Metastatic Melanoma to Ovary and Advances in Metastatic Melanoma Treatment: A Case Report
Melissa Cantave, Anita H Chen, Aakriti R Carrubba, Matthew Robertson

TL;DR
This case report describes a rare instance of melanoma spreading to the ovary and highlights recent advances in treatment.
Contribution
The paper adds a new case to the literature on rare melanoma metastasis to the ovary and discusses recent treatment advances.
Findings
Melanoma metastasis to the ovary is rare and often difficult to diagnose.
Surgical excision and advances in genetic testing and systemic therapy offer potential treatment options.
The prognosis for patients with ovarian metastases from melanoma remains poor.
Abstract
Metastatic lesions to the ovary from melanoma are very rare. There have been several published case reports over the years documenting melanoma metastasizing to the adnexa. Ovarian metastases may either be asymptomatic or present with pelvic pain. As with most adnexal masses, diagnosis can be challenging and depends on the quality of imaging. When present, the prognosis is very poor. Surgical excision can be offered for symptomatic management, confirmation or diagnosis, and for cytoreduction; however, advances in genetic testing and systemic therapy have shown promise in treating this disease. To add to the growing body of literature, we present a case of melanoma metastasizing to the ovary and will discuss the advances in systemic therapy as well as genetic testing for these patients.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
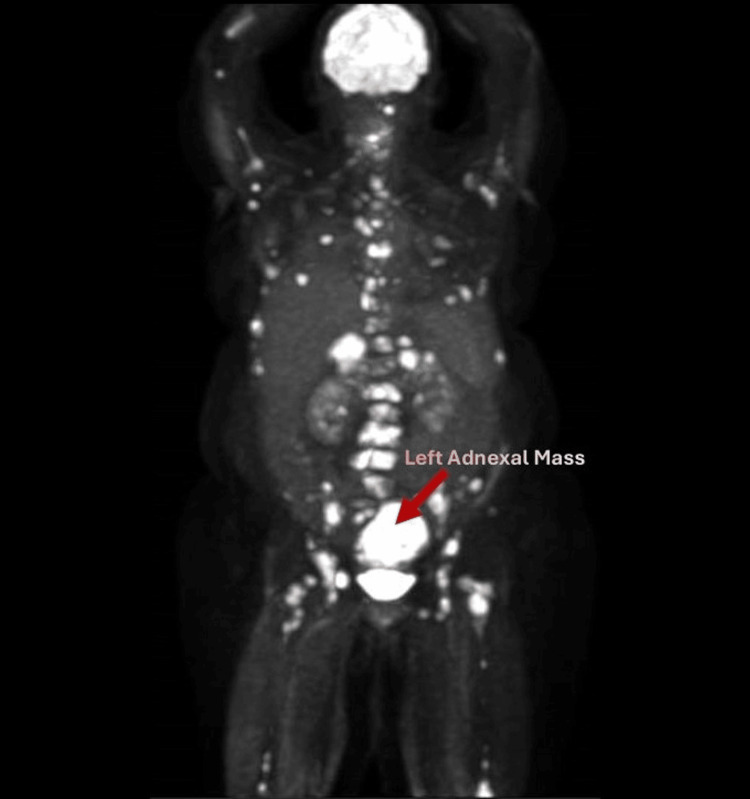 Figure 1
Figure 1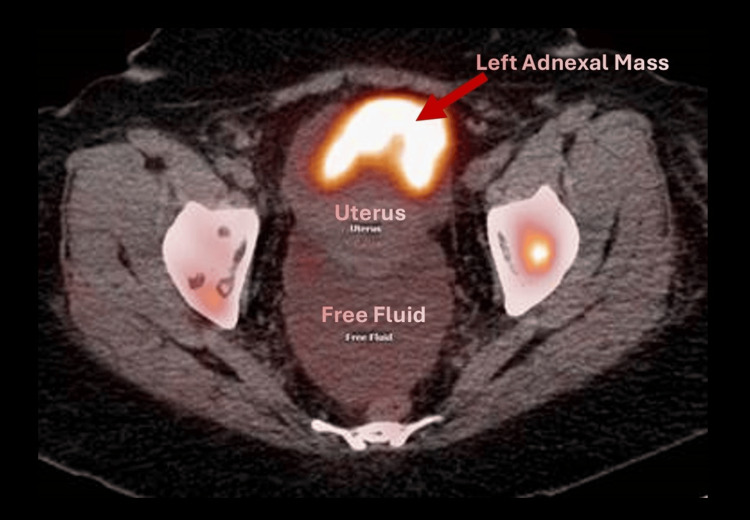 Figure 2
Figure 2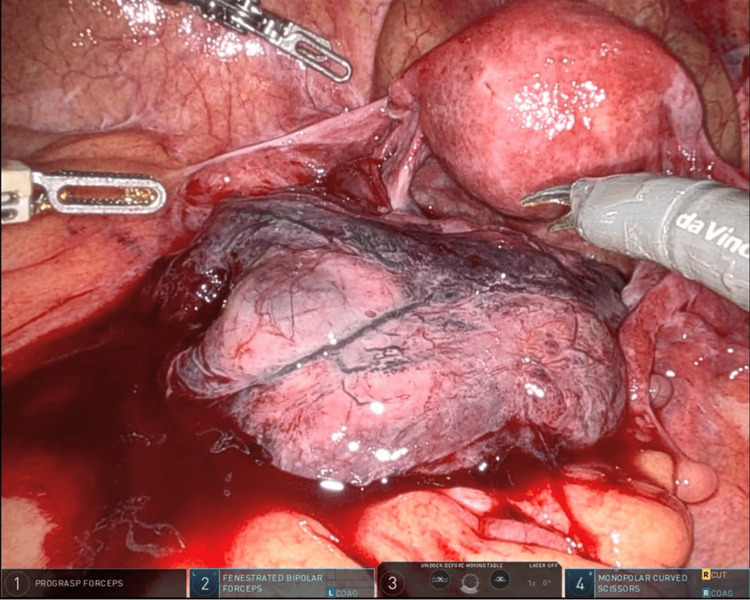 Figure 3
Figure 3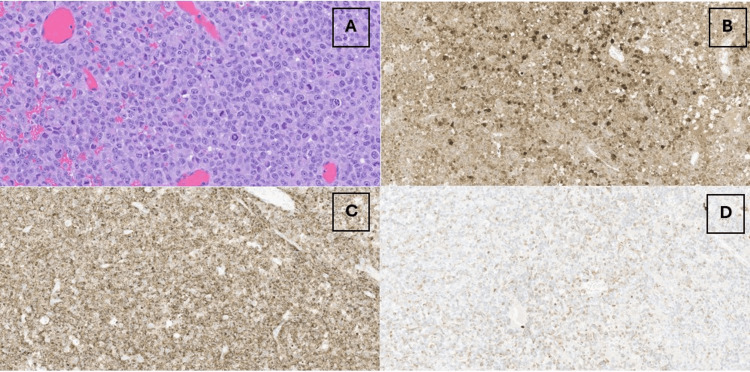 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Melanoma and MAPK Pathways · Virus-based gene therapy research
Introduction
Melanoma can metastasize to unique locations in the body, and metastatic lesions to the ovary are rare. Over the years, there have been several published case reports documenting melanoma metastasizing to the adnexa [1-3]. When present, the prognosis is very poor with a survival rate of around 5%-7% at five years [1]. Past guidelines recommend surgical management with total abdominal hysterectomy and bilateral salpingo-oophrectomy [3]. Advances in genetic testing and systemic therapy including immune checkpoint inhibitors have shown promise in not only developing target therapies but also improving survival for patients with metastatic melanoma. To add to the growing body of literature, we present a case of melanoma metastasizing to the ovary and will discuss the advances in systemic therapy as well as genetic testing for these patients.
Case presentation
A 48-year-old G2P2 patient presented to the gynecology service as a referral for management of an adnexal mass. She had previously presented to an outside hospital emergency room with left flank pain and hematuria. Her past medical history is significant for a superficial spreading melanoma excised from her back in 2016. She was recommended to have surveillance exams with dermatology; however, she was not adherent. Ultimately, she was lost to follow-up and presented eight years later with flank pain. Outside hospital imaging revealed a 6.7 cm left adnexal mass, 2.7 cm bladder mass, extensive osseous metastatic disease, and metastatic adrenal nodules with moderate to severe ascites (Figures 1-2). She was ultimately referred to Gynecologic Oncology for further management of her adnexal mass. An abdominal exam in the office was notable for a distended abdomen with a positive fluid wave.
CT-PET image (sagittal view)CT-PET: computed tomography-positron emission tomographyPET maximum intensity image on the left illustrates widespread metastases of the malignant melanoma, including the left adnexal mass pictured above
CT-PET image (axial view)CT-PET: computed tomography-positron emission tomographyThe overlay PET/CT scan on the right shows the left adnexal mass as well as free fluid in the pelvis in the axial view
She underwent a robotic-assisted total laparoscopic hysterectomy and bilateral salpingo-oophrectomy in order to debulk abdominal disease. Intraoperative laparoscopy images demonstrated an enlarged, blackened left adnexa (Figure 3). Copious bloody ascites were noted upon entry and evacuated prior to hysterectomy. Intraoperative frozen pathology revealed metastatic melanoma.
Intraoperative laparoscopy imageOn laparoscopy, the left adnexa was enlarged and edematous. Copious bloody ascites was evacuated prior to hysterectomy
Final histopathology confirmed metastatic melanoma involving both ovaries (Figure 4). Pelvic washings were significant for rare, atypical mesothelial cells. The uterus, cervix, and bilateral fallopian tubes were uninvolved by the tumor. Immunostains were strongly positive for S100 and HMB45 and were weakly focally positive for cytokeratin. She recovered well from the procedure and was referred to Clinical Genomics for genetic testing as well as her local medical oncologist for further treatment. She completed a comprehensive hereditary genetic testing panel that tested for numerous gene mutations associated with melanoma including CDK4 and BAP1, and her genetic testing demonstrated no pathologic mutations. She started on nivolumab and ipilimumab for systematic treatment and is being followed by her local medical oncologist.
Pathology of the left ovarian tumorThe left ovarian tumor was composed of pattern-less sheets of atypical polygonal cells with prominent nucleoli and numerous mitotic figures on hematoxylin and eosin (H&E) slide as seen throughout the entire slide (A). This image is set at 320X (A). Immunostains are strongly positive for S100 (B) and HMB45 (C), set at 130X. Aberrant keratin expression is apparent on pathology (D), which is also set at 130X. Aberrant keratin expression is well-known in melanoma
Discussion
Melanoma can be unpredictable in its disease spread. More commonly, melanoma can spread to the lungs, brain, liver, eyes, kidney, or bone. Prior case reports have been published documenting the novelty of metastatic lesions to the ovary [1-2]. There are some case reports documenting similar cases of melanoma presenting as metastatic years after initial diagnosis [1-2]. Our case shows the novel course of melanoma presenting years later with widespread disease noted in the ovaries, adrenal glands, and bone metastases. Ovarian metastases may either be asymptomatic or present with pelvic pain, such as in this patient. It can be challenging to differentiate primary ovarian malignancies from adnexal metastasis on imaging modalities such as ultrasound or CT scan, and immunohistochemical stains can provide definitive diagnosis [4]. S-100 is one of the most sensitive markers for melanoma; in addition, HMB-45 has been shown to be associated with melanosome production, which is seen in malignant melanoma [5-6].
Genetic testing has now proven to be beneficial for developing targeted cancer treatments. Genetic mutations associated with metastatic melanoma include B-Raf proto-oncogene (BRAF) mutations, specifically V600E mutations [7]. BRAF mutations are present in approximately 40%-50% of melanomas, and these mutations lead to constitutional activation of the MAP-K/EPK signaling pathway, which promotes cell proliferation and survival [7]. Other less common BRAF mutations include V600K, V600R, and non-V600 mutations [7]. The National Comprehensive Cancer Network (NCCN) as well as the American Society of Clinical Oncology recommend genetic testing for patients with unresectable or metastatic melanoma to guide treatment, especially if patients are found to be BRAF mutation carriers [8-9].
Additional genetic testing on tumor specimens aids in tailoring systematic treatment. Our pathology department performed additional genetic testing on the patient’s tumor, and two clinically relevant variants were detected. First, the patient’s tumor tested positive for a telomerase reverse transcriptase (TERT) mutation, specifically the C228T variant. TERT encodes telomerase reverse transcriptase protein, leading to increased telomerase activity, protein expression, and increased transcriptional activity [10]. TERT can be activated through multiple mechanisms in several cancer types including primary glioblastoma, bladder, and hepatocellular cancers [11]. TERT promotor mutations have been reported in approximately 22%-68% of melanoma cases and have been shown to be an adverse prognostic indicator [10,12]. Second, our patient’s tumor profile was significant for a neuroblastoma rat sarcoma viral oncogene homolog. NRAS encodes a specific protein in the family of Ras proteins, which mediates the transduction of growth signals [13]. Activating NRAS mutations produces oncogenic activation of downstream signaling pathways including Raf/MEK/ERK, causing cell growth, differentiation, and survival [13]. Just as with TERT-promoting mutations, activating NRAS mutations is associated with poor prognosis [14].
Prior to the advent of immune checkpoint inhibitors and modulators, metastatic ovarian melanoma was managed surgically with total abdominal hysterectomy with bilateral salpingo-oophrectomy [3]. Surgical excision can be offered for symptomatic management of pain, confirmation of diagnosis, or cytoreduction [3]. Systemic therapy is required for definitive cancer management. Targeted immunotherapy based on identifiable pathologic mutations such as BRAF V600 mutations has improved survival for patients with metastatic melanoma. Current cornerstone treatments for metastatic melanoma include immune checkpoint modulators, such as LAG3 inhibitors, pembrolizumab, nivolumab, and ipilimumab targeting CTLA-4, and PDL1 [9,15]. Nivolumab is a monoclonal antibody that targets PD1 and is used in combination with ipilimumab, which targets cytotoxic T-lymphocyte antigen-4 (CTLA-4) [16-18]. If BRAF mutation is present, utilizing BRAF inhibitors such as dabrafenib and vemurafenib and MEK inhibitors such as trametinib is the first-line treatment as research studies have shown that these treatments improve progression-free survival [19]. Mitogen-activated protein kinase (MEK) protein is critical in the RAS-RAF-MEK signaling pathway, and dysregulation has been seen in various cancer types like melanoma. Some investigative trials have shown that NRAS activating mutations may predict response to certain MEK inhibitors [16,20].
Conclusions
This case reflects the unique changes and advances in the management and treatment of metastatic melanoma. Prior to the advent of immunotherapy and targeted genetic testing, patients with metastatic melanoma would undergo surgical management with abdominal hysterectomy with bilateral salpingo-oophrectomy. Now, treatment guidelines have been updated to reflect the use of targeted immunotherapy to treat and improve patient outcomes for metastatic melanoma. While surgical excision can be offered for symptomatic management of abdominal or pelvic pain, confirmation of diagnosis, and cytoreduction, systematic therapy is often required for cancer treatment. Advances in genetic testing have made way for the development of novel targeted therapies based on oncogenes specific to melanoma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ovarian metastasis of a malignant melanoma: a case report J Gynecol Obstet Hum Reprod Mendel A Terzibachian JJ Aubin F Malicenco L Ramanah R Riethmuller D 4614624620172842812510.1016/j.jogoh.2017.02.016 · doi ↗ · pubmed ↗
- 2Malignant melanoma metastatic to the ovary Gynecol Oncol Piura B Kedar I Ariad S Meirovitz M Yanai-Inbar I 201205681998951480710.1006/gyno.1997.4919 · doi ↗ · pubmed ↗
- 3Malignant melanoma involving the ovary: a clinicopathologic and immunohistochemical study of 23 cases Am J Surg Pathol Gupta D Deavers MT Silva EG Malpica A 7717802820041516666910.1097/01.pas.0000126786.69232.55 · doi ↗ · pubmed ↗
- 4Diagnostic challenge for ovarian malignant melanoma in premenopausal women: primary or metastatic?World J Surg Oncol Sbitti Y Fadoukhair Z Kadiri H 65920112168290110.1186/1477-7819-9-65PMC 3157440 · doi ↗ · pubmed ↗
- 5Loss of S 100 antigenicity in metastatic melanoma Hum Pathol Aisner DL Maker A Rosenberg SA Berman DM 101610193620051615346610.1016/j.humpath.2005.07.010PMC 2656365 · doi ↗ · pubmed ↗
- 6HMB-45 staining in benign and malignant melanocytic lesions: a reflection of cellular activation Am J Dermatopathol Skelton HG 3rd Smith KJ Barrett TL Lupton GP Graham JH 543550131991172524510.1097/00000372-199113060-00004 · doi ↗ · pubmed ↗
- 7BRAF mutations in melanoma: biological aspects, therapeutic implications, and circulating biomarkers Cancers (Basel) Castellani G Buccarelli M Arasi MB 40261520233762705410.3390/cancers 15164026 PMC 10452867 · doi ↗ · pubmed ↗
- 8Melanoma J Natl Compr Canc Netw Coit DG Andtbacka R Anker CJ 3664001020122239319710.6004/jnccn.2012.0036 · doi ↗ · pubmed ↗