A comprehensive multidisciplinary approach for identifying asbestos exposure among underground workers
Alejandro Salvado, Lilian Capone, Paula Zamorano, Mayra Samudio, María Teresa Garcia-de-Dávila, Glenda Ernst

TL;DR
This study identifies asbestos-related diseases in underground workers, showing that long-term exposure increases risk.
Contribution
The study provides new insights into the prevalence and risk factors of asbestos-related diseases in a specific occupational group.
Findings
2.8% of participants had asbestos-related diseases, with 0.22% diagnosed with lung cancer.
Occupational exposure exceeding 20 years significantly increased the risk of asbestos-related diseases.
Findings align with other surveillance programs on asbestos-exposed workers.
Abstract
Inhalation of asbestos fibers can lead to a range of diseases, including asbestosis, pleural plaques, lung cancer, and malignant mesothelioma. Despite regulatory efforts, asbestos-related diseases remain a significant public health issue. This study aimed to assess the characteristics and prevalence of asbestos-related diseases among exposed workers. We conducted a descriptive cohort study with underground workers in Buenos Aires, Argentina, from March 2018 to March 2023. A comprehensive screening and surveillance program, including medical examinations, was implemented to identify exposure-related signs and symptoms. Histological sections from paraffin-embedded tissue blocks were analyzed using light and polarization microscopy for lung cancer cases. A total of 2,690 participants were included, of whom 2.8% (n = 77) had asbestos-related diseases and 0.22% (n = 6) had lung cancer.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
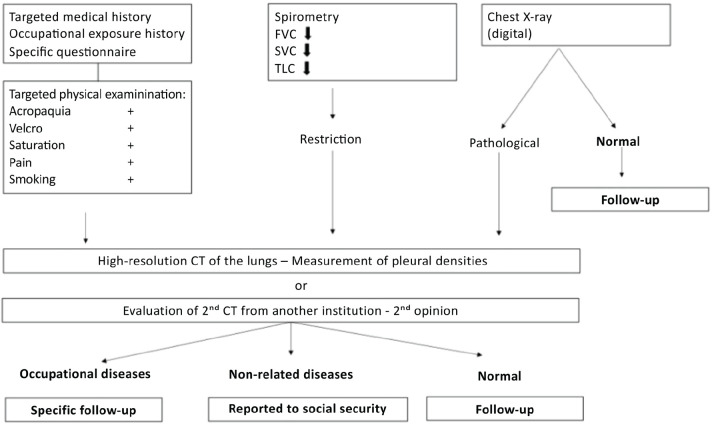 Figure 1
Figure 1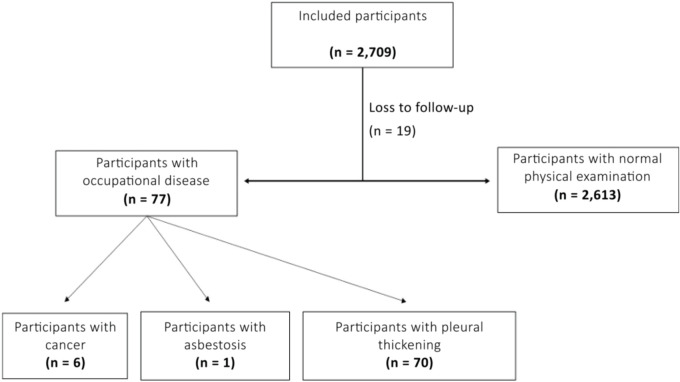 Figure 2
Figure 2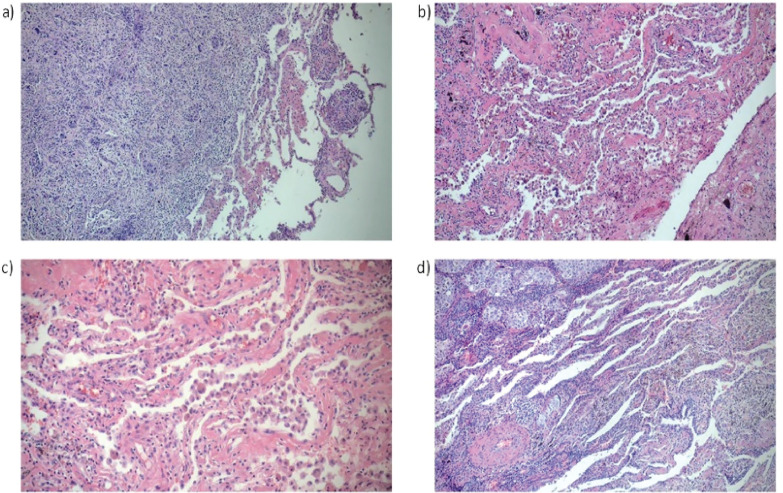 Figure 3
Figure 3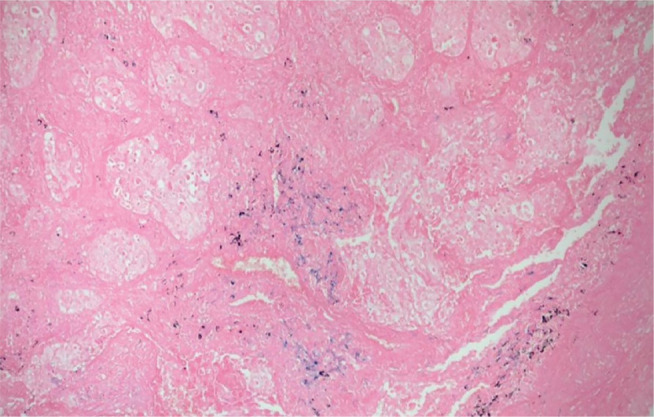 Figure 4
Figure 4| Occupational disease | Normal | p-value | |
|---|---|---|---|
| n | 77 | 2,613 | |
| IMC (kg/m2) | 29.1 ± 7.8 | 29.4 ± 5.7 | 0.9 |
| Age | 58.1 ± 8.6 | 24.9 ± 10.9 | 0.001 |
| Working under 10 years, % (n) | 12.9 (10) | 28.7 (750) | 0.9 |
| Working between 10 to 20 years, % (n) | 23.4 (18) | 35.3 (923) | 0.006 |
| Working over 20 years, % (n) | 63.6 (49) | 35.9 (940) | 0.001 |
| Smoker, % (n) | 35.0 (27) | 23.5 (614) | 0.4 |
| Ex-smoker, % (n) | 29.8 (23) | 22.4 (585) | 0.1 |
| Restrictive spirometry, % (n) | 29.8 (23) | 7.6 (200) | 0.0001 |
| Symptoms, % (n) | 74.0 (57) | 13.7 (360) | 0.001 |
| Pathological CT findings, % (n) | 29.8 (23) | 6.2 (157) | 0.0001 |
| Pathological CX-ray findings, % (n) | 29.8 (23) | 0.1 (3) | 0.0001 |
| Digital clubbing, % (n) | 24.7 (19) | 1.2 (32) | 0.0001 |
| Velcro crackles, % (n) | 4.0 (3) | 1.2 (32) | 0.07 |
| Pain, % (n) | 2.5 (2) | 0.6 (17) | 0.1 |
| Age | Smoking (pack/year) | Exposure time (years) | Workplace exposure | Symptoms | Diagnosis |
|---|---|---|---|---|---|
| 58 | 40 | 15 | Technical Support Center | Digital clubbing. Chest X-ray: pathological findings. | Adenocarcinoma |
| 55 | Never smoked | 7 | Technical Support Center | Chest pain | Malignant epithelioid mesothelioma |
| 50 | 25 | 28 | Technical Support Center | No symptoms. Pathological chest X-ray findings. | Adenocarcinoma |
| 51 | 20 | 26 | Driver | Digital clubbing. Normal spirometry, history of HIV and anal cancer. | Primary lung adenocarcinoma |
| 59 | 14 | 25 | Technical Support | Pathological findings on chest CT | Acinar adenocarcinoma |
| 50 | 36 | 25 | Technical Support Center | Digital clubbing and pathological chest X-rays findings | Squamous cell carcinoma |
| Variable | Odds ratio | 95%CI |
|---|---|---|
| Working > 20 years | 3.02 | 1.72-5.31 |
| Working > 10 years | 1.28 | 0.58-2.83 |
| Age | 1.04 | 1.02-1.05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases
INTRODUCTION
Asbestos refers to a group of mineral silicates, frequently used in construction due to their structural strength and heat-resistant properties. There are two types of asbestos fibers, namely serpentine and amphibole, each with distinct physical and chemical characteristics.^1,2^ Repeated inhalation of these fibers increases the risk of pleuropulmonary diseases, asbestosis, and lung cancer. Most of these conditions have a prolonged latency period.^3,4^
Pleuropulmonary diseases can manifest as either malignant or non-malignant. Malignant mesothelioma, a rare tumor in the general population, is associated with long-term exposure to asbestos, especially amphibole fibers.^5^ More than 85% of cases of mesothelioma are associated with occupational exposure.^3^ The non-malignant forms of asbestos may present as pleural plaques, diffuse pleural thickening, benign pleural effusion, and rounded atelectasis. Benign pleural disease typically has a long latency period, usually more than 20 years.^6^ In populations environmentally exposed to asbestos, the prevalence of benign pleural disease ranges from 0.53% to 8%, increasing proportionally with the years of exposure.^7^
Asbestosis is characterized by diffuse interstitial fibrosis secondary to inhalation of asbestos fibers. Symptoms generally appear after a latency period of 20-30 years and include digital clubbing, Velcro crackles, and dry cough. The most common comorbidity in patients with asbestosis is pleural plaques (96%).^8^
Asbestos exposure has also been reported to increase the risk of lung cancer by 1.24 (95%CI 1.18-1.31) in men and 1.12 (95%CI 0.95-1.31) in women. This risk is further increased in smokers.^9^
In 1997, Argentina prioritized asbestos within its National Plan for the Rational Management of Chemical Substances, recognizing that exposure to asbestos poses risks to both workers and the general population. Argentina pledged to provide its citizens with the same level of protection as many developed countries.^10^ In 2000, Argentina became the first country in Latin America to ban the use of asbestos (Resolution 845), specifically amphiboles. In 2001, Resolution 823 banned the production, import, marketing, and use of chrysotile asbestos fibers and products containing them as of 1 January 2003.^11^
Despite these regulatory efforts, the risk of occupational exposure to asbestos persists, particularly for workers involved in demolition, maintenance, repair, and transportation of asbestos-containing structures.^12^ In March 2018, a surveillance program was initiated to monitor the presence of asbestos in the underground facilities of the city of Buenos Aires, Argentina.
The aim of this study was to describe epidemiological monitoring protocols for asbestos and assess the prevalence of occupational diseases related to asbestos exposure among underground workers in Buenos Aires, Argentina.
METHODS
DESIGN
We conducted a descriptive cohort study with all underground employees in the city of Buenos Aires. Participants were followed from March 2018 to March 2023.
The study was approved by the Ethics Committee of the British Hospital of Buenos Aires (CRIHB # 1237).
POPULATION
Underground workers were recruited and categorized as drivers, workshop workers, or other employees. Participants with a follow-up period of less than 36 months were excluded from the analysis.
PROCEDURE
A surveillance program was implemented to monitor the potential presence of asbestos in facilities, overseen by a multidisciplinary committee. Workers were registered in the Risk Agents Register (RAR), which included employees who had been exposed to asbestos in their workplace. This registration initiated lifelong epidemiological monitoring consisting of 3 specific tests: detection of asbestos detection, chest X-rays, and spirometry, with high-resolution computed tomography (CT) performed as needed. Additionally, clinical records were required to be maintained for 40 years.^13^
All participants in this study completed a patient information form and an occupational exposure questionnaire. A specialized team comprising pulmonologists, radiologists, and occupational medicine experts was assembled, and a working algorithm for diagnosis and surveillance was established, as illustrated in Figure 1.
Figure 1. Algorithm for the management, diagnosis, and epidemiological surveillance of workers exposed to asbestos. CT = computed tomography; FVC = forced vital capacity; SVC = slow vital capacity; TLC = total lung capacity, measured by plethysmography.
The most significant radiographic indicator considered for registration was the presence of small lung opacities classified as grade 1/1 or higher according to the International Labour Organization (ILO). Additionally, an occupational exposure questionnaire was incorporated into the screening process. A pneumonologist conducted physical examinations to identify signs such as acropachy, Velcro crackles, or other symptoms indicative of asbestos exposure. Spirometry was performed, and if results suggested restriction, this was further confirmed or ruled out through lung volume measurements using plethysmography.
For patients with ambiguous X-ray findings or with clinical and functional abnormalities, high-resolution CT scans with 1-mm thin sections for both inspiratory and expiratory sequences, coupled with the Modified Medical Research Council (mMRC) dyspnea questionnaire, was recommended.
Upon completion of these evaluations, a multidisciplinary team consisting of medical specialists from the union, the occupational risk insurance company, the employer, and the Pneumonology Service of the British Hospital reviewed the findings. Criteria for the indication of chest CT without contrast combining both expiratory and inspiratory sequences was based on the following criteria: a) pathological X-ray findings; b) spirometry suggesting restrictions, confirmed by lung volume measurements; c) presence of Velcro crackles or acropachy; d) unexplained dyspnea; and e) occupational history indicating significant asbestos exposure, as assessed by a specific questionnaire that also evaluated smoking habits.
For patients who completed the study, CT scans were reviewed by a specialized radiologist within the multidisciplinary team. In cases where pleural thickening was observed on the images, the densities were carefully examined to differentiate them from neighboring structures such as extrapleural fat or muscle.
HISTOPATHOLOGICAL ANALYSIS OF TISSUE BIOPSIES
For patients diagnosed with lung cancer, histopathological analysis was performed on new sections prepared from paraffin-embedded tissue blocks to investigate the presence of asbestos fibers. Hematoxylin and eosin, Giemsa, and Perls stains were used to detect iron deposits and identify asbestos fibers.
STATISTICAL ANALYSIS
Descriptive statistics were used, with continuous variables expressed as mean ± SD and categorical variables as percentages. Patients were grouped according to the presence or absence of occupational disease. The t-test and chi-square test were used to compare variables. Multivariate analysis was performed to determine the impact of exposure duration in years on the onset of asbestos-related disease, with smoking status included as a confounding adjustment variable. Analyses were performed using GraphPad Prism 8.0.2 and MedCalc 12.0.
RESULTS
A total of 2,709 underground workers in Buenos Aires were initially included in the study (Figure 2). Nineteen participants were excluded due to loss to follow-up. Of the remaining 2,690, 2.8% (n = 77) were diagnosed with an occupational disease, including six cases of cancer (0.22%). The study population was predominantly male (90.1%, n = 2,440), with women accounting for 9.9% (n = 250). Mean participant age was 48.1 ± 10.9 years.
Figure 2. Flow chart of study participants.
The characteristics of the patients, categorized by the presence or absence of occupational disease, are detailed in Table 1. A significantly higher proportion of occupational disease was observed among workers employed for over 20 years. However, smoking habits did not differ significantly between those with and without occupational disease. Additionally, most symptomatic workers had been diagnosed with an occupational disease, as well as those with restrictive spirometry, pathological X-ray findings, and abnormal CT scans compared to those without occupational disease. Of the 77 patients diagnosed with asbestos-related disease, 94.8% (n = 73) were men, with the remaining 4 being women.
Table 1: Characteristics of participants grouped by the presence or absence of occupational disease
Six male patients developed malignant neoplasms. Four of them had been exposed to asbestos for more than 20 years, and one for less than 10 years. Among these patients, five were either current or former smokers (Table 2).
Light microscopy revealed alveoli containing numerous foamy and multinucleated macrophages, with mesothelioma as the primary diagnosis (Figure 3a). Another patient exhibited areas with ciliated columnar epithelium, sparse macrophages, and malignant neoplasia, diagnosed as squamous cell carcinoma (Figure 3b). In a patient with lung adenocarcinoma, areas of malignant neoplasia coexisted with alveoli showing siderosis and anthracosis (Figure 3c). Lastly, histological sections from another patient with lung adenocarcinoma exhibited fibrohyaline tissue infiltrated with neoplastic cells (Figure 3d).
Figure 3. Pathology study. a) Intra-alveolar malignant neoplasm. H&E, original magnification: 10×. b) Alveolar spaces with pneumonocytes, intra-alveolar macrophages, and areas of interstitial hyalinization with anthracotic pigment. H&E: original magnification: 10×. c) Alveolar spaces with pneumonocytes, intra-alveolar macrophages, and areas of interstitial hyalinization with anthracotic pigment. H&E, original magnification: 20×. d) Malignant neoplasm with lymphomononuclear infiltrate and vascular structure thickening.
Perls’ technique for iron staining did not reveal iron bodies in the “drumstick” form described in the literature. However, iron deposits and anthracotic pigments were detected (Figure 4).
Figure 4. Presence of iron deposits (blue) and anthracotic pigment. Perls’ technique, original magnification: 20×.
Multivariate analysis determined that occupational exposure for more than 20 years significantly increased the risk ratio for asbestos-related disease (odds ratio [OR]: 3.02, 95%CI 1.72-5.31), while the risk for over 10 years of exposure was OR: 1.28, with 95%CI 0.5832-2.83 (Table 3).
DISCUSSION
According to the World Health Organization (WHO), approximately 125 million people worldwide are exposed to asbestos in the workplace.^2^ Asbestos consumption in Latin America accounts for 10% of the world’s annual production.^14^ Despite international bans, a global study in 59 countries showed that asbestos-associated mesothelioma causes 9.9 deaths per million annually.^15^
A surveillance program conducted in Germany from 2008 to 2018, involving 2,439 male workers exposed to asbestos, reported a 4.45% prevalence of recognized occupational diseases.^16^ In comparison, the prevalence in our patient cohort was 2.8%. However, the German authors identified a 2.7% prevalence of lung cancer, compared to only 0.22% in our study. Previous research has shown that in Argentina, the risk of mesothelioma due to asbestos exposure is 1.48.^17,18^
The risk of lung cancer increases with asbestos exposure, and the combined impact of asbestos and smoking is cumulative.^19,20^ In our cohort, five of the six patients with lung cancer were smokers. We observed a high percentage of active or former smokers among those with and without occupational disease in our patient series. However, due to the retrospective nature of our study, there may have been potential bias in documenting smoking history for all participants, which precluded its inclusion in the multivariate analysis.
In the multivariate analysis, increased age was also associated with a slight increase in the risk of having an occupational disease. We hypothesized that this trend may be influenced by the number of years of occupational exposure.
Our findings emphasize the need for regular, structured follow-up for all workers with direct or indirect exposure to asbestos. Furthermore, there is a clear need for smoking cessation counseling and a multidisciplinary approach to managing individuals exposed to asbestos in the workplace.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berry TA Belluso E Vigliaturo R GieréR Emmett EA Testa JR Asbestos and other hazardous fibrous minerals: potential exposure pathways and associated health risks Int J Environ Res Public Health 202219740313540971110.3390/ijerph 19074031 PMC 8998304 · doi ↗ · pubmed ↗
- 2World Health Organization Asbestos[Internet]Geneva WHO 2024 accessed 2024 Nov 13Available: http://www.who.int/mediacentre/factsheets/fs 343/en/
- 3Markowitz S. Asbestos-related lung cancer and malignant mesothelioma of the pleura: selected current issues Semin Respir Crit Care Med 20153633343462602434210.1055/s-0035-1549449 · doi ↗ · pubmed ↗
- 4Luberto F Ferrante D Silvestri S Angelini A Cuccaro F Nannavecchia AM Cumulative asbestos exposure and mortality from asbestos related diseases in a pooled analysis of 21 asbestos cement cohorts in Italy Environ Health 2019181713139107810.1186/s 12940-019-0510-6PMC 6686495 · doi ↗ · pubmed ↗
- 5Larson T Melnikova N Davis SI Jamison P. Incidence and descriptive epidemiology of mesothelioma in the United States, 1999-2002 Int J Occup Environ Health 20071343984031808505310.1179/oeh.2007.13.4.398 · doi ↗ · pubmed ↗
- 6Tsao AS Wistuba I Roth JA Kindler HL. Malignant pleural mesothelioma J Clin Oncol 20092712208120901925531610.1200/JCO.2008.19.8523 PMC 4881753 · doi ↗ · pubmed ↗
- 7Robinson BW Lake RA. Advances in malignant mesothelioma N Engl J Med 200535315159116031622178210.1056/NEJ Mra 050152 · doi ↗ · pubmed ↗
- 8Keskitalo E Salonen J Nurmi H VähänikkiläH Kaarteenaho R. Comorbidities and causes of death of patients with asbestosis J Occup Environ Med 20236543493533672894710.1097/JOM.0000000000002777 · doi ↗ · pubmed ↗