Plasma Amino Acid Profiles and Clinical Outcome in Patients with Traumatic Brain Injury: A Study Protocol
Alireza Gheflati, Mostafa Shahraki Jazinaki, Mahlagha Nikbaf-Shandiz, Pegah Rahbarinejad, Hamid Rezaee, Saeid Eslami, Majid Khadem-Rezaian, Alireza Sedaghat, Mohsen Nematy, Mahdi Shadnoush, Ali Jafarzadeh Esfehani, Fatemeh Keyfi, Zachary S. Clayton, Abdolreza Norouzy

TL;DR
This study aims to analyze how plasma amino acid levels in traumatic brain injury patients relate to their clinical outcomes over time.
Contribution
The study introduces a longitudinal approach to assess amino acid profiles and their correlation with TBI recovery metrics.
Findings
Plasma amino acid concentrations will be measured at multiple time points in TBI patients.
Clinical outcome parameters like APACHE II and SOFA scores will be correlated with amino acid levels.
Results may guide future treatment strategies involving amino acid supplementation for TBI.
Abstract
Background: The most common cause of cognitive and behavioral impairments, disability, and mortality around the world is traumatic brain injury (TBI). The imbalance between cerebral metabolism and inflammation leads to protein breakdown and induces altered concentrations of serum amino acids, which can serve as a diagnostic and prognostic sign in patients with TBI. This study aimed to examine the alterations in plasma amino acid concentrations and their relation to clinical outcomes in patients with TBIs.Materials and Methods: At completion, this study will assess 107 patients suffering from TBI aged 18 to 65. Plasma amino acid concentrations, anthropometric indices, and clinical outcome parameters including Acute Physiology and Chronic Health Evaluation (APACHE) II, Sequential Organ Failure Assessment (SOFA), Nutrition Risk in the Critically ill (Nutric) score, Glasgow coma scale…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
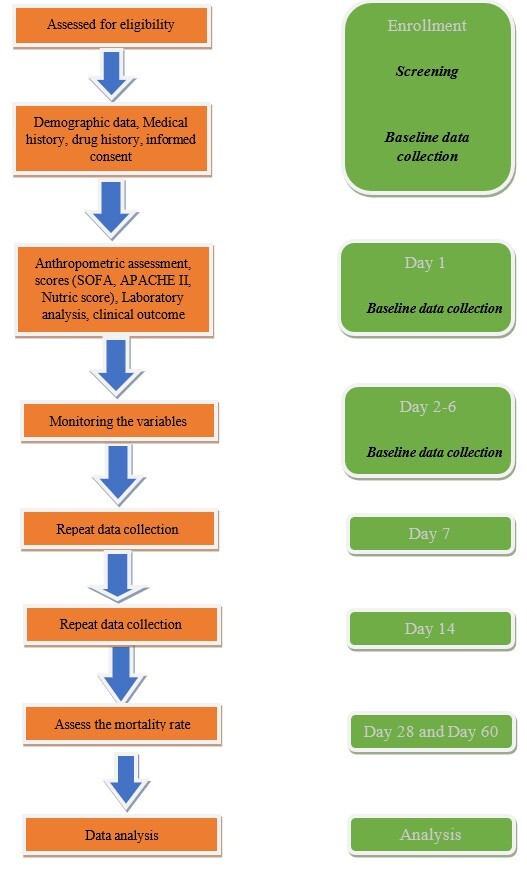 Figure-1
Figure-1| Time Point | Days | |||||
| 0 | 7 | 14 | 28 | 60 | ||
| Enrolment | ||||||
| Eligibility screening | * | |||||
| Informed consent | * | |||||
| Medical interview | * | |||||
| Blood collecting | * | * | * | |||
| Assessment | ||||||
| Demographic | * | |||||
| Laboratory assessment (20 types of plasma amino acid) | * | * | * | |||
| Clinical outcome: GCS, vital signs, electrolyte balance | ||||||
| Anthropometric measurements | Weight | * | * | * | ||
| Height | * | * | * | |||
| BMI | * | * | * | |||
| Fat mass | * | * | * | |||
| Lean body mass | * | * | * | |||
| MAC | * | * | * | |||
| SOFA | * | * | * | |||
| APACHE II | * | * | * | |||
| Nutric score | * | * | ||||
| GOS | * | * | ||||
| Mortality status | * | * | * | |||
| Days of hospital stay | * | * | * | |||
| Dietary intake | ||||||
| Need mechanical ventilator | * | * | * |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Cardiac Arrest and Resuscitation · Traumatic Brain Injury Research
Introduction
Traumatic brain injury (TBI) is the leading cause of cognitive and behavioral impairments, disability, and mortality around the world [1]. As reported by the Global Burden of Diseases (GBD), TBI led to 8.1 million (95% UI 6·0-10·4 million) years of life lost (YLLs) in 2016 [2]. TBI can contribute to a variety of pathophysiological states [3]. For example, TBI can lead to blood-brain barrier rupture, neuroinflammation, neurodegeneration, and ischemic injury, which induce significant changes in cerebral metabolism and exacerbate systemic and neurological inflammation [4].
The concomitant imbalance of cerebral metabolism and inflammation results in protein breakdown, which alters plasma amino acid concentrations [5]. Therefore, measuring amino acid concentrations in patients with TBI is valuable for diagnostic and prognostic purposes [6].
Previous studies have shown that brain tissue after TBI contained up to 50-fold more glutamate and aspartate [7]. Serine, taurine, and alanine levels in the serum also decreased significantly 24 hours after TBI but returned to pre-injury levels after four days [8]. TBI reduces serum glycine levels and disturbs redox balance, ultimately leading to neuronal death [8]. Patients with TBI also had lower levels of branched-chain amino acids (BCAAs) including leucine, isoleucine, and valine relative to healthy individuals, likely as a result of the metabolic cascade that developed after the injury [9].
Alternatively, Intensive care unit (ICU) length of stay (LOS) and ventilator dependency are associated with plasma taurine concentration [10]. Furthermore, low taurine levels were associated with high blood lactate, which may indicate a state of heightened metabolic demand [10]. A better understanding of changes in amino acid profiles among patients with TBI will help clinicians more accurately estimate amino acid requirements and provide optimal nutritional support [11].
To the best of our knowledge, prior studies have only examined the alterations of select amino acids after TBI. No studies have comprehensively assessed plasma amino acid concentrations in patients with TBI.
This study will be the first to comprehensively assess plasma amino acid levels in patients with TBI and relate these values to clinical outcomes including Glasgow coma scale (GCS), mechanical ventilator duration, ICU discharge time, and mortality rate. The results of this study will inform whether particular amino acid profiles are useful biomarkers for TBI.
Materials and Methods
**
**:
After the completion of this study, 107 individuals with TBI hospitalized in the ICU will be recruited. Participants will be selected according to inclusion and exclusion criteria by a qualified neurosurgeon from adult trauma wards referred to Shahid Kamyab, Taleghani, and Shahid Hasheminejad hospitals in Mashhad, Iran.
This project was initiated in September 2022 and will likely be completed in July 2023. The details of this study protocol are depicted in the flow diagram (Figure-1).
- Study Design and Setting
Upon completion of this study, a total of 107 patients who have been diagnosed with subarachnoid hemorrhage (SAH), subdural hemorrhage (SDH), epidural hemorrhage (EDH), brain edema, intracerebral hemorrhage (ICH), or intraventricular hemorrhage (IVH) will be recruited by the neurosurgeon. According to inclusion and exclusion criteria, patients will be chosen.
- Eligibility Criteria
The inclusion criteria for this study will be a) patients with TBI aged 18 to 65 years; b) being admitted to a neurocritical care unit with any type of TBI diagnosis; c) moderate to severe TBI (7≤GCS≤12), and e) signing the informed consent form by the patient or family members.
The exclusion criteria will be: a) severe and active bleeding; b) taking inotropic and corticosteroid medications; c) history of any kind of autoimmune, cancer, and metabolic diseases; d) refusal to continue the study by the patient, parents, or relatives members; e) acute or chronic liver failure; f) pregnancy and breastfeeding; g) chronic renal failure, and h) acute renal failure requiring dialysis.
- Ethics Approval
The Medical Ethics Committee of the Mashhad University of Medical Science approved this longitudinal study protocol. (IR.MUMS.MEDICAL.REC.1400.589).
- Study Assessment
4.1. Clinical Outcome Assessment
Clinical measurement tools including GCS, Sequential Organ Failure Assessment (SOFA), Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Nutrition Risk in the Critically ill (Nutric) score, ICU discharge time, and mechanical ventilator duration will be recorded by a nutritionist at baseline, middle (7th day) and end of the study (14th day). Moreover, 28-day and 60-day in-hospital and out-of-hospital mortality will be recorded during the study. Demographic data, social and medical background (current employment, place of residence, marital status) will be collected by a neurosurgeon.
4.2. Anthropometric Assessment
Anthropometric parameters will be measured at baseline, 7th day, and 14th day by a well-trained nutritionist. A bed scale (Balas Company) will be used to measure body weight, also the ulnar length will be used to estimate height. The mid-arm circumference will be measured at the mid-point between the elbow and apex of the shoulder by a non-stretched tape. Fat and fat-free masses will be measured by bioelectrical impedance analysis (s10, in Body Company, South Korea). The body mass index will be calculated based on the ratio of the weight in kilograms to the square of the height in meters. All anthropometric indices will be collected by a trained nutritionist. The study timeline is demonstrated in Table-1.
4.3. Laboratory Assessment
Five milliliters (5 cc) of venous blood samples will be taken in EDTA-containing tubes at baseline, 7th day, and 14th day, at ~7:00 am, for assessment of plasma amino acids. Blood samples will be centrifuged immediately to separate the plasma sample from the whole blood. The plasma will be stored at -20 °C after being divided into aliquots and placed in microtubes. The samples will then be placed in a freezer at -80 °C to be analyzed for the concentration of 18 types of plasma amino acids (glycine, glutamic acid, valine, asparagine, lysine, serine, glutamine, isoleucine, threonine, arginine, alanine, tyrosine, methionine, tryptophan, phenylalanine, aspartic acid, leucine, and histidine) and two metabolites of arginine (ornithine and citrulline). After precolumn derivatization with o-phthalaldehyde (OPA), the concentrations of plasma amino acids will be measured using reverse-phase high-performance liquid chromatography (RP-HPLC) on a C18 column with a fluorescence detector. Briefly, 100 µL of plasma will be mixed with 200 µL of the internal standard. The tubes will be centrifuged for 5 minutes at 12000 rpm. Twenty µL of supernatant will be added to 100 µL buffer solution before the addition of 20 µL of OPA reagent. Following, samples will be blended with 200 µL of distilled water, and 20 µL of the mixture will be injected into the HPLC system (Agilent Technologies 1260 infinity series, USA) for analysis.
- Power Calculation and Sample Size Estimates
The sample size was computed based on Oudemans-van Straaten et al. (2010) [12] based on 5% Type I error (α=0.05), 0.093 as effect size (d=0.093) (96 persons). Finally, the sample size was increased to 107 patients to account for 10% attrition.
- Statistical Methods
To assess the normality of quantitative variables, the Kolmogorov-Smirnov test will be performed. For normally distributed data, the quantitative data will be presented as mean ± standard deviation (SD), and for variables with non-normal distribution, including median and interquartile range (IQR). The qualitative data will be demonstrated in the form of frequency and percentage. Quantitative variables will be compared between the survived and deceased groups using the student t-test or the Mann-Whitney test. The chi-square or Fisher’s exact test will be used to analyze the comparison of qualitative variables between the surviving and deceased patients. The relation among quantitative variables will be investigated by Pearson or Spearman correlation coefficient. The Kaplan-Meier test will be conducted to compare the survival rate between amino acid-sufficient and deficient patients based on the log-rank test of survival time. The test results will be considered statistically significant when the P-value is less than 0.05. The data will be analyzed using the SPSS Software Version 23 (IBM Inc, Chicago, IL, USA).
Discussion
Until now, the relation of select amino acids with mortality and several clinical outcomes have been discussed separately, however, there is little information available regarding the prevalence of all essential and non-essential amino acid deficiencies and the relation between amino acid profiles and main clinical parameters among patients with TBI.
Physical damage to brain tissue caused by TBI could result in brain dysfunction [13] including ischemia, glutamate excitotoxicity, changes in neurotransmitter function, neuroinflammation, altered brain metabolism, a heightened pro-inflammatory state, and protein breakdown [14]. Previous studies have indicated protein catabolism/anabolism imbalance in patients with TBI [15][16], and have identified serum amino acid concentrations as the main predictor of mortality in patients with acute TBI. Recently, serum amino acid levels were shown to be associated with brain tissue concentrations, and as such, serum amino acids may be prognostic indicators of TBI [6]. For example, increased glutamate receptor activation and redox imbalance are observed in patients with TBI, which can lead to cell death within the brain and ultimately neurological dysfunction [17][18].
Studies indicated that the glutamate toxicity side effects can be reversed by elevated levels of glycine, taurine, and serine in brain tissue through their role in mitochondrial function regulation [18][19]. Moreover, glycine levels in brain tissue and serum glycine concentrations in patients with TBI may be linked to the pathology of oxidative stress caused by TBI, as it is a small neutral amino acid that could easily diffuse through a disrupted blood-brain barrier [20]. Alternatively, increased glycine levels in brain tissue and decreased serum glycine levels after TBI may be due to the antioxidant property of this amino acid. In addition, glycine and serine interact with glutamate receptors [21]. Moreover, glycine and cytosine are precursors of glutathione synthesis, a primary antioxidant system, and increasing levels of these amino acids may be a means to reduce TBI-mediated oxidative stress [22]. The critical amino acids serine, glycine, and alanine produce glucagon, which is essential in TBI-stimulated glycogen metabolism [23]. Some studies have observed reduced proline levels in patients with TBI [24], suggesting that proline levels may be linked to TBI pathology, whereas other investigations have shown anti-inflammatory effects of proline in the cerebral cortex [25]. An experimental study reported low serum citrulline levels in a model of severe TBI in rats, but the exact mechanism mediating this response was unclear [21]. On the other hand, there is evidence that L-citrulline has a protective effect on cerebral arteries [26]. The concentration of circulating amino acids is likely to be considered a potential prognostic marker for patients with TBI, as there is a negative nitrogen balance in TBI patients. The importance of the relation between plasma amino acid levels and mortality and other paraclinical biomarkers has been mentioned in previous investigations. Past studies showed a possible association between the higher concentrations of some amino acids like homocysteine and magnetic resonance imaging (MRI) finding as silent brain infracts, atrophy of the brain, white matter hyperintensity, elevated risk of subclinical stroke, and other neuropsychiatric diseases [27][28][29][30]. On the other hand, according to Rahmani et al. a rise in homocysteine levels was significantly associated with an increase in the rate of mortality and a significant decrease in GCS [31]. Also, based on the study of Vuille-Dit-Bille et al. an increase in intracranial pressure (ICP) following TBI is associated with a rise in leucine and isoleucine levels [32]. In addition, low plasma taurine is correlated with a longer mechanical ventilation dependency and length of ICU stay [10]. Therefore, it can be expected that amino acid levels can be a good predictor of mortality and other paraclinical data.
Acknowledgements
The Mashhad University of Medical Sciences will provide financial support for this study.
Conflict of Interest
No conflicts of interest were declared by the authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dewan MC Rattani A Gupta S Baticulon RE Hung Y-C Punchak Metal Estimating the global incidence of traumatic brain injury J Neurosurg 2018130410809710.3171/2017.10.JNS 1735229701556 · doi ↗ · pubmed ↗
- 2James SL Theadom A Ellenbogen RG Bannick MS Montjoy-Venning W Lucchesi L Retal Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016 Lancet Neurol 2019181568710.1016/S 1474-4422(18)30415-0PMC 629145630497965 · doi ↗ · pubmed ↗
- 3Andriessen TM Jacobs B Vos PE Clinical characteristics and pathophysiological mechanisms of focal and diffuse traumatic brain injury J Cell Mol Med 2010141023819210.1111/j.1582-4934.2010.01164.x PMC 382315620738443 · doi ↗ · pubmed ↗
- 4Genton L Pichard C Protein catabolism and requirements in severe illness Int J Vitam Nutr Res 201181214314310.1024/0300-9831/a 00005822139565 · doi ↗ · pubmed ↗
- 5Stocchetti N Maas AI Traumatic intracranial hypertension N Engl J Med 20143702221213010.1056/NEJ Mra 120870824869722 · doi ↗ · pubmed ↗
- 6Hajiaghamemar M Seidi M Oeur RA Margulies SS Toward development of clinically translatable diagnostic and prognostic metrics of traumatic brain injury using animal models: A review and a look forward Exp Neurol 2019318101233105500510.1016/j.expneurol.2019.04.019PMC 6612432 · doi ↗ · pubmed ↗
- 7Koura S Doppenberg E Marmarou A Choi S Young H Bullock R Relationship between excitatory amino acid release and outcome after severe human head injury Acta Neurochir Suppl 19982446977919610.1007/978-3-7091-6475-4_70 · doi ↗ · pubmed ↗
- 8Hajiaghamemar M Kilbaugh T Arbogast KB Master CL Margulies SS Using serum amino acids to predict traumatic brain injury: a systematic approach to utilize multiple biomarkers Int J Mol Sci 20202151786178610.3390/ijms 21051786 PMC 708469532150890 · doi ↗ · pubmed ↗