A Case of Nocardia kroppenstedtii Infection Successfully Treated With a Multidisciplinary Approach
Francesco Foglia, Annalisa Ambrosino, Giuseppe Greco, Annalisa Chianese, Carla Zannella, Francesca Cinone, Alfonso Reginelli, Diego Sandro Giordano, Giovanni Tortorella, Maria Teresa Laieta, Anna De Filippis, Massimiliano Galdiero, Rita Greco, Emiliana Finamore

TL;DR
A rare Nocardia infection in an older patient was successfully treated using a multidisciplinary medical approach.
Contribution
This paper reports a rare clinical case of Nocardia kroppenstedtii infection in an immunocompetent individual.
Findings
Nocardia kroppenstedtii was isolated from a 69-year-old patient's subxiphoid and leg formations.
The infection was successfully managed through antimicrobial stewardship and multidisciplinary care.
Only five clinically relevant cases of this rare species have been documented in literature.
Abstract
Nocardia species constitute a diverse group of microorganisms classified as aerobic actinomyces. Among these species, many have been implicated as causative agents of severe human infections, particularly in immunocompromised patients, affecting lungs, skin, and nervous system. Here, we described a rare species, identified as Nocardia kroppenstedtii, isolated at the Complex Operative Unit of Virology and Microbiology from the subxiphoid formation and pseudonodular formation in the left leg of a 69-year-old immunocompetent patient, who was hospitalized and treated at the Complex Operative Unit of Internal Medicine and Geriatrics of the University Hospital of Campania “Luigi Vanvitelli” in an antimicrobial diagnostic stewardship context. This rare pathogen was first isolated in 2014 from a bronchoalveolar lavage sample obtained from a lung transplant recipient. Since then, only five cases…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
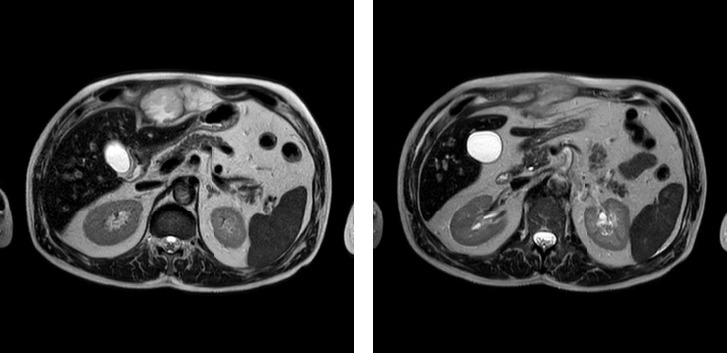 Figure 1
Figure 1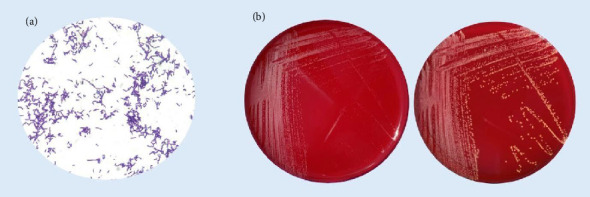 Figure 2
Figure 2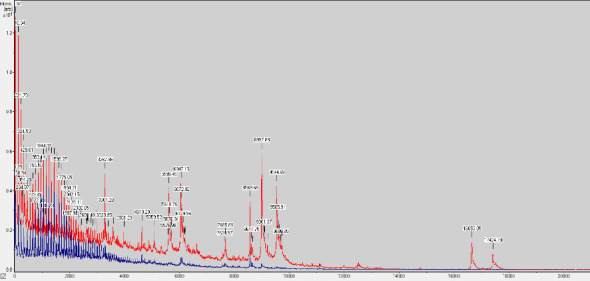 Figure 3
Figure 3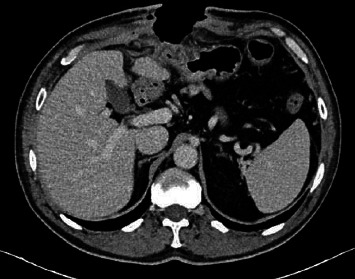 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsActinomycetales infections and treatment · Infectious Diseases and Mycology · Fungal Infections and Studies
1. Introduction
Nocardia spp. is a group of Gram-positive bacteria commonly found in soil, water, and organic matter [1]. These bacteria thrive in aerobic conditions and exhibit variable acid-fast staining. The genus was first isolated and described by Edmond Nocard in 1888 [2]. Since then, many species have been identified, thanks to the advent of molecular methods and the increasing availability of whole-genome sequencing [3]. According to the List of Prokaryotic Names with Standing in Nomenclature (LPSN), the Nocardia genus currently counts 251 species (https://www.bacterio.net); Among the 251 identified species, only a small subset is pathogenic to humans causing opportunistic and potentially fatal infections, especially in immunocompromised patients like organ transplant recipients, individuals with malignancy and suffering from acquired immunodeficiency syndrome (AIDS) [4].
The clinical picture of nocardiosis depends on the body systems affected by the infection, specifically lungs, skin, and central nervous system (CNS). In 80% of cases, lung involvement occurs due to inhalation, causing severe pneumonia (acute/subacute/chronic infection), which could disseminate to the CNS, evolving in abscesses into the brain and other organs: the onset of skin infections occurs in 20% of cases after a traumatic event through direct skin contact, which could result in lymphocutaneous infection with ulceration of lymph nodes while disseminated infections involving multiple organs are less frequent, and they can be life-threatening [5]. Identifying Nocardia species is crucial in clinical practice because their susceptibility to antibiotics is varied [6]. Recently, a fair number of infections occurred in patients with none of the conditions mentioned above, suggesting that a weakened immune system is not the only predisposing factor to infection.
The mechanisms of pathogenesis are not entirely clear and include the ability to evade the host's microbicidal activities. Actually, immunocompetent patients with nocardiosis represent one-third of all cases [7–11].
In the last decade, a new species was isolated from a bronchoalveolar lavage sample obtained from a lung transplant recipient and recognized as Nocardia kroppenstedtii in the United Kingdom [12].
Although Nocardia species are generally found worldwide, with cases frequently reported in Europe, Asia, North America, and other regions, specific global distribution data for Nocardia kroppenstedtii is peculiarly limited, with only few human isolations reported globally. Nocardia species, including Nocardia kroppenstedtii, are typically associated with soil and water environments, from which they can be transmitted to humans [3].
Here, we present a rare case study involving the isolation of N. kroppenstedtii in a patient with a competent immune system treated at the University Hospital of Campania “Luigi Vanvitelli” in Naples, Italy, which highlights the crucial role of the antimicrobial diagnostic stewardship program implemented in our hospital [13–15] in formulating accurate treatment plans.
To the best of our knowledge, this is the sixth reported clinical case in the world.
2. Clinical Case Overview
A 69-years-old patient with a mute medical history presented at our hospital with fever, a large subxiphoid-evolving swelling, which developed two weeks after exerting intense effort from a physical activity outdoor, and another lump on the inside of the upper third of the right inner thigh. A thoracic computed tomography (CT) scan performed two weeks before admission, showed inhomogeneous subxiphoid hypodensity and pseudonodular formation in the left leg lobe, with speculated contours and a ground-glass thickening halo; therefore, a therapy consisting of 200 mg cefditoren pivoxil for 10 days and 25 mg deltacortene for a week plus 12,5 mg deltacortene for another week was administered. One week before admission, the patient started to experience fever responsive to paracetamol. Magnetic resonance imaging (MRI) contrast examination showed an increased swelling with irregular and intense thickening and progressive enhancement of the walls with uneven content (Figure 1). The patient was then hospitalized with a blood pressure of 130/60 mmHg, SpO2 of 97%, 38.7°C fever, and a heart rate of 110 BPM. The blood samples showed high neutrophil counts and a CRP 23 times the normal value (10.5 mg/dL). The elevated levels of transaminases, gamma-glutamyl transferase, and alkaline phosphatase indicated a possible compression of the mass on the bile ducts and the liver. The patient was in severe pain, to the extent that he was using opioid patches. A nasopharyngeal swab for SARS-Cov2 detection was done, and the result was negative. Chemiluminescence immunoassay results for Hepatitis B Virus (HBV), Hepatitis C Virus (HCV), and Human Immunodeficiency Virus (HIV) were negative.
The patient underwent a drainage surgical procedure to remove the subxiphoid abscess collection and the pseudonodular formation identified on CT and MRI, with the aim of analyzing and identifying any potential isolates and remained hospitalized in the UOC of Internal Medicine and Geriatrics while the antibiotic treatment was upscaled according to European Society of Clinical Microbiology and Infection Diseases (ESCMID) guidelines to meropenem (3 g/d) and vancomycin (30 mg/kg/d) on the first day.
The drainage fluids collected during the surgical intervention from the subxiphoid formation and pseudonodular formation were sent at the UOC of Microbiology and Virology, cultured in brain heart infusion (BHI) broth and incubated at 37°C. Meanwhile, the staining of the two samples resulted in Gram-positive bacilli with a branching filamentous morphology that resembled actinomycetes (Figure 2(a)). The next day, the turbidity of the two broths indicated microbial growth. To isolate the eventual infectious agent and both were plated on culture media, including MacConkey agar, Columbia CNA agar with 5% Sheep Blood, Chocolate agar, Sabouraud Dextrose agar (Liofilchem, Italy), and incubated at 37°C for 24 h. After the incubation period, we observed the growth of greyish colonies only on Columbia CNA agar which became yellowish after 4–5 days (Figure 2(b)), for both the fluids. We confirm that the two samples were colonised by the same agent performing matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS, Bruker Daltonics, USA) identification. The identification of the microorganism in both isolates was repeated two times for sample and resulted in Nocardia kroppenstedtii with a high confidence score.
The data generated by MALDI-TOF MS (Software version 4.1 (100), specific to the species, were analyzed according to the manufacturer's instructions. Additionally, the spectra underwent baseline correction and were adjusted to the total positive ion current [16] (Figure 3).
The antibiotic susceptibility testing revealed that the strain was resistant to meropenem, and high-susceptible to trimethoprim/sulfamethoxazole (TMP-SMX) (Table 1).
The identification of N. kroppenstedtii with its susceptibility pattern led to an updating of the empirical therapy into a targeted one and IV TMP-SMX (400/80/5 mg) was started at a dosage of three infusions a day. After 2 days, the neutrophil counts and CRP levels started to decrease drastically, reaching basal values, and the two blood culture sets performed resulted negative. The patient no longer had fever, and the opioid patch was removed as he no longer felt any pain. A total body CT scan was performed before dismission, showing successful surgical site debridement with no residual collections (Figure 4).
3. Discussion
Since its pathogenic emergence nocardiosis has been characterized as a disease primarily affecting patients with weakened immune systems. This is due to the multitude of cases linked to comorbidities such as Hodgkin's lymphoma, AIDS, Cushing's syndrome, various forms of cancer, the use of drugs that suppress the immune system, lung diseases, chronic kidney diseases, and more. However, recent epidemiological research indicates that not all individuals diagnosed with nocardiosis have concurrent diseases or identifiable risk factors [4–11]. This case report emphasizes an exceptionally rare instance of N. kroppenstedtii infection, which also exhibits unusual localizations. It also provides the first account of N. kroppenstedtii being identified in drainage fluid and the first recorded infection of this pathogen of extreme rarity in a patient with a healthy immune system. Nocardia kroppenstedtii is known for causing severe invasive infections that can be life-threatening. Since its initial identification in 2014, only six cases have been reported in medical literature including this paper, with the majority resulting in fatal outcomes [12, 17–20] (Table 2). This case also marks the first time that MALDI-TOF has been successfully used in diagnosing Nocardia kroppenstedtii.
Current guidelines for treating nocardiosis suggest starting empirical therapy with TMP-SMX or alternative medications such as linezolid and amikacin. For more severe infections, a combination therapy of TMP-SMX and third-generation cephalosporins or carbapenems is recommended.
Antibiotic susceptibility testing confirmed that TMP-SMX and tigecycline were the most effective treatments, aligning with existing guidelines while both cephalosporins and carbapenems showed resistance. Interestingly, this particular strain presented a decreased susceptibility to meropenem.
4. Conclusion
The positive outcome of the patient's surgical and clinical treatment, facilitated by interdepartmental collaboration, underscores the significance of a multidisciplinary strategy. This strategy is crucial within the framework of antimicrobial diagnostic stewardship across laboratories and hospital units. It enhances both the treatment process and patient results in infection cases. This is particularly true when the infections are caused by exceptionally uncommon pathogens, as demonstrated in this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wilson J. W. Nocardiosis: Updates and Clinical Overview Mayo Clinic Proceedings 20128740340710.1016/j.mayocp.2011.11.0162-s 2.0-8485983551522469352 PMC 3498414 · doi ↗ · pubmed ↗
- 2Fatahi-Bafghi M. Nocardiosis From 1888 to 2017 Microbial Pathogenesis 201811436938410.1016/j.micpath.2017.11.0122-s 2.0-8503781772029146497 · doi ↗ · pubmed ↗
- 3Traxler R. M. Bell M. E. Lasker B. Headd B. Shieh W.-J. Mc Quiston J. R. Updated Review on Nocardia Species: 2006–2021 Clinical Microbiology Reviews 202235000277 e 12110.1128/cmr.00027-21PMC 976961236314911 · doi ↗ · pubmed ↗
- 4Filice G. A. Nocardiosis in Persons With Human Immunodeficiency Virus Infection, Transplant Recipients, and Large, Geographically Defined Populations Journal of Laboratory and Clinical Medicine 200514515616210.1016/j.lab.2005.01.0022-s 2.0-1594440578015871308 · doi ↗ · pubmed ↗
- 5Malaguez Webber F. Nachiappan A. Lau F. D. Costello C. Zane S. Nocardia Caishijiensis Infection: A Case Report and Review of the Literature BMC Infectious Diseases 202323 p. 21810.1186/s 12879-023-08186-z PMC 1008082537024793 · doi ↗ · pubmed ↗
- 6Takiguchi Y. Ishizaki S. Kobayashi T. Pulmonary Nocardiosis: A Clinical Analysis of 30 Cases Internal Medicine 2017561485149010.2169/internalmedicine.56.81632-s 2.0-8502054420028626172 PMC 5505902 · doi ↗ · pubmed ↗
- 7Roy M. Martial A. Ahmad S. Disseminated Nocardia Beijingensis Infection in an Immunocompetent Patient European Journal of Case Reports in Internal Medicine 20207 p. 00190410.12890/2020_001904 PMC 765499433194869 · doi ↗ · pubmed ↗
- 8Wintheiser G. A. Venable E. R. Temesgen Z. Disseminated Nocardia in an Immunocompetent Host Mayo Clinic Proceedings 20219684784810.1016/j.mayocp.2020.11.01933814090 · doi ↗ · pubmed ↗