A single-centre, retrospective study on the impact of omitting preoperative antibiotic prophylaxis on wound infections in minor orthopedic implant removals
Cyrill Pfammatter, Jan Hambrecht, Yannik Kalbas, Valentin Neuhaus, Christian Hierholzer, Claudio Canal

TL;DR
This study found that skipping antibiotics before minor orthopedic implant removals doesn't increase infection risks.
Contribution
The study provides evidence that preoperative antibiotics may be unnecessary for minor implant removal surgeries.
Findings
No deep wound infections were observed in patients who skipped preoperative antibiotics.
Wound-healing disorders occurred at similar rates with or without preoperative antibiotics.
Abstract
The use of preoperative antibiotic prophylaxis (POAP) in elective implant removal (IR) is controversial due to a lack of evidence-based recommendations. First-generation cephalosporins, which are commonly used in orthopedic IR, are believed to reduce wound infection risks. However, the potential for serious side effects had raised concerns about their necessity. This study was intended to evaluate whether omitting POAP in small IR increases the risk of wound infections. This retrospective, single-centre cohort study was conducted at a level I trauma centre in Switzerland, including patients who underwent IR between January 1, 2016, and December 31, 2021. The IR procedures involved the upper extremities (UEs), such as the clavicle, olecranon, radius and ulna, as well as the lower extremities (LEs), such as the patella, tibia, fibula, (bi)malleolar and foot. Postoperative follow-up…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
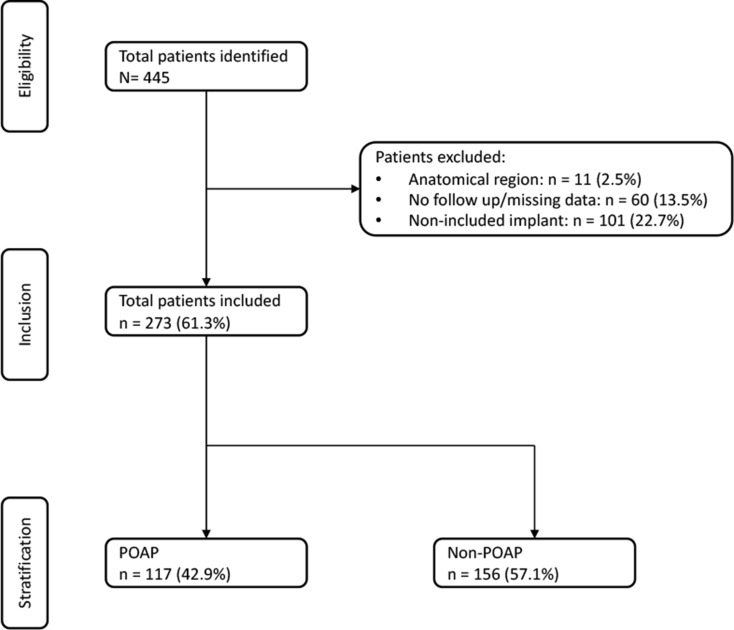 Figure 1
Figure 1- —University of Zurich
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Surgical Sutures and Adhesives · Orthopedic Infections and Treatments
Introduction
Elective implant removal (IR) is common in orthopedic surgery in industrialized countries, being performed in up to 30% of operations [1]. These operations are seen as a standard procedure; however, there are few clinical studies showing their relevance and benefit [2]. Although there are clinical guidelines regarding the indications for IR, there is still a lack of evidence-based recommendations in this regard [3]. Therefore, the decision to perform IR is highly individual and based on different indications. Patients who desire IR either show absolute indications, such as infections and non-unions, or relative indications, such as symptomatic relief; the restriction of movement and nonspecific and, sometimes, weather-dependent symptoms of discomfort. For the latter, the benefits of IR have not been consistent [4].
Postoperative complications depend on the location and type of the implant removed, and they are estimated to range from 11 to 21% [5]. Studies investigating the outcomes of hardware removal in a specific anatomical region have shown a wide range of rates for overall and specific complications [6, 7]. One of the most common complications is wound infection. Its incidence varies with the duration of surgery, the size of the surgical incision, diabetes and smoking status and other patient risk factors [8]. In the literature, an incidence rate for wound infection of up to 11% has been described [9]. Preoperative antibiotic prophylaxis (POAP) has been hypothesised to reduce incidence rates, but its clinical relevance has not yet been established. Some guidelines include POAP, but these mention its contradictory position regarding IR [10]. A 2017 study of elective IR demonstrated a modest absolute risk reduction of 1.7% for the therapy group [11]. Currently, while regional guidelines exist, there are no international standards directing the use of POAP in IR. Consequently, the implementation of POAP largely varies according to individual surgeons’ discretion [12].
Antibiotic administration can lead to adverse effects, including allergic reactions, gastrointestinal disturbances, dermatological reactions, edema and headaches, which result in higher cost and lower quality of life [13]. One of the most prominent concerns arising from antibiotic overuse is the development of multidrug-resistant bacteria. Globally speaking, the Lancet estimated 4.95 million deaths in 2022 associated with antimicrobial resistance [14].This raises a pertinent question regarding the necessity of antibiotics in IR. Therefore, the aim of this study was to explore the feasibility of omitting POAP in elective same-day surgeries for small IR in a single level I trauma centre given the possibility of wound infections.
Materials and methods
Study design
This research constitutes a retrospective, single-centre, cohort study performed at a level I trauma centre, and its documentation is aligned with the guidelines outlined in the STROBE (strengthening the reporting of observational studies in epidemiology) statement [15].
Ethical consideration
This investigation obtained approval from the cantonal ethics committee and was executed in strict adherence with the principles delineated in the Declaration of Helsinki (PB_2016_01888). Only patients who provided written consent were included.
Study population
Patients undergoing elective IR procedures on the upper and lower extremities between the 1 January 2016 and 31 December 2021 at the outpatient facility of a Swiss level I trauma centre were enrolled in this study. We registered all patients who presented to our outpatient clinic with a non-infected and radiologically consolidated fracture of the upper or lower extremities following open or closed reduction and internal fixation and were requesting IR. To facilitate meaningful comparisons, we chose to focus our cohort on the most frequently encountered anatomical regions for IR. These include the clavicula, olecranon, ulna, radius, patella, tibia, fibula, ankle and foot. Patients who underwent elective IR in other anatomical regions (e.g., the humerus, femur, and sacrum) were excluded from the study. Additionally, patients with Kirschner wires only, intramedullary nails, large plates (more than 10 holes), tension band wiring only and external fixators only were excluded as well. Furthermore, patients under 18 years of age; pregnant patients; patients lacking written informed consent; individuals with pre-existing infection; and patients with non-union and individuals with incomplete data, such as a missing initial operation report or missing follow-ups, were excluded from participation in this study.
Surgery and aftercare
All patients manifested radiologically consolidated fractures after open or closed reduction and internal fixation procedures were performed on either the upper or lower extremities, with a postoperative interval of at least 1 year for distal radius/ulna and olecranon fractures and typically at least 2 years for clavicle fractures. The choice between general anesthesia and regional anesthesia was determined based on the individual preferences of the patients. All patients underwent elective same-day surgery in an outpatient setting. The decision to administer preoperative antibiotic prophylaxis was based on the surgeons’ preferences. The follow-up protocol included a wound assessment 1 day postoperatively and a clinical examination with radiological evaluation 6 weeks postoperatively. In the interim period, wound care and monitoring were managed by the patients’ general practitioners or a home healthcare organization, depending on their individual capacity to manage the wound effectively.
Clinical evaluation and outcomes
Patients were examined before and after surgery. At the clinical examination and radiological control 6 weeks postoperatively, complications such as deep wound infection, wound-healing disorder, refracture, persistent bleeding, neurovascular injury, persistent pain, muscle hernia and re-hospitalisation were identified. Our primary outcomes to be assessed were deep wound infection and wound-healing disorder, examined specifically in association with the omission of POAP. The secondary outcome included the previously mentioned complications. We compared the rate of complications in the upper extremity (UE) and lower extremity (LE) groups and we investigated the association between complication and comorbidities and the demographics as well as the perioperative variables of our cohort. Of the patients receiving POAP, 98.3% were administered Cefazolin, typically at a single-shot dosage of 2 g.
Definitions
Deep wound infection was defined as redness, swelling and heat around the surgical incision; localised increased pain and tenderness; pus or other drainage from the wound; fever or systemic symptoms (general malaise or chills) and a foul odour from the wound. Deep wound infection was diagnosed based on a clinical examination and blood tests with elevated infection parameters (c-reactive protein and white blood cell count). Microbiological evidence was collected whenever possible, using either swabs or tissue samples, to confirm the presence of infection and identify the causative organism. However, specific anatomo-pathological were not applied in our diagnostic process. Wound-healing disorder was defined as a wound that was not fully closed after 6 weeks. Refracture was defined as a fracture of the bone from which the implant was removed. The fracture had to be visible on X-ray. Persistent bleeding was defined as postoperative bleeding lasting more than 2 days. Neurovascular injury was defined as the onset of postoperative paresthesia and/or the onset of inadequate arterial perfusion in the distal region. Muscle hernia was defined as a postoperative newly protruding muscle in the region of the surgical incision. Persistent pain was defined as the patient’s subjective perception of pain that lasted for more than 4 weeks. Partial IR was defined as IR in which certain components were intentionally left in place according to the treatment plan (e.g., in bimalleolar stabilization, in which only the medial material was taken out). Remaining material was defined as hardware being unintentionally retained due to breakage or other intraoperative complications.
Statistics
Statistical analyses were performed using R software [R], specifically R Core Team (2024) (R: A language and environment for statistical computing (Version 4.2). Retrieved June 18, 2024, from https://www.r-project.org/. Continuous data were expressed as means ± standard deviations, whereas categorical variables were expressed as counts and percentages. The normality of the data was assessed visually using histograms. For parametric data, unpaired student’s t-tests were used. Non-parametric data were analysed using Wilcoxon–Mann–Whitney tests. Binary categorical data were analysed using Fisher’s exact test. Odds ratios and 95% confidence intervals were estimated using conditional maximum likelihood. For non-binary categorical data, the Chi-squared test with Yates’s correction for continuity was used. Statistical significance was defined as a p-value < 0.05.
Results
Study population
We enrolled a total of 445 patients in this study, of whom 273 met our inclusion criteria. We excluded 60 patients (13.5%) due to incomplete data in their reports, 11 patients (2.5%) due to the anatomical region of the IR and 101 patients (22.7%) due to the kind of implant used (Kirschner wires, intramedullary nails, large plates, tension band wiring and external fixators). Finally, we were able to include 117 patients who underwent IR with POAP and 156 patients who underwent IR without POAP (Fig. 1). When categorized by anatomical region, we recorded 132 cases in the UE: 55 clavicle, 23 olecranon, 46 radius, and 8 ulna IR cases. In the LE, there were 141 cases in total: 36 tibia, 51 fibula, 31 ankle, 17 foot, and 6 patella IR cases.
Fig. 1. Patient selection flowchart
Patient demographics and procedural parameters
Of the 273 included patients, 153 (56%) were male, and 120 (44%) were female, with a mean age of 41.2 years (range: 17–82 years, SD = 14.5). Eighty-seven (31.9%) patients were suffering from comorbidities. The most frequently encountered comorbidities that were relevant for infections and wound-healing disorder were cardiovascular diseases (40.2%), followed by allergies (40.2%), skeletal disorders (12.6%) and metabolic diseases (4.6%). The UE and LE groups had some demographic differences (Table 1). Smoking was seen in 70 patients (25.6%). The number of smokers in the LE group was almost twice as high as in the UE group.
Table 1. Patient demographicsOverallUpper extremityLower extremityp-valueN273132141 Demographics Sex = F (%)120 (44.0)57 (43.2)63 (44.7)0.899Mean age in years (SD)41.2 (14.5)41.3 (14.7)41.0 (14.3)0.866Comorbidities = Yes (%)87 (31.9)39 (29.5)48 (34.0)0.505Smoking = Yes (%)70 (25.6)24 (18.2)46 (32.6)0.01n number, F female, SD standard deviation
Perioperative variables
The mean duration of surgery was 32.8 min (range: 3–165 min, SD = 18.7). The mean surgical duration of IR in the UE group was over 10 min longer than in the LE group.
In the UE group, regional anesthesia was used four times more often. Another difference was the application of preoperative antibiotic prophylaxis, which was based on the surgeons’ preferences. In the UE group, 45 (34.1%) patients received POAP, as compared to 72 (51.1%) in the LE group. Consequently, doctors were 2.01 times more likely to use POAP in the lower extremities. Partial IR was performed in 38.6% in the LE group and in 7.6% in the UE group (Table 2).
Table 2. Perioperative variablesOverallUpper extremityLower extremityp-value Perioperative variables Type of anesthesia = regional (%)33 (12.1)27 (20.5)6 (4.3)< 0.001POAP = Yes (%)117 (42.9)45 (34.1)72 (51.1)0.007Partial IR = Yes (%)64 (23.5)10 (7.6)54 (38.6)< 0.001Mean duration of surgery in minutes (SD)32.8 (18.7)38.7 (15.8)27.4 (19.7)< 0.001
Postoperative outcome
In the UE group, nine patients (6.8%) experienced persistent pain, one (0.8%) had persistent bleeding, three (2.3%) developed wound-healing disorders, one (0.8%) presented with a muscle hernia and three (2.3%) suffered from refractures; however, no neurovascular injuries were observed. All refractures occurred in the clavicle, resulting in a clavicle refracture rate of 5.5%. In the LE group, 17 patients (12.1%) reported persistent pain, five (3.5%) experienced persistent bleeding, eight (5.7%) had wound-healing disorders, there were no cases of muscle hernia and there was one (0.7%) case of neurovascular injury and no refractures (Table 3).
Table 3. Postoperative outcomeOverallUpper extremityLower extremityp-value Postoperative Outcome Complication = Yes (%)21 (7.7)8 (6.1)13 (9.2)0.452Wound-healing disorder = Yes (%)11 (4.0)3 (2.3)8 (5.7)0.263Persistent bleeding = Yes (%)6 (2.2)1 (0.8)5 (3.5)0.247Persistent pain = Yes (%)26 (9.5)9 (6.8)17 (12.1)0.205Muscle hernia = Yes (%)1 (0.4)1 (0.8)0 (0.0)Neurovascular injury = Yes (%)1 (0.4)0 (0.0)1 (0.7)Refracture = Yes (%)3 (1.1)3 (2.3)0 (0.0)0.223
A 10% lower rate of comorbidities relevant for wound healing in patients who received POAP can be detected as compared to those who did not (p = 0.08). The distributions of sex, age and smoking status were similar between the two groups. The duration of surgery and the rates of wound-healing disorder and refracture were also comparable in both groups. The postoperative outcomes in the POAP and non-POAP groups only differed by more than 1% for persistent pain, with 12.8% of patients in the POAP group suffering from persistent pain, as compared to 7.1% in the non-POAP group (p = 0.16). No patients in either the POAP or the non-POAP group developed deep wound infections. In the POAP group, five patients (4.3%) suffered from a wound-healing disorder, while six patients (3.8%) in the non-POAP group did (p = 1). Other factors, such as smoking and comorbidities, were not associated with wound issues. Persistent bleeding was present in 3.2% in the POAP group compared to 0.9% in the group without POAP (Table 4).
Table 4. Primary outcomeOverallNon-POAPPOAPp-valueSex = F (%)120 (44.0)67 (42.9)53 (45.3)0.792Mean age in years (SD)41.2 (14.5)39.46 (13.57)43.48 (15.47)0.023Smoking = Yes (%)70 (25.6)39 (25.0)31 (26.5)0.889Mean duration of surgery in minutes (SD)32.8 (18.7)30.85 (14.30)35.49 (23.20)0.043Comorbidities = Yes (%)87 (31.9)57 (36.5)30 (25.6)0.075Wound-healing disorder = Yes (%)11 (4.0)6 (3.8)5 (4.3)1Refracture = Yes (%)3 (1.1)2 (1.3)1 (0.9)1Persistent pain = Yes (%)26 (9.5)11 (7.1)15 (12.8)0.162Deep wound infection = No (%)273 (100.0)156 (100.0)117 (100.0)Persistent bleeding = Yes (%)6 (2.2)5 (3.2)1 (0.9)0.371
Secondary outcomes
We found that in 31.0% of the operations performed by residents, POAP was used. In comparison, senior consultants used POAP in 79.1% of the operations. Thus, senior consultants were more likely to use POAP (odds ratio: 8.32). The mean duration of surgery led by senior consultants was 36.9 min, while that of residents was 31.5 min. Both groups performed surgery on the lower extremities in approximately half of cases and exhibited similar rates of partial IR post-surgery. However, senior consultants were 2.5 times more likely to leave remaining material in the surgical site.
The number of partial IR in patients without POAP was 24 (15.4%), as compared to 40 (34.5%) in the POAP group. Doctors were 2.88 times more likely to use POAP in partial IR.
Discussion
Preoperative antibiotic prophylaxis is commonly used in IR to prevent wound infections, although its use remains controversial. Studies have yielded conflicting evidence regarding the effectiveness of prophylaxis [11, 12, 16]. First-generation cephalosporins are commonly used for this prophylaxis, as they effectively penetrate bone and muscle [17, 18]. While many studies have focused on comparing various antibiotics for prophylactic use in orthopedics [19, 20], few studies have specifically addressed whether such prophylaxis should be routinely used, especially in IR. The side effects of antibiotics can be serious, ranging from skin rash, eosinophilia and diarrhea to acute kidney damage. Dermatologic reactions occurred in 1 to 5% of cases, eosinophilia in 3 to 10%, leukopenia in 1 to 2%, diarrhea in 1 to 10% and kidney damage in 8 to 13%, as reported in various studies [17, 21–23]. Thus, our aim was to determine whether the withholding of POAP in elective, simple IR significantly increases wound infections as compared to elective IR with POAP.
Our key results are as follows:
- POAP does not have a significant effect on deep wound infections and wound-healing disorders when used for patients with minor IR.
- The use of POAP was significantly higher in the LE group as compared to the UE group.
Other studies have reported wound infection rates for IR ranging from 3.0% [24] to 14.9% [9, 11]. These findings are consistent with our results, which showed an overall wound infection rate of 4.0%. Specifically, wound-healing disorders accounted for 4.0% of cases, while deep wound infections were not observed.The infection rate is influenced by various factors, such as patient comorbidities, smoking status, age and the duration of surgery [25, 26]. Additionally, factors regarding hygiene in and the sterility of the operation room also play crucial roles in determining the risk of postoperative infections [27].
Our results show a low percentage of infections (4.0%), which may be attributed to the high standard of equipment, sound operating room protocols and the strict hygiene measures of the surgical team. Another factor could be the careful selection of patients, as multimorbid patients were not included in our study, as they were operated in another setting. Additionally, we excluded cases involving intramedullary nails, large plates and external fixators, focusing exclusively on small IR, as these patients were managed in an inpatient setting and subject to a different billing process. This selection criterion may contribute to the low infection rate observed in our study.
Regarding our primary objective of assessing wound infections, with a specific focus on their association with the omission of POAP, Redais et al. [24] conducted a study involving 965 patients to evaluate the efficiency of antibiotic prophylaxis in preventing surgical site infection following IR. They found a significant difference in infection rates: the group that received POAP had an infection rate of 3.0%, as compared to 11.1% in the group without POAP. In contrast, Backes et al. [11], who included 477 patients in their study, did not observe a significant difference between groups, with infection rates of 13.2% for those who underwent POAP and 14.0% for those who did not. Few randomised controlled trials address this topic, as demonstrated by Rather et al. [28].
Our study results align with the findings of Backes et al. [11], revealing a wound infection rate of 4.3% in the POAP group and 3.8% in the group without POAP. This suggests that while POAP may slightly reduce infection rates, the difference observed in our study is not substantial enough to establish a significant impact. These findings contribute to the ongoing debate on the effectiveness of prophylactic antibiotics in preventing wound infections post-surgery, highlighting the need for further research to establish clear guidelines.
Regarding our secondary outcome, we examined the use of POAP based on the skill and experience of the operating surgeon, comparing residents to senior consultants. Residents used POAP in 31.0% of their operations, whereas senior consultants did so in 79.1% of cases. We found that senior consultants were more likely to use POAP. The senior consultants may have been handling more complex IRs due to their higher skill and experience levels, necessitating the use of POAP as a safety measure. This complexity is suggested by our data, as senior consultants led more surgeries with retained screws and had longer operation durations on average. However, other factors contributing to this complexity could not be identified in our analysis. To the best of our knowledge, we have not identified any studies conducted on this specific topic.
Examining the use of POAP in patients with partial IR, we observed a significantly higher rate of POAP administration. Surgeons were 2.9 times more likely to use POAP in cases in which the implants were only partially removed (p-value < 0.001). Furthermore, when the patient was older and the operation lasted longer, surgeons were more likely to use POAP. These findings, in conjunction with the higher likelihood of POAP use among senior consultants, suggest that these operations were more complex, thereby necessitating the use of POAP. When comparing the administration of POAP in the UE and LE groups, we found that in the UE group, 34.1% of patients received POAP, while in LE group, 51.1% of patients did. Therefore, surgeons were twice as likely to use POAP in IR for the LE group.
While scientific literature does not cover this area specifically, it describes wound infection and complication rates in the context of the LEs and UEs [9, 11, 29]. Regarding IR, Backes et al. [9] found wound infection rates of 5.5% in the UEs and 12.5% in the LEs. Dong et al. [30] reported a 7.3% wound infection rate in the UEs, while Backes et al. [11] found a 14.0% wound infection rate in the LEs. Our findings show a 2.3% wound infection rate in the UEs and a 5.7% rate in the LEs, which are lower than those in the recent literature but suggest the same trend.
When examining the higher rate of wound infections in the LEs, several factors may contribute: thin layers of tissue, greater strain on the skin, challenges related to rest and activity and enhanced blood circulation due to exercise aids during regeneration [31, 32]. However, pain may prevent patients from walking and, consequently, engaging in exercise. Additionally, many patients suffer from chronic venous insufficiency, which impairs functional blood circulation and, thus, may hinder wound healing, potentially increasing the risk of infection [33]. This may explain why POAP was used more frequently in the LEs. Overall, our findings indicate that the elective IR of small plates is a safe procedure and produces few wound infections with or without POAP.
Strengths
In this study, we were able to include a large sample with relatively large subgroups for the UEs and LEs. The same goes for the various subgroups of the UE and LE groups. In our sample, the homogeneity of the patients was high. Furthermore, the data were collected during a standardised follow-up period of 6 weeks postoperatively, ensuring consistency in outcome assessments. The follow-up evaluations were conducted by experienced trauma surgeons, which enhanced the quality and accuracy of the clinical assessment and documentation.
Limitations
Several limitations must be acknowledged. The admission of POAP was depending on the surgeons’ preference, which is a strong limitation. Additionally, this is a retrospective, single-centre, cohort study, which inherently carries the risk of selection bias. Notably, multimorbid patients were operated on an in-hospital setting, potentially leading to the underestimation of infection and overall complication rates. Moreover, because documentation beyond 6 weeks was not collected, complications arising later were not detected. Additionally, the single-centre design prevents the generalisation of our findings to other institutions with differing patient demographics and clinical practices.
Conclusion
When analysing patients with uncomplicated IR, we found in this study that the use of POAP has no significant impact on the incidence of deep wound infections or wound-healing disorders. Therefore, the administration of POAP should not be routine but, rather, carefully considered based on the anticipated complexity of an IR procedure. This supports the recommendation to discontinue the use of POAP in cases where IR is anticipated to be straightforward. Particularly in LE procedures, in which our data and similar research indicate high infection rates, it is crucial to thoroughly assess the risk of infection. Factors such as the expected complexity of a surgery, the anatomical site involved and the presence of comorbidities must be evaluated before deciding whether to administer POAP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Neu HC. Cephalosporin antibiotics as applied in surgery of bones and joints. Clin Orthop Relat Res. 1984(190):50–64.6386261 · pubmed ↗
- 2Brimmo AT, Glia A, Barajas-Gamboa JS, Abril C, Rodríguez J, Kroh M, et al. Ventilation-based strategy to manage intraoperative aerosol viral transmission in the era of SARS-Co V-2. Life (Basel). 2024;14(3). 10.3390/life 14030313.10.3390/life 14030313 PMC 1097081338541639 · doi ↗ · pubmed ↗