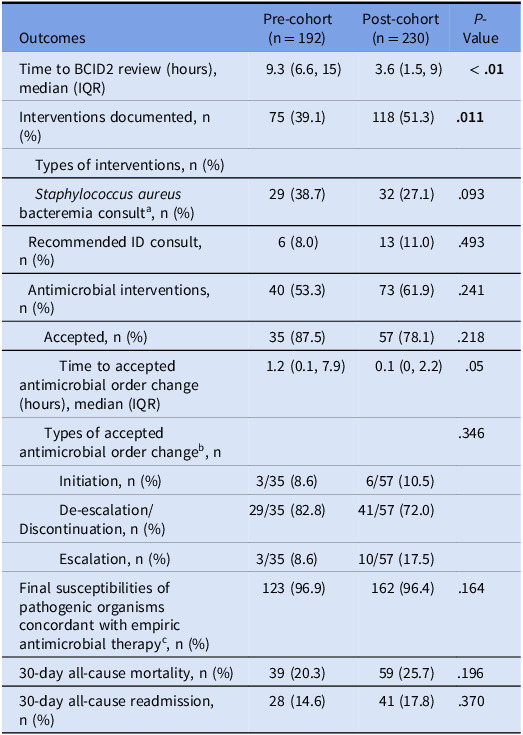 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Antibiotic Use and Resistance · Antimicrobial Resistance in Staphylococcus
Introduction
The BioFire® Blood Culture Identification 2 (BCID2) panel (BioMérieux) is a rapid diagnostic tool that detects bacterial and yeast pathogen genetic targets and antimicrobial resistance markers in positive blood cultures, providing organism identification within 1–2 hours.^ 1 ^ Rapid blood culture diagnostics in combination with antimicrobial stewardship program (ASP) interventions decrease time to optimization of antimicrobials, resulting in decreased mortality, shorter hospital lengths of stay, and lower costs.^ 2–6 ^ However, traditional ASP review typically occurs only on weekdays during business hours, potentially limiting these interventions.
In August 2021, Nebraska Medicine upgraded from the original BCID to the BCID2 panel and updated guidance for clinicians. ASP performs review of all blood culture results during business hours on weekdays. To optimize care for the most critically ill patients with bloodstream infections, we implemented a workflow in September 2022 for the overnight intensive care unit (ICU) clinical pharmacist to review BCID2 results in ICUs reported after ASP hours. The ICU pharmacists were selected since they provide 24-hour, 7-day-a-week on-site care to patients most likely to benefit from early appropriate antibiotic therapy. Thus, the objective of this study was to assess the impact of overnight ICU pharmacist review on time to evaluation of antimicrobials based on BCID2 results and accepted antimicrobial order recommendations based on our institutional ASP guidance.
Methods
We conducted a single-center, quasi-experimental quality improvement study at an academic medical center licensed for 718 beds, including 96 ICU beds. Patients were included if they had a positive blood culture with a BCID2 result while in an ICU during overnight clinical pharmacist coverage (21:00–07:00) Monday–Friday (Supplemental Figure 1). We compared ASP review of BCID2 results from overnight August 1, 2021 to August 31, 2022 (pre-cohort) to overnight ICU pharmacist review from September 1, 2022 to September 30, 2023 (post-cohort). Patients were excluded if they transferred from outside hospitals with bloodstream infections, had recurrent bloodstream infections with the same organism, and patients discharged or deceased within 24 hours of BCID2 results. We chose to exclude BCID2 results between Friday after 17:00 and Monday before 7:00 for intervention comparison between our cohorts because these results would not always be reviewed routinely by weekday ASP.
The primary outcome was time to evaluation of therapy based on BCID2 result, defined as hours from BCID2 result to time of review documentation by ASP or overnight ICU pharmacists. The overnight ICU pharmacist reviewed BCID2 results per institutional workflow (Supplemental Figure 2) and provided recommendations in concordance with the ASP guidance for BCID2 results (Supplemental Material). All BCID2 results were reviewed; however, intervention occurred only when a change in therapy was recommended (Supplemental Figure 3). Secondary outcomes included number and types of documented interventions, accepted antimicrobial interventions, time to accepted antimicrobial order changes, types of accepted antimicrobial order changes, empiric antimicrobial concordance with final pathogen susceptibilities, 30-day all-cause mortality, and 30-day all-cause readmission. Time to accepted antimicrobial order changes were defined as time of ASP or overnight ICU pharmacist BCID2 review to time of antibiotic order placement.
Interventions were categorized as antimicrobial order changes, initiation of infectious diseases (ID) consults, or Staphylococcus aureus bacteremia consults. Institutional policy requires an ID consult for all patients with Staphylococcus aureus bacteremia. If not already consulted, this process is initiated by ASP or recommended by overnight ICU pharmacists. For antimicrobial order changes, effective empiric therapy was defined as administration of an antimicrobial to which the organism demonstrated in vitro susceptibility (ie, reported as susceptible per Clinical and Laboratory Standards Institute). Each study outcome was independently adjudicated by three investigators (S.W.S., J.H.R., J.T.), and our institutional review board deemed this project as quality improvement exempt from review. Descriptive statistics were performed for cohort characteristics. Primary and secondary outcomes were compared using independent sample t-tests, χ^2^, Fisher’s exact, and Mann-Whitney U tests.
Results
There were 422 overnight BCID2 results from 395 patients included, 192 in the pre-cohort and 230 in the post-cohort. Table 1 summarizes cohort characteristics, including BCID2 organisms. There were no significant differences between the two groups. Infections were more frequently classified as community-onset (58.5%), defined as positive blood cultures drawn ≤ 48 hours of hospital admission, with Staphylococcus epidermidis (21.3%) and Escherichia coli (12.1%) detected most often. There were 41 (9.7%) polymicrobial BCID2 results and 32 (7.6%) had no targets detected on BCID2.
Table 1.Cohort characteristicsCharacteristicOverall (N = 422)Pre-cohort (n = 192)Post-cohort (n = 230) P-ValueAge (years), mean ± SD 57.9 ± 18.156.9 ± 18.558.9 ± 17.8.256Gender, male, n (%)243 (57.6)112 (58.3)131 (57.0).776Hospital length of stay (days), median (IQR)13.9 (7.1, 32.8)13.7 (7.4, 33.6)14.4 (7.4, 33.4).558Immunocompromised^ a ^, n (%)149 (35.3)66 (34.4)83 (36.1).714Infection type^ b ^, n (%).472 Community-onset247 (58.5)116 (60.4)131 (56.9) Hospital-acquired175 (41.5)76 (39.6)99 (43.1)Organisms Detected on BCID2, n (%).497 * Staphylococcus epidermidis* 90 (21.3)43 (22.4)47 (20.4) * Escherichia coli* 51 (12.1)23 (12)28 (12.2) * Staphylococcus aureus* 50 (11.8)24 (12.5)26 (11.3) Polymicrobial41 (9.7)21 (10.9)20 (8.7) None detected32 (7.6)11 (5.7)21 (9.1) * Staphylococcus* spp. only28 (6.6)17 (8.9)11 (4.8) * Streptococcus* spp. only25 (5.9)10 (5.2)15 (6.5) * Klebsiella pneumoniae* group17 (4.0)9 (4.7)8 (3.5) * Enterococcus faecium* 15 (3.6)7 (3.7)8 (3.5) * Pseudomonas aeruginosa* 12 (2.8)6 (3.1)6 (2.6) Other^ c ^ 61 (14.6)21 (10.9)40 (17.4)Contaminants^ d ^, n (%)127 (30.1)65 (33.9)62 (27.0).124Abbreviations: BCID2, Blood Culture Identification 2; SD, standard deviation; IQR, interquartile range. a Solid organ transplant, bone marrow transplant, hematology/oncology, human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS). b Community-onset = positive blood cultures drawn ≤ 48 hours of hospital admission; Hospital-acquired = positive blood cultures drawn > 48 hours of hospital admission. c
Enterococcus faecalis (n = 8), Streptococcus pneumoniae (n = 6), Enterobacterales order only (n = 6), Klebsiella aerogenes (n = 6), Serratia marcescens (n = 5), Candida albicans (n = 5), Candida glabrata (n = 5), Streptococcus pyogenes (n = 4), Klebsiella oxytoca (n = 4), Enterobacter cloacae complex (n = 3), Staphylococcus lugdunensis (n = 2), Streptococcus agalactiae (n = 2), Acinetobacter baumannii complex (n = 1), Bacteroides fragilis (n = 1), Salmonella spp. (n = 1), Haemophilus influenzae (n = 1), Candida parapsilosis (n = 1). d 1 positive blood culture set out of 2 sets with Gram-positive microorganisms indicated by microbiology lab.
Median time to BCID2 review was significantly reduced in the post-cohort compared to the pre-cohort (3.6 hours vs 9.3 hours, P < .01). A higher proportion of patients had documented interventions in the post-cohort versus the pre-cohort (51.3% vs 39.1%, P = .011). Acceptance rates of antimicrobial interventions were not significantly different between the groups: 78.1% in the post-cohort compared to 87.5% in the pre-cohort (P = .218).
Among accepted antimicrobial interventions, time to antimicrobial order changes was also reduced in the post-cohort (0.1 hours vs 1.2 hours, P = .05). Table 2 summarizes types of accepted antimicrobial order changes and additional secondary outcomes. No statistical differences were observed in empiric antimicrobial concordance with final pathogen susceptibilities, 30-day mortality, or 30-day readmission.
Table 2.Primary and secondary outcomesOutcomesPre-cohort (n = 192)Post-cohort (n = 230) P-ValueTime to BCID2 review (hours), median (IQR)9.3 (6.6, 15)3.6 (1.5, 9) < .01 Interventions documented, n (%)75 (39.1)118 (51.3) .011 Types of interventions, n (%) * Staphylococcus aureus* bacteremia consult^ a ^, n (%)29 (38.7)32 (27.1).093 Recommended ID consult, n (%)6 (8.0)13 (11.0).493 Antimicrobial interventions, n (%)40 (53.3)73 (61.9).241 Accepted, n (%)35 (87.5)57 (78.1).218 Time to accepted antimicrobial order change (hours), median (IQR)1.2 (0.1, 7.9)0.1 (0, 2.2).05 Types of accepted antimicrobial order change^ b ^, n.346 Initiation, n (%)3/35 (8.6)6/57 (10.5) De-escalation/Discontinuation, n (%)29/35 (82.8)41/57 (72.0) Escalation, n (%)3/35 (8.6)10/57 (17.5)Final susceptibilities of pathogenic organisms concordant with empiric antimicrobial therapy^ c ^, n (%)123 (96.9)162 (96.4).16430-day all-cause mortality, n (%)39 (20.3)59 (25.7).19630-day all-cause readmission, n (%)28 (14.6)41 (17.8).370Abbreviations: BCID2, Blood Culture Identification 2; ID, infectious diseases; IQR, interquartile range. a
Staphylococcus aureus bacteremia consults include Staphylococcus aureus detected in polymicrobial BCID2 results (Pre-cohort, n = 5; Post-cohort, n = 6) and Staphylococcus aureus alone detected by BCID2 (Pre-cohort, n = 24; Post-cohort, n = 26). b Initiation = starting an antimicrobial with activity against the pathogen detected by BCID2; De-escalation/Discontinuation = narrowing spectrum of activity or stopping of therapy; Escalation = broadening spectrum of activity of therapy with patients already initiated on antimicrobials. c Pre-cohort = 127 pathogenic organisms; Post-cohort = 168 pathogenic organisms; Susceptibilities were not performed on contaminants.
Discussion
We evaluated the impact of adding overnight pharmacist review of BCID2 results to a typical ASP workflow demonstrating an increase in interventions as well as reduction in time to review and intervention. While current literature focuses primarily on ID and ASP review of rapid diagnostics, our study highlights a novel expansion of these activities utilizing ICU pharmacists to act as ASP extenders by implementing prospective audit and feedback in concordance with ASP guidance. The decreased time to antimicrobial order changes was likely due to earlier review of BCID2 results and communication of recommendations with ICU providers via telephone or secure private messaging.
Furthermore, the significantly higher number of documented interventions post-implementation demonstrated the impact of more rapid reviews, which allowed for faster changes in antimicrobials. There were numerically lower acceptance rates of overnight ICU pharmacist recommendations, which may be the result of intervention timing with cross-covering overnight care teams being less willing to make changes without primary team consideration. However, the ASP team created and implemented clear BCID2 guidance for ICU pharmacists to ensure appropriate institutional-based recommendations.
In patients with accepted antimicrobial interventions, the overnight ICU pharmacist workflow (Supplemental Figure 2) was associated with a reduced median subsequent time to antimicrobial change. These results further support that earlier review of rapid diagnostics by non-ASP clinicians have the ability to decrease time to initiation of effective therapy.^ 7,8 ^ Among patients who warranted initiation or escalation of antibiotics, this is a significant finding, as delaying effective antimicrobial therapy for bloodstream infections has been associated with increased mortality.^ 9 ^ Although there was no significant difference in the types of accepted antimicrobial order changes, there was a higher percentage of initiations and escalations of therapy within the post-cohort.
Additional strengths include our definitions of antimicrobial order changes being mostly aligned with previous studies.^ 7,10 ^ However, the lack of concordance in definitions and differentiation between spectrum of activity and exposure to more than one antimicrobial complicates these antimicrobial therapy definitions. Furthermore, a high percentage of concordance of final susceptibilities with empiric therapy was maintained in the post-cohort demonstrating our ICU pharmacists’ recommendations were appropriate based on our institutional ASP BCID2 guidance and local antibiogram patterns.
Limitations include its single-center, retrospective, pre-post study design. Only overnight BCID2 results for ICU patients were reviewed, so future studies are warranted to explore the impact of a similar intervention in non-ICU settings. An additional limitation was the potential for missing intervention documentation. As a result of this project, we completed additional education on the overnight ICU pharmacist workflow (Supplemental Figure 2) with emphasis on review/intervention documentation. Finally, implementation of overnight ICU BCID2 review included the first month of our post-group cohort which may have introduced bias.
Our study demonstrates the benefit of rapid diagnostics in combination with overnight ICU pharmacy services to improve time to stewardship intervention. Our findings emphasize the importance of integrating rapid diagnostics and continuous ASP review, specifically in the ICU, to optimize the management of bloodstream infections.
Supplementary material
For supplementary material accompanying this paper visit http://doi.org/10.1017/ash.2025.28.click here to view supplementary material
Supporting information
Arduser Sindelar et al. supplementary materialArduser Sindelar et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sparks R , Balgahom R , Janto C , Polkinghorne A , Branley J. Evaluation of the Bio Fire blood culture identification 2 panel and impact on patient management and antimicrobial stewardship. Pathol 2021;53:889–895.10.1016/j.pathol.2021.02.01634120744 · doi ↗ · pubmed ↗
- 2Timbrook TT , Morton JB , Mc Coneghy KW , Caffrey AR , Mylonakis E , La Plante KL. The effect of molecular rapid diagnostic testing on clinical outcomes in bloodstream infections: a systematic review and meta-analysis. Clin Infect Dis 2017;64:15–23.27678085 10.1093/cid/ciw 649 · doi ↗ · pubmed ↗
- 3Banerjee R , Teng CB , Cunningham SA , et al. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin Infect Dis 2015;61:1071–1080.26197846 10.1093/cid/civ 447PMC 4560903 · doi ↗ · pubmed ↗
- 4Pardo J , Klinker KP , Borgert SJ , Butler BM , Giglio PG , Rand KH. Clinical and economic impact of antimicrobial stewardship interventions with the Film Array blood culture identification panel. Diagn Microbiol Infect Dis 2016;84:159–164.26639226 10.1016/j.diagmicrobio.2015.10.023 · doi ↗ · pubmed ↗
- 5Wenzler E , Timbrook TT , Wong JR , Hurst JM , Mac Vane SH. Implementation and optimization of molecular rapid diagnostic tests for bloodstream infections. Am J Health Syst Pharm 2018;75:1191–1202.29970407 10.2146/ajhp 170604 · doi ↗ · pubmed ↗
- 6Barlam TF , Cosgrove SE , Abbo LM , et al. Implementing an antibiotic stewardship program: guidelines by the infectious diseases society of America and the society for healthcare epidemiology of America. Clin Infect Dis 2016;62:e 51–77.27080992 10.1093/cid/ciw 118PMC 5006285 · doi ↗ · pubmed ↗
- 7Wilde AM , Song M , Allen WP , et al. Implementation of a pharmacy-driven rapid bacteremia response program. Am J Health Syst Pharm 2024;81:74–82.37658845 10.1093/ajhp/zxad 211 · doi ↗ · pubmed ↗
- 8Gawrys GW , Tun K , Jackson CB , et al. The impact of rapid diagnostic testing, surveillance software, and clinical pharmacist staffing at a large community hospital in the management of gram-negative bloodstream infections. Diagn Microbiol Infect Dis 2020;98:115084.32603973 10.1016/j.diagmicrobio.2020.115084 · doi ↗ · pubmed ↗