Epithelioid Hemangioendothelioma (EHE) Mimicking Mesothelioma: Case Presentation and Review
Kabir Grewal, Saivaroon Gajagowni, Elyse Lopez, Kayanaat Grewal, Son Viet Nguyen

TL;DR
A rare cancer called epithelioid hemangioendothelioma was mistaken for mesothelioma, highlighting the need for thorough testing and repeat biopsies for accurate diagnosis.
Contribution
The paper presents a case where EHE was misdiagnosed as mesothelioma, emphasizing the value of repeat biopsies and next-generation sequencing in atypical malignancies.
Findings
Pulmonary EHE in a 41-year-old female was initially misdiagnosed as mesothelioma.
Repeat biopsies and next-generation sequencing were crucial for correct diagnosis.
EHE's nonspecific imaging and overlapping pathology with other malignancies complicate early detection.
Abstract
Epithelioid hemangioendothelioma (EHE) is an extremely rare vascular sarcoma that can initially present with a myriad of symptoms anywhere in the body. Imaging findings are often nonspecific, and the pathology tends to have overlap with other malignancies. As a result, it can be quite difficult to suspect and diagnose EHE. We present a case of pulmonary EHE in a 41-year-old female with left pleural thickening and subclavian tumor thrombus who was initially misdiagnosed and treated as mesothelioma. This instance demonstrates the importance of maintaining a broad differential and the utilization of repeat biopsies and next-generation sequencing for questionable diagnoses of atypical malignancies.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
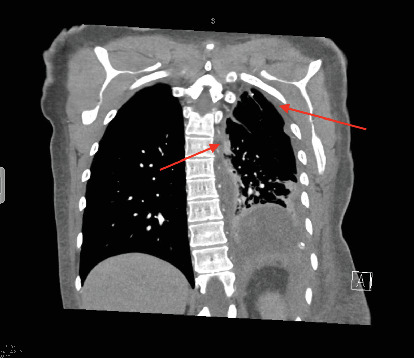 Figure 1
Figure 1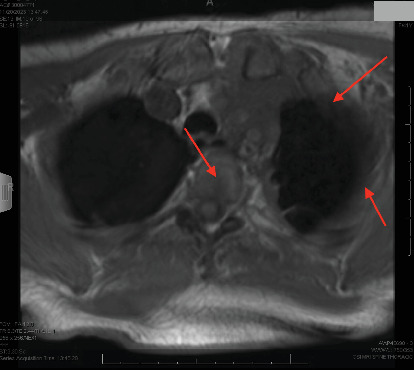 Figure 2
Figure 2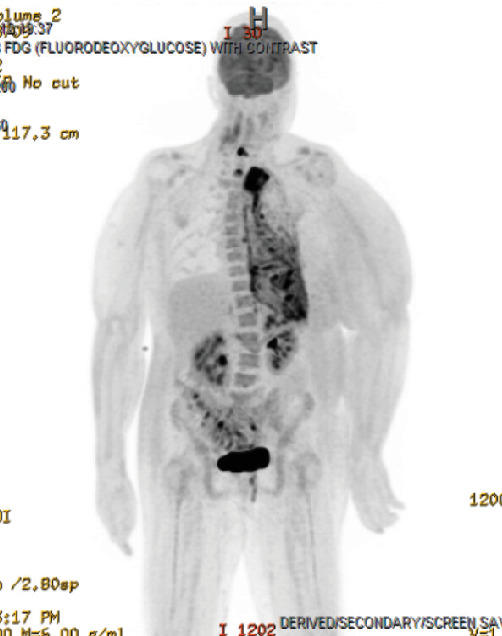 Figure 3
Figure 3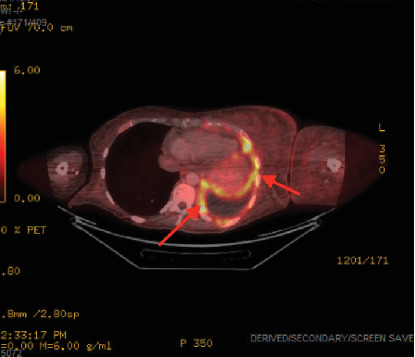 Figure 4
Figure 4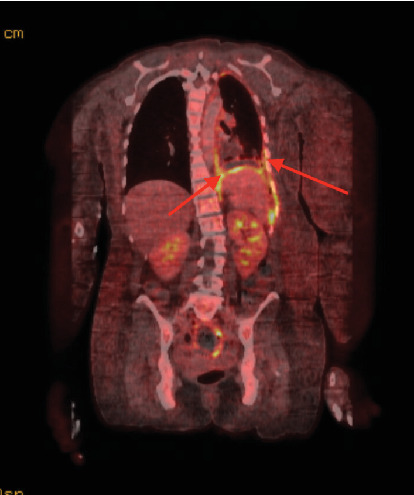 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Occupational and environmental lung diseases · Cardiac tumors and thrombi
1. Background
Epithelioid hemangioendothelioma (EHE) is a rare vascular sarcoma with low to moderate differentiation and potential metastatic ability. The incidence of the disease is 0.038/100,000 with an overall prevalence of < 1/1,000,000 [1]. The most commonly affected organs include the liver; bone; and rarely, the lung. There are fewer than 200 cases of primary pulmonary EHE published in the peer-reviewed literature [2]. Presentation can vary from asymptomatic patients with incidental findings on imaging to pleuritic chest pain, dyspnea, and cough [3]. Radiographic findings can include single or multiple lung masses distributed either unilaterally or bilaterally [4]. Disease rarity and nonspecific symptoms and imaging findings make diagnosing EHE difficult.
We present an informative case of pleural EHE that was initially misdiagnosed and treated as mesothelioma. The case highlights the diagnostic difficulty that EHE provides and emphasizes the importance of a broad differential for lung and pleural masses. Immunostaining of biopsy samples showed mixed results, requiring repeat biopsies and staining for official diagnosis.
2. Case Presentation
In this case, we focus on a 41-year-old female nonsmoker with no notable medical history, family history of cancer, or known asbestos exposure. She initially presented to her local hospital for a 3-month history of worsening dyspnea, flank pain, and left supraclavicular swelling. Imaging showed a subclavian tumor thrombus; left pleural effusion with diffuse nodular thickening; and mediastinal, supraclavicular, and hilar lymphadenopathy (Figure 1).
At the outside hospital, the patient underwent video-assisted thoracoscopic (VATS) biopsy with subsequent talc pleurodesis. Biopsy from the left supraclavicular lymph node was also obtained. Preliminary pathology results were nonspecific with initial staining grossly positive for WT1 and calretinin. The impression was “poorly differentiated spindle cell neoplasm.” This was presumed to be mesothelioma, and the patient soon underwent Cycle 1 of cisplatin/pemetrexed before being referred to our quaternary care cancer center for further workup and treatment.
3. Outcome and Follow-Up
The patient presented to our hospital 3 weeks after initial workup and 1 week after initial chemotherapy. She continued to endorse dyspnea, chest tightness, and back pain. MRI showed extensive left-sided pleural disease with osseous metastases to the spine and ribs (Figure 2). PET-CT showed extensive left-sided pleural thickening with soft tissue extension into the neck and involvement of the left brachiocephalic and jugular veins (Figures 3, 4, and 5). A CT-guided percutaneous left pleural biopsy (core + FNA) was performed.
Immunohistochemical studies were grossly negative for cytokeratin, calretinin, and WT1, which was inconsistent with the original mesothelioma diagnosis. Repeat pathology staining was positive for ERG, CD31, and nuclear CAMTA-1. After extension discussion between pathology and the sarcoma team, a diagnosis of EHE was established. The detection of a WWTR1:CAMTA-1 fusion alteration on gene sequencing helped confirm EHE.
The patient was started on a chemotherapy regimen of gemcitabine and docetaxel for a goal of 10 total cycles of 21 days each. After six cycles, surveillance imaging shows no further disease progression. Due to pancytopenia, Cycle 7 was delayed and the patient was put on a treatment break with plans to resume chemo in the future pending follow-up.
4. Discussion
We present a case of a 41-year-old female with EHE involving the pleura. Literature review shows 58 published cases of pleural EHE (Table 1). Sixty-four percent of the patients were male, and the average age at diagnosis was 50. Thirty-three cases (57%) are confirmed to be dead, with 22 of the 33 dying within 12 months of diagnosis. Pleural involvement is associated with poor prognosis [44]. Treatment modalities varied, with 11 (19%) receiving only surgical interventions, 15 (26%) receiving only chemotherapy, 10 (17%) receiving a combination of surgery/chemotherapy/radiation, and 22 (38%) not receiving any form of treatment or not having data available.
Diagnosis of pulmonary EHE is complicated by a lack of specific symptoms. The most common initial presentation among published cases is pleuritic chest pain (43%), with other common symptoms including dyspnea and cough (Table 1). Imaging findings are nonspecific and often show pleural thickening with effusions. As in our case, EHE can often be misdiagnosed as mesothelioma [15]. This emphasizes the importance of maintaining a broad differential for pleural thickening including inflammation, infection, mesothelioma, and EHE.
Biopsy remains the gold standard for diagnosing and differentiating between EHE and mesothelioma. EHE classically stains positive for endothelial and vascular markers including CD31, CD34, and ERG [1]. More recently, positive immunohistochemical staining for nuclear CAMTA-1 is found to be specific for EHE [41, 45]. On the other hand, mesothelioma classically stains positive for calretinin, CK5 or CK5/6, WT1, and D2-40 [41].
Preliminary biopsy results for our patient were positive for WT1, calretinin, and D2-40, leading to the initial diagnosis and treatment of mesothelioma. However, repeat biopsy showed immunostaining positive for ERG, CD31, and nuclear CAMTA-1 and negative for WT1, calretinin, and CK5/6, consistent with EHE. This diagnosis was only confirmed after next-generation sequencing showed a WWTR1:CAMTA1 fusion alteration, a classic finding in EHE [45]. The mixed results in this case showcase that biopsies may not be definitive, especially when samples show such conflicting results. Next-generation sequencing can be utilized to differentiate between mimicking diseases on a genomic level.
Due to the rarity of EHE, treatment for the condition varies based on disease site. Early cases of EHE were treated with surgical excision, although often unsuccessfully. More recently, the condition has been treated with chemotherapy, typically carboplatin/etoposide. Due to the rarity and complex nature of EHE, there has been a push to establish global standards of treatment [1]. It is recommended for EHE to be managed at dedicated sarcoma centers. The preferred treatment for unifocal EHE, defined as a localized tumor, is surgery, with an expected cure rate of 70%–80% for negative margins. Other procedures such as pleural stripping or pneumonectomy should be considered individually in cases of pulmonary EHE [44]. Radiation is recommended as an adjunct to surgery, not alone. If there is serosal involvement or metastatic disease, patients are candidates for systemic therapy, although a standard regimen has not been established. Retrospective data suggests that the highest clinical activity is seen with mTOR inhibitors with a progression-free survival (PFS) and overall survival in the range of 1 year and 2 years, respectively, and ∼10% of patients having even longer PFS [1].
We present a rare case of EHE involving the pleura that was misdiagnosed as mesothelioma. This case emphasizes the utility of repeat biopsies to confirm results when the diagnosis is unclear or when the clinical presentation is atypical for the suspected disease (i.e., mesothelioma in a young patient without asbestos exposure). Next-generation sequencing can be useful to confirm disease on a genomic level. Specialty cancer centers can be quite beneficial in establishing and treating ultrarare malignancies like EHE. Further research into establishing localized and systemic treatment guidelines for EHE are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stacchiotti S. Miah A. B. Frezza A. M. Epithelioid hemangioendothelioma, an ultra-rare cancer: a consensus paper from the community of experts ESMO Open 20216310017010.1016/j.esmoop.2021.10017034090171 PMC 8182432 · doi ↗ · pubmed ↗
- 2Cazzuffi R. Calia N. Ravenna F. Primary pulmonary epithelioid hemangioendothelioma: a rare cause of PET-negative pulmonary nodules Case Reports in Medicine 20112011626267410.1155/2011/2626742-s 2.0-8487178308021869893 PMC 3160144 · doi ↗ · pubmed ↗
- 3Travis W. D. Tazelaar H. D. Miettinen M. Travis W. D. Brambilla E. Muller-Hermelink H. K. Harris C. C. Epithelioid haemangioendothelioma/angiosarcoma World Health Organization Classification of Tumours, Pathology and Genetics: Tumours of the Lung, Pleura, Thymus and Heart 2004 Lyon IARC Press 9798
- 4Amin R. M. S. Hiroshima K. Kokubo T. Risk factors and independent predictors of survival in patients with pulmonary epithelioid haemangioendothelioma. Review of the literature and a case report Respirology 200611681882510.1111/j.1440-1843.2006.00923.x 2-s 2.0-3375008695217052315 · doi ↗ · pubmed ↗
- 5Stout A. P. Hemangio-endothelioma: a tumor of blood vessels featuring vascular endothelial cells Annals of Surgery 1943118344546410.1097/00000658-194309000-0001417858281 PMC 1617738 · doi ↗ · pubmed ↗
- 6Yousem S. A. Hochholzer L. Unusual thoracic manifestations of epithelioid hemangioendothelioma Archives of Pathology & Laboratory Medicine 198711154594633105516 · pubmed ↗
- 7Bevelaqua F. A. Valensi Q. Hulnick D. Epithelioid hemangioendothelioma Chest 198893366566610.1378/chest.93.3.6652-s 2.0-00239724793342681 · doi ↗ · pubmed ↗
- 8Lin B. T. Colby T. Gown A. M. Malignant vascular tumors of the serous membranes mimicking mesothelioma. A report of 14 cases The American Journal of Surgical Pathology 199620121431143910.1097/00000478-199612000-000012-s 2.0-00298010078944035 · doi ↗ · pubmed ↗