Housing Status and Healthcare Utilization in People Presenting With Seizure
Sandeepa S. Mullady, Andrew J. Wood, Elan L. Guterman, Nicole Rosendale

TL;DR
This study found that people experiencing homelessness who have seizures use healthcare services more frequently and differently than those with stable housing.
Contribution
The study provides new insights into how housing status affects healthcare utilization patterns in seizure patients.
Findings
People experiencing homelessness had higher odds of 30-day re-visit after seizure.
They had shorter hospital stays and were less likely to be discharged to a facility.
Housing status was linked to differences in healthcare use and outcomes.
Abstract
To examine the association between housing status and healthcare utilization in individuals presenting with seizure. We performed a retrospective cross-sectional analysis of all adults (age >18) presenting to a public hospital emergency department with seizures, defined by ICD-9/10 codes, between 1/1/2016 and 8/03/2019. They were categorized by housing status (people experiencing homelessness [PEH], people with housing). Healthcare utilization outcomes were 30-day re-visit to acute care, discharge disposition, and hospital length of stay for those admitted. We used multivariable linear and logistic regression models adjusting for age, comorbidities, and insurance status. There were 6483 individuals (2092 [32.3%] PEH). Compared to people with housing, PEH were younger (48.2 vs 50.9, P < .0001), more likely to be a person of color (80.9 vs 75.1%, P < .0001), and have Medicaid (51.4% vs…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
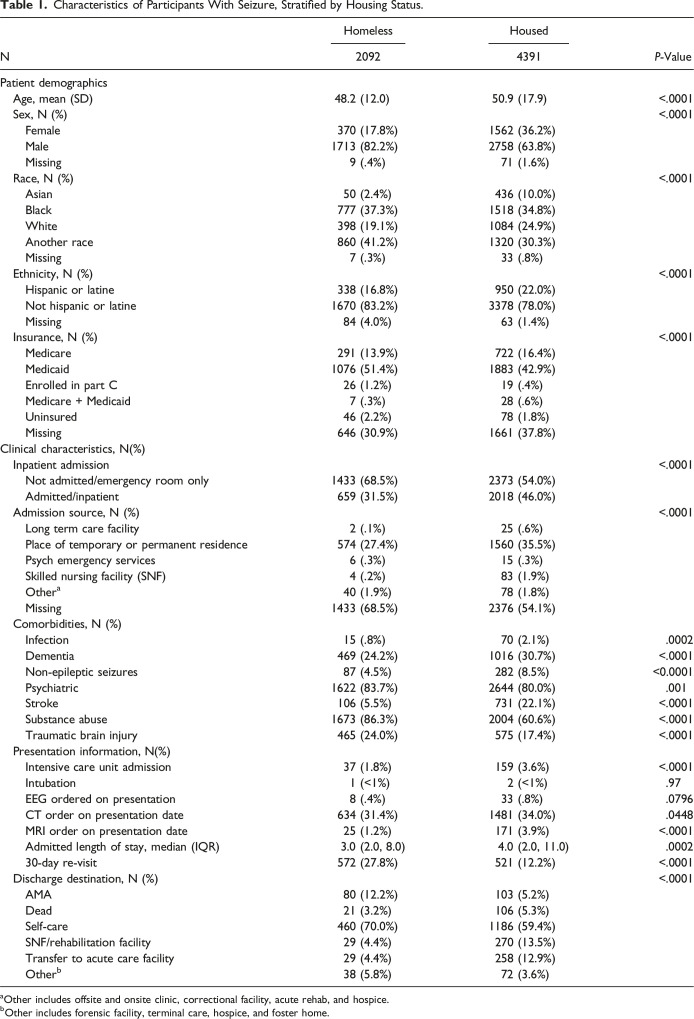 Figure 1
Figure 1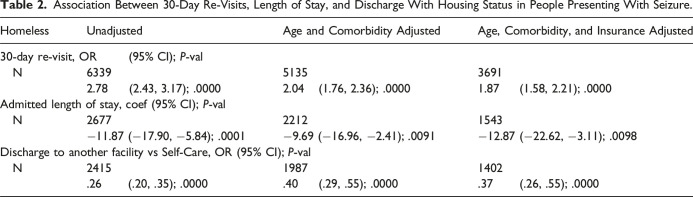 Figure 2
Figure 2- —National Institute of Neurological Disorders and Strokehttps://doi.org/10.13039/100000065
- —National Institute on Aginghttps://doi.org/10.13039/100000049
- —American Academy of Neurologyhttps://doi.org/10.13039/100005339
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHomelessness and Social Issues · Emergency and Acute Care Studies · Healthcare Decision-Making and Restraints
Introduction
Homelessness is an epidemic, with an estimated 582,462 people experiencing homelessness on a single night in the US.^ 1 ^ More than half of people experiencing homelessness (PEH) in the U.S. reside in California.^ 2 ^ PEH have high rates of healthcare utilization in acute care settings.^ 3 ^ Prior research suggests that seizure is a common indication for admission in PEH,^ 4 ^ however, little is known about healthcare utilization in this population.
The objective of this study was to assess the association between housing status and healthcare utilization in a sample of people presenting to the emergency department after seizure.
Methods
We performed a retrospective cross-sectional analysis of all adult patients (aged 18 years or older) who presented to the emergency department (ED), regardless of subsequent admission, at Zuckerberg San Francisco General Hospital (ZSFG) with a primary presentation diagnosis of seizure, defined by ICD-9 (345.x, 780.3, 333) and ICD-10 codes (G40, G41, R56), between January 1, 2016 and August 3, 2019. Due to conversion to another electronic health record (EHR) system, more recent data were not available.
Participant sociodemographic characteristics, including housing status, were obtained as they were coded in the EHR. Race was categorized as Asian, Black, White, or another race. Comorbidities (substance use, traumatic brain injury, stroke, infection, psychiatric conditions, non-epileptic seizures, dementia) were obtained using ICD9/10 codes. Specifically, for non-epileptic seizures, we used ICD-9 codes 300.1 and 300.11 (Dissociative, conversion, factitious; conversion) and ICD-10 code F44.5 (Dissociative convulsions) to avoid incorrectly identifying epileptic seizures as non-epileptic.^ 5 ^ Healthcare resource use (CT imaging, MR imaging, and EEG ordered on presentation date), and markers of illness severity (intensive care unit [ICU] admission, intubation) were obtained using billing codes. Primary outcomes were 30-day re-visit, length of stay, and discharge disposition in all those presenting to the ED. The 30-day re-visit variable was categorized as a binary (yes/no) variable based on the date between the first presentation and subsequent presentation, either to the ED or as a hospital readmission. Discharge disposition was dichotomized to self-care vs facility due to small sample sizes within individual categories. All patients at ZSGF receive social work and case management services, and the vast majority (regardless of immigration status) are insured under a Medicare or Medicaid insurance plan; thus, these variables were not included in the analysis.
We included those with complete housing information in the final analysis (n = 928 [12.5%] missing). We divided the population based on housing status and performed univariate analyses using 2 sample t-tests for continuous variables and Pearson’s chi-squared test for categorical variables. We assessed the association between homelessness and 30-day re-visits, length of stay, and discharge disposition using multivariable linear and logistic regressions, adjusting for age, comorbidities including psychiatric condition, dementia, stroke, infection, substance use, and traumatic brain injury, and insurance status. To investigate the role of race in the association between housing status and healthcare utilization, we performed regression models adjusting for the same independent variables adding an interaction term for race and housing status.
Statistical significance was set at α < .05 for both the univariate and multivariate analyses. Statistical analyses were performed with Stata (version 17, StataCorp, College Station, TX).
This study was approved by the institutional review board of University of California, San Francisco (certificate 16-19911) and was exempt from the need for informed consent as no direct participant contact was made. It was reported in alignment with The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplement 1).
Results
There were 6483 individuals who presented to the ED with seizure with complete housing status (2092, 32.3% PEH). PEH were younger (48.2 vs 50.9, P < .0001), more likely to be people of color (80.9 vs 75.1%, P < .0001), and more likely to be insured by Medicaid (51.4% vs 42.9%, P < .0001) (Table 1). PEH were less likely to be admitted (54% vs 68.5%, P < .0001; Table 1). Comorbidities differed between the groups: PEH had higher likelihood of substance use (86.3% vs 60.6%, P < .0001), higher likelihood of traumatic brain injury (24.0% vs 17.4%, P < .001), lower likelihood of stroke (5.5% vs 22.1%, P < .0001), and lower likelihood of non-epileptic seizures (4.5% vs 8.5%, P < .0001; Table 1).Table 1.Characteristics of Participants With Seizure, Stratified by Housing Status.NHomelessHousedP-Value20924391Patient demographics Age, mean (SD)48.2 (12.0)50.9 (17.9)<.0001 Sex, N (%)<.0001 Female370 (17.8%)1562 (36.2%) Male1713 (82.2%)2758 (63.8%) Missing9 (.4%)71 (1.6%) Race, N (%)<.0001 Asian50 (2.4%)436 (10.0%) Black777 (37.3%)1518 (34.8%) White398 (19.1%)1084 (24.9%) Another race860 (41.2%)1320 (30.3%) Missing7 (.3%)33 (.8%) Ethnicity, N (%)<.0001 Hispanic or latine338 (16.8%)950 (22.0%) Not hispanic or latine1670 (83.2%)3378 (78.0%) Missing84 (4.0%)63 (1.4%) Insurance, N (%)<.0001 Medicare291 (13.9%)722 (16.4%) Medicaid1076 (51.4%)1883 (42.9%) Enrolled in part C26 (1.2%)19 (.4%) Medicare + Medicaid7 (.3%)28 (.6%) Uninsured46 (2.2%)78 (1.8%) Missing646 (30.9%)1661 (37.8%)Clinical characteristics, N(%) Inpatient admission<.0001 Not admitted/emergency room only1433 (68.5%)2373 (54.0%) Admitted/inpatient659 (31.5%)2018 (46.0%) Admission source, N (%)<.0001 Long term care facility2 (.1%)25 (.6%) Place of temporary or permanent residence574 (27.4%)1560 (35.5%) Psych emergency services6 (.3%)15 (.3%) Skilled nursing facility (SNF)4 (.2%)83 (1.9%) Other^ a ^40 (1.9%)78 (1.8%) Missing1433 (68.5%)2376 (54.1%) Comorbidities, N (%) Infection15 (.8%)70 (2.1%).0002 Dementia469 (24.2%)1016 (30.7%)<.0001 Non-epileptic seizures87 (4.5%)282 (8.5%)<0.0001 Psychiatric1622 (83.7%)2644 (80.0%).001 Stroke106 (5.5%)731 (22.1%)<.0001 Substance abuse1673 (86.3%)2004 (60.6%)<.0001 Traumatic brain injury465 (24.0%)575 (17.4%)<.0001 Presentation information, N(%) Intensive care unit admission37 (1.8%)159 (3.6%)<.0001 Intubation1 (<1%)2 (<1%).97 EEG ordered on presentation8 (.4%)33 (.8%).0796 CT order on presentation date634 (31.4%)1481 (34.0%).0448 MRI order on presentation date25 (1.2%)171 (3.9%)<.0001 Admitted length of stay, median (IQR)3.0 (2.0, 8.0)4.0 (2.0, 11.0).0002 30-day re-visit572 (27.8%)521 (12.2%)<.0001 Discharge destination, N (%)<.0001 AMA80 (12.2%)103 (5.2%) Dead21 (3.2%)106 (5.3%) Self-care460 (70.0%)1186 (59.4%) SNF/rehabilitation facility29 (4.4%)270 (13.5%) Transfer to acute care facility29 (4.4%)258 (12.9%) Other^ b ^38 (5.8%)72 (3.6%)^a^Other includes offsite and onsite clinic, correctional facility, acute rehab, and hospice.^b^Other includes forensic facility, terminal care, hospice, and foster home.
PEH also had lower likelihood of ICU admission (3.6% vs 1.8% P < .0001) and undergoing MRI on presentation to the acute care setting (3.9% vs 1.2%, P < .0001).
Compared to those with housing, PEH had higher odds of a 30-day re-visit (adjusted odds ratio [aOR] 1.87, 95% CI: 1.58, 2.21), shorter length of stay (coef −12.87, 95% CI: −22.62, −3.11) and lower odds of being discharged to a facility (aOR 0.37, 95% CI: .26, .55) after adjustment (Table 2). There was no significant interaction of race with housing status on these associations.Table 2.Association Between 30-Day Re-Visits, Length of Stay, and Discharge With Housing Status in People Presenting With Seizure.HomelessUnadjustedAge and Comorbidity AdjustedAge, Comorbidity, and Insurance Adjusted30-day re-visit, OR (95% CI); P-val N6339513536912.78 (2.43, 3.17); .00002.04 (1.76, 2.36); .00001.87 (1.58, 2.21); .0000Admitted length of stay, coef (95% CI); P-val N267722121543−11.87 (−17.90, −5.84); .0001−9.69 (−16.96, −2.41); .0091−12.87 (−22.62, −3.11); .0098Discharge to another facility vs Self-Care, OR (95% CI); P-val N241519871402.26 (.20, .35); .0000.40 (.29, .55); .0000.37 (.26, .55); .0000
Discussion
In this cross-sectional analysis of people presenting with seizure to an urban public hospital, PEH had higher odds of 30-day re-visits, shorter lengths of stay, and lower odds of discharge to a facility. In this hospital system, all PEH are evaluated by social work and case management services and there are robust resources available for patient assistance. Despite these resources, disparities remain.
The increased odds of 30-day re-visits amongst PEH in our study may be related to a lack of medication access or limited seizure health literacy amongst PEH. In a national study examining epilepsy readmissions, repeat convulsion was the most cited reason for return to hospital suggesting the importance of medication titration or adherence.^6,7^ Alcohol use and psychosis were found to increase risk of readmission.^6,7^ There was a higher prevalence of psychiatric conditions and substance use in PEH in our study, which may have contributed to increased re-visit rate.
Our finding that PEH had shorter lengths of stay is different than other studies that show increased hospital lengths of stay among PEH.^ 8 ^ The prevalence of patient-directed discharge was higher in PEH in our sample and may partially explain these findings. Limitations in city-wide shelter resources may encourage individuals to join shelter waitlists that are filled on a first-come-first basis rather than await further work-up in the hospital setting. The 2023 California Statewide Study of People Experiencing Homelessness found that 41% of individuals who desired shelter were unable to do so.^ 9 ^
The prevalence of dementia itself was found to be lower in our study population; in general, cognitive impairment is higher amongst PEH.^ 10 ^ Seizures itself can contribute to cognitive decline in PEH, and this may impact a person’s understanding of the goals of the hospitalization or willingness to remain admitted.^ 11 ^ Shorter lengths of stay in PEH may contribute to incomplete titration of anti-seizure medication that result in increased re-visits. Patient acuity, measured through intubation and ICU rates, were lower amongst PEH and may be driving lengths of stay as well.
Prior interventions have focused on access to primary care. Our study makes a case for the development of pathways to improve access to neurologic care. One such previously established pathway involved automatic consultation of epilepsy services for all PEH presenting with seizure etiology and led to improved dissemination of information and integration of care to the outpatient setting.^ 12 ^ Integration of primary care services into homeless shelters has been shown to reduce barriers to access and increase preventative care.^ 13 ^ Integrating neurology into underserved settings such as street medicine clinics and federally qualified healthcare centers may similarly improve access. Transforming neurology from a subspeciality care service to a primary care model would allow for preventative neurologic care and potential unburdening of acute care systems.
Limitations include our mechanism of coding homelessness, which is based on demographic data in the EHR. Our designation of PEH was not sensitive enough to capture all those that may be unhoused, which biased the result towards null. Identifying other sociodemographics, such as primary language or immigration status, may elucidate other barriers to access, however, individuals in California have access to healthcare insurance regardless of immigration status. Despite the high rates of coverage in PEH in our study, disparities in healthcare utilization remain. We were not able to extract imaging results, medications, and presumed etiology of seizures, which may ascertain predictors in healthcare utilization, including differences in seizure severity and access to appropriately dosed medications. Additionally, this analysis is from a single center and, therefore, may not be generalizable to the larger population.
Conclusions
PEH with seizures have high healthcare utilization despite potentially lower clinical acuity. Our study suggests that these disparities exist even within a healthcare system with robust social work support. Further research better characterizing the reasons for re-visits in PEH will be helpful in devising systemic solutions.
Supplemental Material
Supplemental Material - Housing Status and Healthcare Utilization in People Presenting With Seizure Supplemental Material for Housing Status and Healthcare Utilization in People Presenting With Seizure by Sandeepa S. Mullady, Andrew J. Wood, Elan L. Guterman, and Nicole Rosendale in Journal of the Neurohospitalist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1de Sousa T Andrichik A Cuellar M Marson J Prestera E Rush K . The 2022 Annual Homelessness Assessment Report (AHAR). Washington, DC: The U.S. Department of Public Health; 2022.
- 2Committee CSH . Fact Sheet: Homelessness in California. Sacramento, CA: Committee CSH; 2021.
- 3Kushel MB Vittinghoff E Haas JS . Factors associated with the health care utilization of homeless persons. JAMA. 2001;285(2):200-206. doi:10.1001/jama.285.2.20011176814 · doi ↗ · pubmed ↗
- 4Rosendale N Guterman EL Betjemann JP Josephson SA Douglas VC . Hospital admission and readmission among homeless patients with neurologic disease: retraction and replacement. Neurology. 2019;92:e 2822-e 2831.31127074 10.1212/WNL.0000000000007645 PMC 7987868 · doi ↗ · pubmed ↗
- 5Altalib HH Galluzzo D Argraves S , et al. Managing functional neurological disorders: protocol of a cohort study on psychogenic non-epileptic seizures study. Neuropsychiatric Dis Treat. 2019;15:3557-3568. doi:10.2147/NDT.S 234852 PMC 693917631920316 · doi ↗ · pubmed ↗
- 6Blank LJ Crispo JAG Thibault DP Davis KA Litt B Willis AW . Readmission after seizure discharge in a nationally representative sample. Neurology. 2018;92(5):e 429-e 442. doi:10.1212/WNL.0000000000006746 PMC 636990630578373 · doi ↗ · pubmed ↗
- 7Terman SW Guterman EL Hill CE Betjemann JP Burke JF . Factors associated with 30-day readmission for patients hospitalized for seizures. Neurol Clin Pract. 2020;10(2):122-130. doi:10.1212/CPJ.000000000000068832309030 PMC 7156187 · doi ↗ · pubmed ↗
- 8Hwang SW Weaver J Aubry T Hoch JS . Hospital costs and length of stay among homeless patients admitted to medical, surgical, and psychiatric services. Med Care. 2011;49(4):350-354. doi:10.1097/MLR.0b 013e 318206 c 50d 21368678 · doi ↗ · pubmed ↗