Role of Adjuvant Radiotherapy in Sweat Gland Carcinoma: A Case Report and Literature Review
Arit Bhattacharjee, Debarshi Lahiri, Ranti Ghosh, Debanjan Chakraborty

TL;DR
This paper discusses a case of sweat gland carcinoma and reviews the potential benefits of adjuvant radiotherapy in managing this rare and aggressive skin cancer.
Contribution
The paper presents a case report and literature review highlighting the possible role of adjuvant radiotherapy in sweat gland carcinoma.
Findings
Adjuvant radiotherapy may improve local and regional control in sweat gland carcinoma with high-risk features.
Diagnosis of sweat gland carcinoma is challenging due to clinical and histopathological variability.
There is a lack of consensus guidelines for adjuvant treatment of sweat gland carcinoma.
Abstract
Sweat gland carcinoma (SGC) is a rare type of malignant adnexal tumours of the skin (MATS). It has potential for local infiltration, regional nodal involvement, and distant metastasis. Wide local excision with regional lymph nodal dissection is the mainstay of treatment and there are no consensus guidelines for adjuvant treatment. We present a case report of a gentleman, suffering from SGC in the left lumbar region with axillary nodal metastasis, presenting with a longstanding skin nodule, with recent spurt in growth and ulceration over it. He was treated with wide local excision of the lesion and left axillary nodal dissection. Postoperative histopathology and immunohistochemistry confirmed the diagnosis of SGC. He received adjuvant radiotherapy to primary and nodal sites due to the presence of high-risk features. Diagnosis of SGC is very challenging due to clinical variation,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1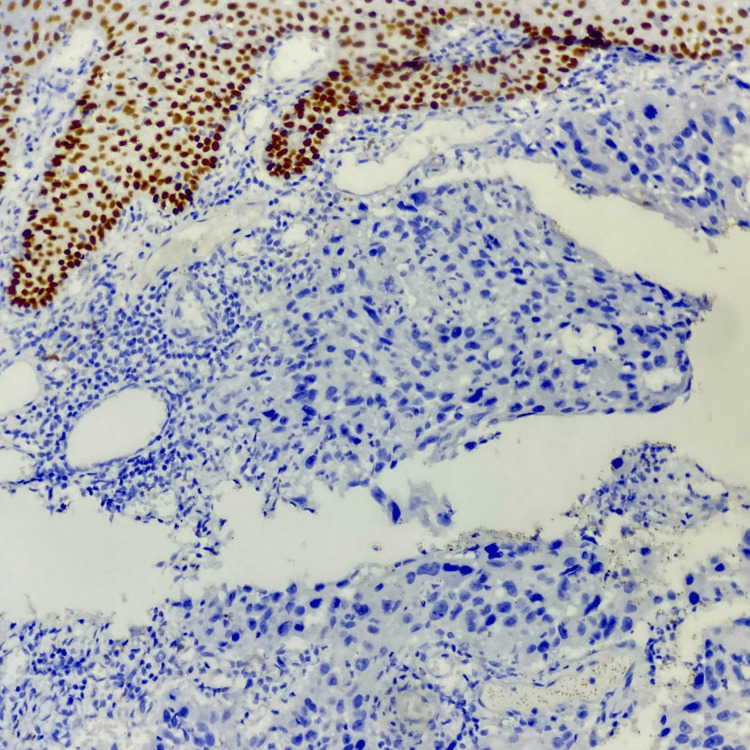 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Salivary Gland Tumors Diagnosis and Treatment · Vascular Tumors and Angiosarcomas
Introduction
Sweat gland carcinoma (SGC) is a very rare malignant adnexal tumour of the skin (MATS), comprising less than 0.01% of cutaneous cancers [1]. Arising from the pilosebaceous unit and eccrine and apocrine sweat glands, SGC usually occurs in the fifth to seventh decades of life, with similar gender preponderance. The most common sites are the head and neck region, axilla, inframammary region, perineum, and lower extremities [2]. Starting as an asymptomatic nodule, it often shows aggressive growth kinetics later - also local invasiveness, lymphatic involvement, and even distant metastases [3]. Clinically, variable presentation, accidental discovery during histopathological examination (HPE), and furthermore complex immunohistochemistry (IHC) profiling makes the diagnosis challenging. The paucity of relevant literature makes the management of SGC even more difficult. Surgical excision with regional lymph node dissection (LND) is standard treatment, but the role of adjuvant treatment is not very clear due to limited evidence.
Here, we present a case of SGC of the left lumbar region revealing challenges in diagnosis and management, emphasizing the role of adjuvant treatment in tumors having a higher risk of locoregional relapse.
Case presentation
A 69-year-old gentleman with hypertension and ischemic heart disease, in the month of June 2023, presented with a persistent asymptomatic nodule, in the left lumbar region, which was gradually progressing in size since the last three months. Clinically, the lesion was 4 x 3 cm in size, hard, painless, and ulcerated and had ill-defined margins (Figure 1), suspicious for a cutaneous malignancy.
Clinical photograph of the skin lesion
After routine lab investigations, a positron emission tomography/computed tomography (PET-CT) scan done on September, 2023, showed FDG avid cutaneous thickening in left lumbar region approximately 3.1 cm anteroposteriorly, 1.7 cm thick, SUV max 12.1, with an 8 x 10 mm sized hypermetabolic left axillary lymphadenopathy, SUV max 8.9, which stages the tumor to be cT2N1M0 (Stage III, as per AJCC TNM staging for non-melanoma skin cancers). FNAC from both primary tumor and node showed squamous cell carcinoma (SCC).
The patient underwent wide local excision (WLE) of the lesion and rotational fasciocutaneous flap reconstruction, with ipsilateral axillary node dissection in the last week of September 2023. Surgical HPE showed SCC, tumor size 3 x 3.2 cm, Grade 3, with lymphovascular invasion (LVI) and perineural invasion (PNI) present. Overlying ulcerated skin and subcutaneous tissue infiltration up to 1.3 cm depth was noted. All surgical margins were free of tumour. Four out of 23 axillary nodes (4/23) were involved by carcinoma without any extra-nodal extension (ENE). IHC showed positivity for CK7, CK5/6, and P63 (Figure 2); negative for CK20, P40, and Ki67 5% reported as MATS consistent with SGC.
Immunohistochemistry slide showing p63 positivity
We discussed the case in the Multidisciplinary Tumour Board on December 2023 due to a surprising change in histopathology. Another HPR review confirmed the diagnosis of SGC. In view of the high-grade, positive LVI and PNI, extensive lymph nodal involvement, and depth of invasion >1 cm, the patient was treated with adjuvant radiotherapy to both the primary site and axilla, to reduce the risk of the locoregional relapse.
He received external beam radiation (EBRT), starting from the first week of January 2024 till the third week of February 2024, to a dose of 60 Gy in 30 fractions to the primary tumor bed with adequate margins, for including subclinical microscopic disease (tumor bed identified by scar localization during planning CT by radio-opaque material on skin scar and pre-surgical images) using electrons of 10 MeV energy, prescribed at depth of 3 cm for optimal coverage, and a 1 cm bolus to ensure adequate skin doses. Left axillary nodes of level I-III were irradiated, to a dose of 50 Gy in 25 fractions using volumetric modulated arc therapy (VMAT), to minimize normal tissue toxicities, ensuring limited doses as per tolerance of critical organs at risk - left lung, heart, left humeral head, neurovascular bundle, and spinal cord.
EBRT was completed in February 2024 over a period of six weeks with only Grade I acute dermatitis. The patient is still alive and disease free nine months since the RT conclusion, pursuing clinical follow up every three to four months now, with good functional and psychosocial quality of life (QoL).
Discussion
Due to the limited literature, variable presentation, difficult pathological classification, diagnosis, and treatment, there is no consensus guideline for management of SGC.
After the pathological classification of SGC by Berg in 1968 [4], the WHO 2018 classification divided SGC into 10 subtypes: adnexal adenocarcinoma, syringocystadenocarcinoma papilliferum, clear cell hidradenocarcinoma, porocarcinoma, mucinous carcinoma, and others [5]. Traditionally, SGCs are divided into apocrine and eccrine, sometimes having both features. There is insufficient evidence to suggest any impact of tissue origin or WHO classification on management [6-7]. Occurring in the fifth to seventh decades of life, with similar gender preponderance, most usual sites of SGC are the head and neck, followed by the lower limbs. The pattern of relapse is mostly regional nodes, followed by the lung [2].
In our patient, SGC was present on the left lumbar region, an uncommon site, and it spread to the axillary nodes without any abdominal-pelvic nodal disease. In absence of obvious histopathology, it is very difficult to differentiate from benign or other analogous malignant counterparts, so very often, it can surprise clinicians. IHC with expressions of P53, P63, and CK7 is very suggestive of SGC [8]. Similarly, in our patient, initially, the clinicoradiological, FNAC, and histopathology of the operative specimen suggests SCC of the skin, whereas the aforesaid IHC results changed the diagnosis to SGC.
The recommended treatment of SGC is full-thickness WLE with at least 1-2 cm margin, preferably by Mohs micrographic surgery, which shows the lowest rate of local relapse in aggressive skin malignancies [9-10]. Upfront 50% risk of lymph nodal involvement dictates the role of elective LND in SGC, even in clinically node negative status, keeping in mind the role of sentinel lymph node mapping [11]. Although the literature is scarce, the role of radiotherapy in reducing the rates of locoregional relapse (which are higher otherwise, up to 50%) is of paramount importance [12]. Pathological features such as dermal LVI, PNI, deep infiltration, positive resection margins, anaplasia, and ENE may identify a higher risk of recurrence, and adjuvant EBRT is clinically meaningful there, up to 60-70 Gy doses, with good local control, supported by recent evidences [6,13]. Definitive EBRT doses up to 60-70 Gy radiation in the head and neck SGC improved local control greatly [14].
In our patient, as HPE showed four high-risk features (positive LVSI, PNI, high grade, and deep tissue infiltration), adjuvant RT was delivered up to 60 Gy dose to the primary disease and 50 Gy to the axillary nodes. No dose escalation was done due to clear margins and no ENE. The usage of electrons helped to achieve complete target coverage, dose distribution, and proper reproducible set-up during treatment. The VMAT technique for the axilla maximized normal tissue sparing.
Although robust evidences are unavailable, multiple chemotherapeutic agents such as 5-fluorouracil, doxorubicin, cyclophosphamide, paclitaxel, mitomycin C, vincristine, and cisplatin had been used in SGC, mostly with short-term response and potential toxicity. Another case report showed a patient of metastatic SGC, treated with doxorubicin, mitomycin C, vincristine, and cisplatin, who achieved complete response, sustaining for 1.5 years. Docetaxel has also been used with a good response rate [15].
Conclusions
SGC is a rare aggressive cancer, belonging to the malignant skin adnexal tumour group. Multifaceted clinical presentation and pathological complexity makes the diagnosis difficult, making IHC so crucial for accurate characterisation. Mohs micrographic surgery followed by risk-adapted adjuvant EBRT is the preferred treatment approach for optimal outcome in localized SGC. No standard guideline is available for the use of chemotherapy and Immunotherapy. Furthermore, prospective studies are necessary to develop consensus treatment guideline.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary cutaneous apocrine carcinoma: case report and literature review Indian J Pathol Microbiol Chadha S Kumar R Singhal S Ruhela S 1831856420213343343810.4103/IJPM.IJPM_341_19 · doi ↗ · pubmed ↗
- 2Porocarcinoma; presentation and management, a meta-analysis of 453 cases Ann Med Surg (Lond) Salih AM Kakamad FH Baba HO 74792020172872121410.1016/j.amsu.2017.06.027PMC 5499034 · doi ↗ · pubmed ↗
- 3Metastatic sweat gland adenocarcinoma: a clinico-pathological dilemma World J Surg Oncol Chintamani Chintamani Sharma R Badran R Singhal V Saxena S Bansal A 13120031292153710.1186/1477-7819-1-13PMC 184447 · doi ↗ · pubmed ↗
- 4Tumors of sweat glands Am J Pathol Gates O Warren S Warvi WN 591631191943 https://pubmed.ncbi.nlm.nih.gov/19970710/19970710 PMC 2033085 · pubmed ↗
- 5Mucinous sweat gland adenocarcinoma of the eyelid - current knowledge of a rare tumor Orbit Segal A Segal N Gal A Tumuluri K 3343402920102115857410.3109/01676830.2010.516469 · doi ↗ · pubmed ↗
- 6Case report: case report and literature review: treatment of sweat gland carcinoma Front Oncol Dai Y Feng J Zhou X 10919341320233675615410.3389/fonc.2023.1091934 PMC 9900132 · doi ↗ · pubmed ↗
- 7Microcystic adnexal carcinoma: report of 13 cases and review of the literature Dermatol Surg Snow S Madjar DD Hardy S 4014082720011129871610.1046/j.1524-4725.2001.00208.x · doi ↗ · pubmed ↗
- 8Current management approach to hidradenocarcinoma: a comprehensive review of the literature Ecancermedicalscience Soni A Bansal N Kaushal V Chauhan AK 517920152581505910.3332/ecancer.2015.517PMC 4370612 · doi ↗ · pubmed ↗